
1 October 2, 2018 Corporate Presentation Issuer Free Writing Prospectus Filed pursuant to Rule 433 Registration Number 333 - 227400 October 2, 2018
2 Forward - Looking Statements This presentation includes forward - looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 , as amended, on Synthetic Biologics’ current expectations and projections about future events . In some cases forward - looking statements can be identified by terminology such as "may," "should," "potential," "continue," "expects," "anticipates," "intends," "plans," "believes,“ "estimates,” “indicates,” and similar expressions . These statements are based upon management’s current beliefs, expectations and assumptions and are subject to a number of risks and uncertainties, many of which are difficult to predict and include statements regarding our timeline for our SYN - 004 (ribaxamase) and SYN - 010 clinical trials and reporting of data, the size of the market, benefits to be derived from use of SYN - 004 (ribaxamase) and SYN - 010 , our anticipated patent portfolio, and our execution of our growth strategy . The forward - looking statements are subject to risks and uncertainties that could cause actual results to differ materially from those set forth or implied by any forward - looking statements . Important factors that could cause actual results to differ materially from those reflected in Synthetic Biologics’ forward - looking statements include, among others, our product candidates demonstrating safety and effectiveness, as well as results that are consistent with prior results, our ability to initiate clinical trials and if initiated, our ability to complete them on time and achieve the desired results and benefits, our clinical trials continuing enrollment as expected, our ability to obtain regulatory approval for our commercialization of product candidates or to comply with ongoing regulatory requirements, regulatory limitations relating to our ability to promote or commercialize our product candidates for the specific indications, acceptance of our product candidates in the marketplace and the successful development, marketing or sale of our products, developments by competitors that render our products obsolete or non - competitive, our ability to maintain our license agreements, the continued maintenance and growth of our patent estate, our ability to become or remain profitable, our ability to establish and maintain collaborations, our ability to obtain or maintain the capital or grants necessary to fund our research and development activities, a loss of any of our key scientists or management personnel, and other factors described in Synthetic Biologics’ annual report on Form 10 - K for the year ended December 31 , 2017 , subsequent quarterly reports on Form 10 - Qs and any other filings we make with the SEC . The information in this presentation is provided only as of the date presented, and Synthetic Biologics undertakes no obligation to update any forward - looking statements contained in this presentation on account of new information, future events, or otherwise, except as required by law .
3 Free Writing Prospectus Statement This presentation highlights basic information about us and the offering. Because it is a summary, it does not contain all of the information that you should consider before investing. We have filed a registration statement (including a preliminary prospectus) with the SEC for the offering to which this presentation relates. The registration statement has not yet become effective. Before you invest, you should read the preliminary prospectus in the registration statement (including the risk factors described therein) and other documents we have filed with the SEC for more complete information about us and the offering. You may access these documents for free by visiting EDGAR on the SEC Web site at http://www.sec.gov. The preliminary prospectus, dated October 2, 2018, is available on the SEC Web site at http://www.sec.gov. Alternatively, we or any underwriter participating in the offering will arrange to send you the prospectus if you contact A.G.P./Alliance Global Partners, 590 Madison Avenue, 36th Floor, New York, NY 10022 or via telephone at 212 - 624 - 2006 or email: prospectus@allianceg.com . This presentation shall not constitute an offer to sell, or the solicitation of an offer to buy, nor will there be any sale o f these securities in any state or other jurisdiction in which such offer, solicitation or sale would be unlawful prior to the registration or qualification under the securities laws of such state or jurisdiction. The offering will only be made by means of a prospectus pursuant to a registration statement that is filed with the SEC after such registration statement becomes effective.
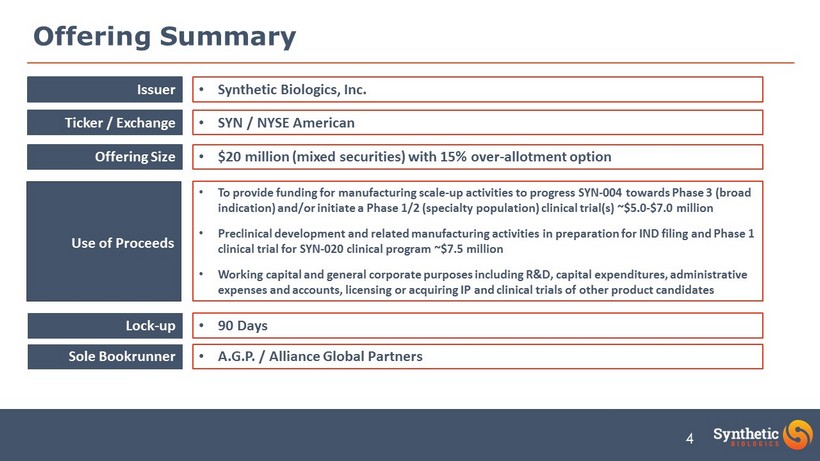
4 Offering Summary Issuer Ticker / Exchange Offering Size Use of Proceeds Lock - up Sole Bookrunner • Synthetic Biologics, Inc. • SYN / NYSE American • $20 million (mixed securities) with 15% over - allotment option • To provide funding for manufacturing scale - up activities to progress SYN - 004 towards Phase 3 (broad indication) and/or initiate a Phase 1/2 (specialty population) clinical trial(s) ~$5.0 - $7.0 million • Preclinical development and related manufacturing activities in preparation for IND filing and Phase 1 clinical trial for SYN - 020 clinical program ~$7.5 million • Working capital and general corporate purposes including R&D, capital expenditures, administrative expenses and accounts, licensing or acquiring IP and clinical trials of other product candidates • 90 Days • A.G.P. / Alliance Global Partners

5 Our Leadership Team Steven Shallcross, Interim CEO & CFO Vanda Pharmaceuticals, Inc., Empire Petroleum Partners, LLC, Innocoll AG (formerly privately held Innocoll Holdings, Inc.) Joseph Sliman, MD, MPH, CMO Vanda Pharmaceuticals, Inc., MedImmune , Inc., DynPort Vaccine Raymond Stapleton, PhD, SVP, Manufacturing Merck & Co., Inc. Michael Kaleko, MD, PhD, SVP R&D Genetic Therapy, Inc. (Novartis), Advanced Vision Therapies (currently known as Wellstat Ophthalmics ) Deb Mathews, PharmD, VP Medical Affairs Bayer Healthcare Pharmaceuticals, Novartis Vince Wacher, PhD, Product Development & Partnering Verva Pharmaceuticals Ltd.
6 About Synthetic Biologics • Diversified microbiome - focused company pioneering proprietary early & late - stage product candidates designed to protect and preserve the gut microbiome: • SYN - 004 (ribaxamase), for the prevention of antibiotic - mediated primary C. difficile infection (CDI), pathogenic overgrowth and antimicrobial resistance (AMR); • SYN - 010 , for the treatment of an underlying cause of irritable bowel syndrome with constipation (IBS - C); and, • SYN - 020 , potential to treat multiple GI & systemic diseases that stem from GI inflammation and “leaky gut” • Targeting large unmet medical needs and significant market opportunity in the prevention of bacterial infections and the treatment of GI disorders by harnessing the potential of the gut microbiome • Developing robust pipeline of product candidates leveraging proprietary formulations • Expanding intellectual property estate protecting platform product candidates • Exploring traditional and innovative paths to market
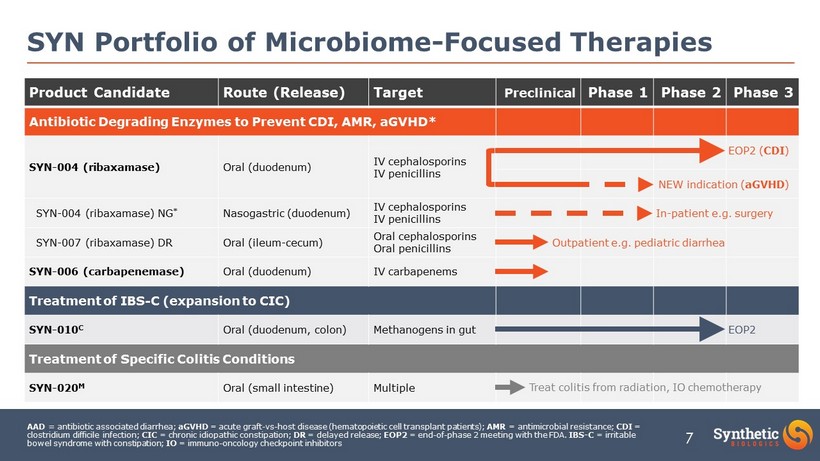
7 AAD = antibiotic associated diarrhea; aGVHD = acute graft - vs - host disease (hematopoietic cell transplant patients); AMR = antimicrobial resistance; CDI = clostridium difficile infection; CIC = chronic idiopathic constipation; DR = delayed release; EOP2 = end - of - phase 2 meeting with the FDA. IBS - C = irritable bowel syndrome with constipation; IO = immuno - oncology checkpoint inhibitors SYN Portfolio of Microbiome - Focused Therapies Product Candidate Route (Release) Target Preclinical Phase 1 Phase 2 Phase 3 Antibiotic Degrading Enzymes to Prevent CDI, AMR, aGVHD* SYN - 004 (ribaxamase) Oral (duodenum) IV cephalosporins IV penicillins SYN - 004 (ribaxamase) NG * Nasogastric (duodenum) IV cephalosporins IV penicillins SYN - 007 (ribaxamase) DR Oral (ileum - cecum) Oral cephalosporins Oral penicillins SYN - 006 (carbapenemase) Oral (duodenum) IV carbapenems Treatment of IBS - C (expansion to CIC) SYN - 010 C Oral (duodenum, colon) Methanogens in gut Treatment of Specific Colitis Conditions SYN - 020 M Oral (small intestine) Multiple Outpatient e.g. pediatric diarrhea In - patient e.g. surgery EOP2 ( CDI ) Treat colitis from radiation, IO chemotherapy EOP2 NEW indication ( aGVHD )
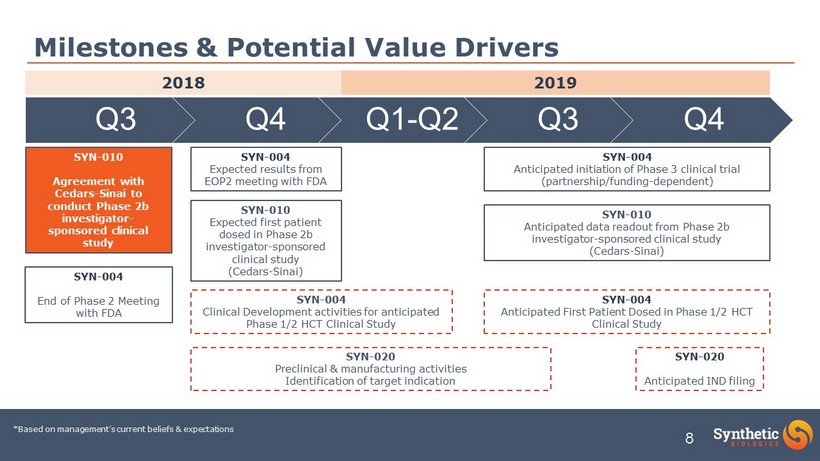
8 Q3 Q4 Q1 - Q2 Q3 Q4 Milestones & Potential Value Drivers 2018 2019 SYN - 010 Agreement with Cedars - Sinai to conduct Phase 2b investigator - sponsored clinical study SYN - 010 Expected first patient dosed in Phase 2b investigator - sponsored clinical study (Cedars - Sinai) SYN - 004 Expected results from EOP2 meeting with FDA SYN - 004 End of Phase 2 Meeting with FDA SYN - 020 Anticipated IND filing SYN - 010 Anticipated data readout from Phase 2b investigator - sponsored clinical study (Cedars - Sinai) SYN - 004 Anticipated initiation of Phase 3 clinical trial (partnership/funding - dependent) SYN - 004 Clinical Development activities for anticipated Phase 1/2 HCT Clinical Study SYN - 004 Anticipated First Patient Dosed in Phase 1/2 HCT Clinical Study SYN - 020 Preclinical & manufacturing activities Identification of target indication *Based on management’s current beliefs & expectations

SYN - 004 (ribaxamase)
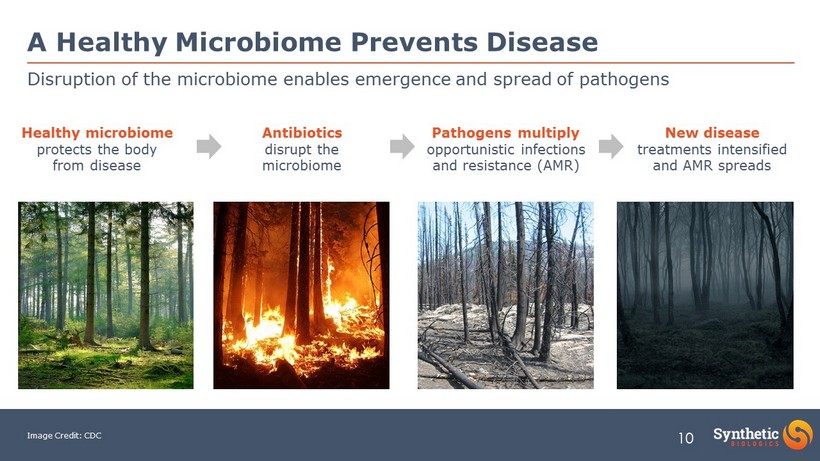
10 Healthy microbiome protects the body from disease Antibiotics disrupt the microbiome Pathogens multiply opportunistic infections and resistance (AMR) Image Credit: CDC A Healthy Microbiome Prevents Disease Disruption of the microbiome enables emergence and spread of pathogens New disease treatments intensified and AMR spreads

11 Healthy microbiome protects the body from disease Antibiotics disrupt the microbiome Image Credit: CDC A Healthy Microbiome Prevents Disease Preventing disruption of the microbiome can protect against pathogens and disease PREVENTION Synthetic Biologics Concept: Block the microbiome damaging agent Let the healthy microbiome do its work
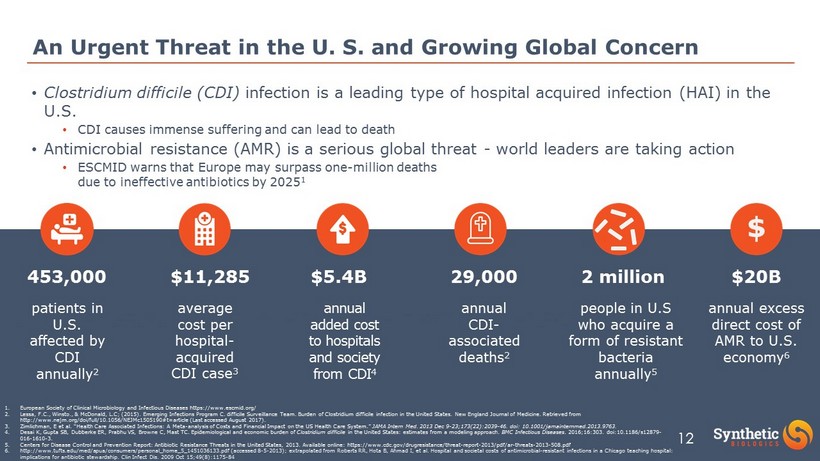
12 9. ., & McDonald, L.C; (2015). Emerging Infections Program C. difficile Surveillance Team. Burden of Clostridium difficile infec tion in the United States. New England Journal of Medicine. Retrieved from http://www.nejm.org/doi/full/10.1056/NEJMc1505190#t=a rticle (Last accessed August 2017). 10. e, E van et al. “Excess length of stay and mortality due to Clostridium difficile infection: a multi - state modelling approac h.” The Journal of hospital infection 88 4 (2014): 213 - 7. DOI: 10.1016/j.jhin.2014.08.008 11. Desai K, Gupta SB, Dubberke ER, Prahu VS, Browne C, Mast TC. Epidemiological and economic burden of Clostridium difficile in the United States: estimates from a modeling approach. BMC Infectious Diseases . 2016;16:303. doi:10.1186/s12879 - 016 - 1610 - 3. An Urgent Threat in the U. S. and Growing Global Concern average cost per hospital - acquired CDI case 3 patients in U.S. affected by CDI annually 2 453,000 $11,285 annual added cost to hospitals and society from CDI 4 $5.4B annual CDI - associated deaths 2 29,000 1. European Society of Clinical Microbiology and Infectious Diseases https://www.escmid.org/ 2. Lessa , F.C., Winsto ., & McDonald, L.C; (2015). Emerging Infections Program C. difficile Surveillance Team. Burden of Clostridium difficile infectio n in the United States. New England Journal of Medicine. Retrieved from http://www.nejm.org/doi/full/10.1056/NEJMc1505190#t=article (Last accessed August 2017). 3. Zimlichman , E et al. “Health Care Associated Infections: A Meta - analysis of Costs and Financial Impact on the US Health Care System.” JAMA Intern Med. 2013 Dec 9 - 23;173(22):2039 - 46. doi : 10.1001/jamainternmed.2013.9763. 4. Desai K, Gupta SB, Dubberke ER, Prabhu VS, Browne C, Mast TC. Epidemiological and economic burden of Clostridium difficile in the United States: estimates from a modeling approach. BMC Infectious Diseases . 2016;16:303. doi:10.1186/s12879 - 016 - 1610 - 3. 5. Centers for Disease Control and Prevention Report: Antibiotic Resistance Threats in the United States, 2013. Available online : h ttps://www.cdc.gov/drugresistance/threat - report - 2013/pdf/ar - threats - 2013 - 508.pdf 6. http://www.tufts.edu/med/apua/consumers/personal_home_5_1451036133.pdf (accessed 8 - 5 - 2013); extrapolated from Roberts RR, Hota B, Ahmad I, et al. Hospital and societal costs of antimicrobial - resistant infections in a Chicago teaching hospital: implications for antibiotic stewardship. Clin Infect Dis. 2009 Oct 15;49(8):1175 - 84 2 million people in U.S who acquire a form of resistant bacteria annually 5 annual excess direct cost of AMR to U.S. economy 6 $ $20B • Clostridium difficile (CDI) infection is a leading type of hospital acquired infection (HAI) in the U.S. • CDI causes immense suffering and can lead to death • Antimicrobial resistance (AMR) is a serious global threat - world leaders are taking action • ESCMID warns that Europe may surpass one - million deaths due to ineffective antibiotics by 2025 1
13 • Two proprietary oral 75mg capsules (custom designed oral β - lactamase) • Designed to protect the natural balance of microbes in the gut microbiome during antibiotic use • Did not interfere with the efficacy of IV antibiotics in Phase 2 studies SYN - 004 (ribaxamase) • be co - administered with certain IV antibiotics • b reak down excess IV antibiotic excreted into the GI tract • h elp prevent C lostridium difficile infection (C DI ) , pathogen overgrowth and the emergence of antimicrobial resistance ( AMR ) What is ribaxamase? Ribaxamase is designed to:
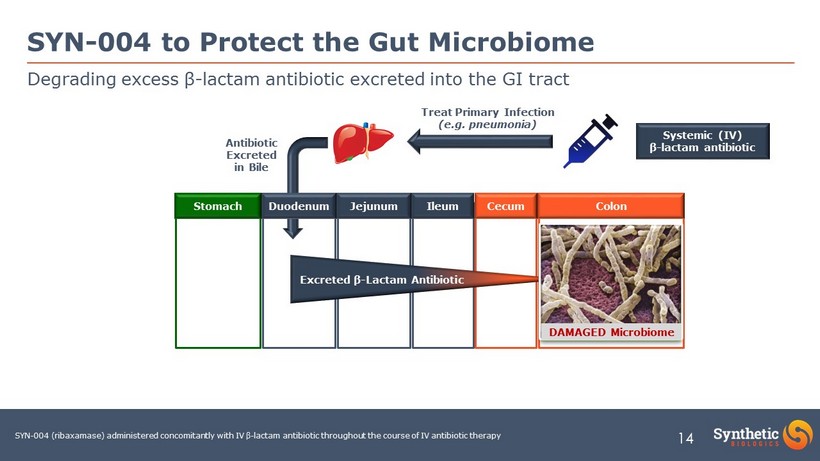
14 Degrading excess β - lactam antibiotic excreted into the GI tract SYN - 004 to Protect the Gut Microbiome Antibiotic Excreted in Bile Systemic (IV) β - lactam antibiotic Treat Primary Infection (e.g. pneumonia) Stomach Duodenum Jejunum Ileum Cecum Colon Excreted β - Lactam Antibiotic SYN - 004 (ribaxamase) administered concomitantly with IV β - lactam antibiotic throughout the course of IV antibiotic therapy Healthy Microbiome DAMAGED Microbiome
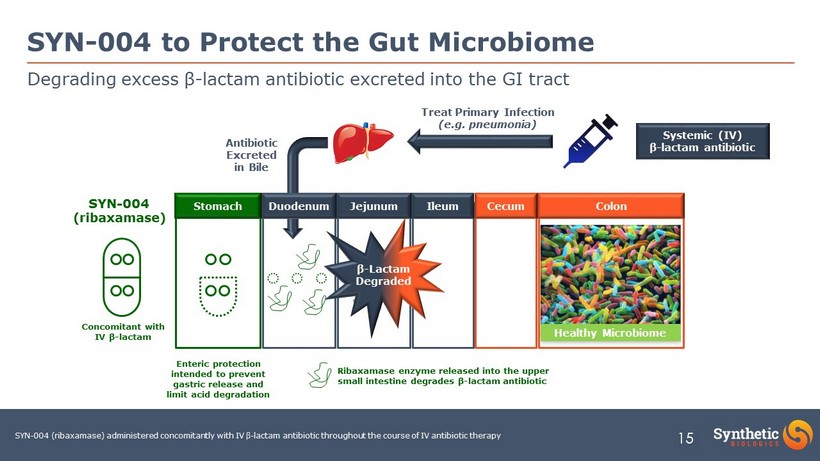
15 Degrading excess β - lactam antibiotic excreted into the GI tract SYN - 004 to Protect the Gut Microbiome SYN - 004 (ribaxamase) Antibiotic Excreted in Bile Systemic (IV) β - lactam antibiotic Treat Primary Infection (e.g. pneumonia) Stomach Duodenum Jejunum Ileum Cecum Colon Enteric protection intended to prevent gastric release and limit acid degradation Ribaxamase enzyme released into the upper small intestine degrades β - lactam antibiotic SYN - 004 (ribaxamase) administered concomitantly with IV β - lactam antibiotic throughout the course of IV antibiotic therapy Concomitant with IV β - lactam β - Lactam Degraded Healthy Microbiome
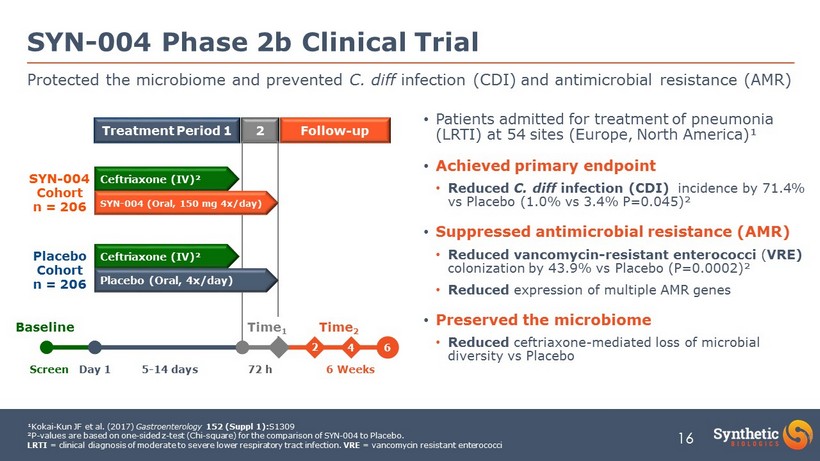
16 • Patients admitted for treatment of pneumonia (LRTI) at 54 sites (Europe, North America)¹ • Achieved primary endpoint • Reduced C. diff infection (CDI) incidence by 71.4% vs Placebo (1.0% vs 3.4% P=0.045)² • Suppressed antimicrobial resistance (AMR) • Reduced vancomycin - resistant enterococci ( VRE) colonization by 43.9% vs Placebo (P=0.0002)² • Reduced expression of multiple AMR genes • Preserved the microbiome • Reduced ceftriaxone - mediated loss of microbial diversity vs Placebo SYN - 004 Phase 2b Clinical Trial Protected the microbiome and prevented C. diff infection (CDI) and antimicrobial resistance (AMR) 16 ¹Kokai - Kun JF et al. (2017) Gastroenterology 152 (Suppl 1): S1309 ²P - values are based on one - sided z - test (Chi - square) for the comparison of SYN - 004 to Placebo. LRTI = clinical diagnosis of moderate to severe lower respiratory tract infection. VRE = vancomycin resistant enterococci Treatment Period 1 Follow - up 2 Screen Day 1 5 - 14 days 72 h 6 Weeks SYN - 004 Cohort n = 206 Placebo Cohort n = 206 Ceftriaxone (IV)² SYN - 004 (Oral, 150 mg 4x/day) Ceftriaxone (IV)² Placebo (Oral, 4x/day) Baseline 4 Time 1 Time 2 6 4 2
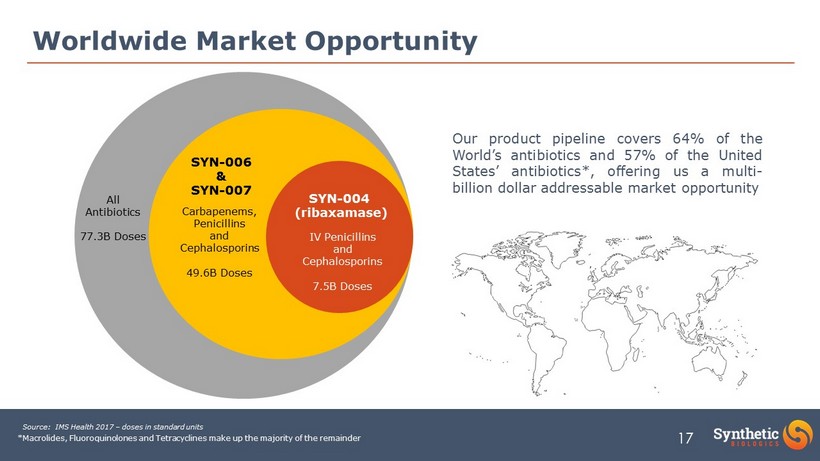
17 Worldwide Market Opportunity All Antibiotics 77.3B Doses IV Penicillins and Cephalosporins 7.5B Doses Source: IMS Health 2017 – doses in standard units Carbapenems, Penicillins and Cephalosporins 49.6B Doses Our product pipeline covers 64 % of the World’s antibiotics and 57 % of the United States’ antibiotics*, offering us a multi - billion dollar addressable market opportunity SYN - 004 (ribaxamase) SYN - 006 & SYN - 007 *Macrolides, Fluoroquinolones and Tetracyclines make up the majority of the remainder
18 • Anticipate large, global, multi - center, randomized controlled clinical trial • Primary efficacy endpoint reduction of CDI incidence in SYN - 004 vs Placebo treatment group • Co - primary safety endpoint relative risk of mortality in SYN - 004 vs Placebo treatment group • Evaluate a broad range of patients who are receiving multiple IV β - lactam antibiotics to treat different index infections (e.g. LRTI, UTI, intraabdominal) • EOP2 meeting with the FDA held in Q3 2018 • An indication in a specialized patient population may provide a more favorable clinical development opportunity and significant cost savings with a similar time - to - market • Supported by clinical outcomes from completed SYN - 004 clinical studies Broad Indication: Phase 3 clinical trial under discussion with FDA SYN - 004 Development Status CDI : Clostridium difficile infection. LRTI: lower respiratory tract infection. UTI: urinary tract infection.
19 • Prevention of acute graft - versus - host disease (aGVHD) in Allogeneic Hematopoietic Cell Transplantation (HCT) recipients • An estimated 8,539 allogeneic HCT procedures were conducted in the USA in 2016 1 • ~4,500 procedures conducted in China 2 • 80 - 90% of allogeneic HCT recipients will be treated with IV β - lactam antibiotics • Decreased microbiome diversity due to IV β - lactam antibiotics is strongly associated with aGVHD 3 • aGVHD occurs in 40 - 60% of allogeneic HCT recipients • Reduced microbiome diversity enables VRE colonization, increases fatal VRE bacteremia 4 and CDI 5 • Prevention of aGVHD in allogeneic HCT recipients is critical to patient outcomes and survival 6 ‒ First - line aGVHD therapies (steroids) fail in ≥50% of patients resulting in very poor overall survival • Phase 1/2 study to evaluate SYN - 004 PK, safety and microbiome protection in allogeneic HCT recipient • Potential Phase 3 study to evaluate ability of SYN - 004 to prevent aGVHD Evaluation of SYN - 004 in a specialty β - lactam treated patient population SYN - 004 Indication Expansion Concept 1 D’Souza A, Fretham C. Current use and outcome of hematopoietic stem cell transplantation: CIMBTR summary and slides, 2017. Available at http://www.cimbtr.org 2 Xu L - P et al. (2017) Bone Marrow Transplant 52: 1512 - 8 3 Shono Y et al. (2016) Sci Transl Med 8: 339ra71 4 Taur Y et al. (2012) Clin Infect Dis 55: 905 - 14. 5 Dubberke ER et al. (2010) Clin Transplant 24: 192 - 8. . 6 The high incidence and absence of effective therapies preclude the argument that it is cheaper to wait for patients to develop aGVHD then treat the disease (a common rebuttal when discussing CDI preven tio n).
20 Pending Patent Applications • Methods of Manufacture • Clinical Dosing, Formulation • Methods of Treatment Expires 2035/6 Patented other β - Lactamase Composition of Matter & Uses Expires 2035 Patented SYN - 004 (ribaxamase) Composition of Matter Expires 2031 Extensive patent portfolio, multiple protection strategies SYN - 004 Patent Position ¹Intellectual property owned outright by Synthetic Biologics, Inc. ~60 Granted Patents and ~55 Pending Applications (US & International)
SYN - 010
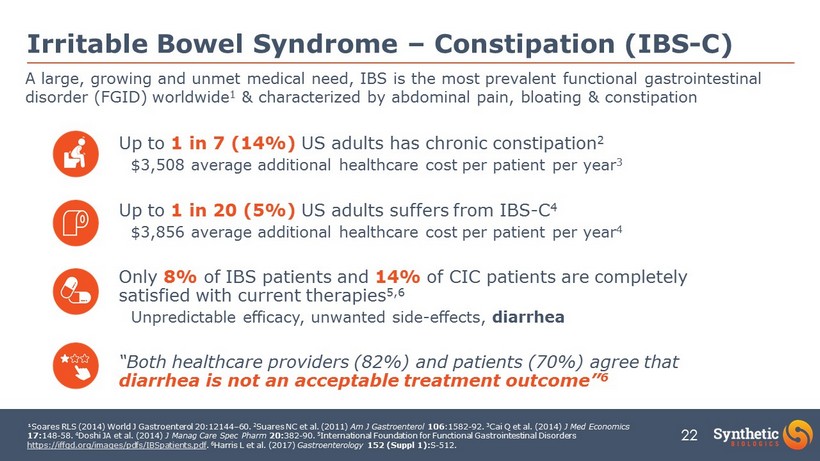
22 Irritable Bowel Syndrome – Constipation (IBS - C) Up to 1 in 7 (14%) US adults has chronic constipation 2 $3,508 average additional healthcare cost per patient per year 3 Up to 1 in 20 (5%) US adults suffers from IBS - C 4 $3,856 average additional healthcare cost per patient per year 4 Only 8% of IBS patients and 14% of CIC patients are completely satisfied with current therapies 5 ,6 Unpredictable efficacy, unwanted side - effects, diarrhea “Both healthcare providers (82%) and patients (70%) agree that diarrhea is not an acceptable treatment outcome” 6 ¹Soares RLS (2014) World J Gastroenterol 20:12144 – 60. 2 Suares NC et al. (2011) Am J Gastroenterol 106 :1582 - 92. 3 Cai Q et al. (2014) J Med Economics 17: 148 - 58. 4 Doshi JA et al. (2014) J Manag Care Spec Pharm 20: 382 - 90. 5 International Foundation for Functional Gastrointestinal Disorders https://iffgd.org/images/pdfs/IBSpatients.pdf . 6 Harris L et al. (2017) Gastroenterology 152 (Suppl 1): S - 512. A large, growing and unmet medical need, IBS is the most prevalent functional gastrointestinal disorder (FGID) worldwide 1 & characterized by abdominal pain, bloating & constipation

23 IBS and Constipation Markets are Growing More than 2x growth in 4 years! US IBS and Constipation Market 1 • Digital and DTC campaigns are enhancing awareness of both IBS and gut health • New entrants are growing the market , not cannibalizing it 1 • Only 26% of patients are “very satisfied” with current FDA approved prescription medication 2 • Current therapies have not been shown to effectively address the symptoms of pain and bloating • Significant global market opportunity $2.5B Market Growth Drivers 1. IMS Health Analytics Link custom report. (Last accessed, August 2017). Population estimates: United Nations Population Division. Department of Economic and Social Affairs. World Population Prospects: The 2015 Revision. (July 2015.); 2. American Gastroenterological Association. Irritable Bowel Syndrome in America. A Survey Report conducted by AGA. (December 2015). (Last accessed 03/19/2017).
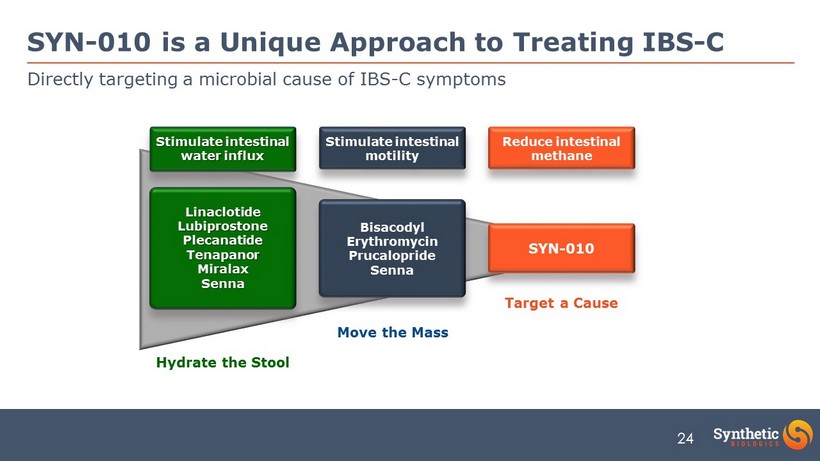
24 Directly targeting a microbial cause of IBS - C symptoms SYN - 010 is a Unique Approach to Treating IBS - C Bisacodyl Erythromycin Prucalopride Senna Linaclotide Lubiprostone Plecanatide Tenapanor Miralax Senna Target a Cause Hydrate the Stool Stimulate intestinal motility Stimulate intestinal water influx Reduce intestinal methane SYN - 010 Move the Mass
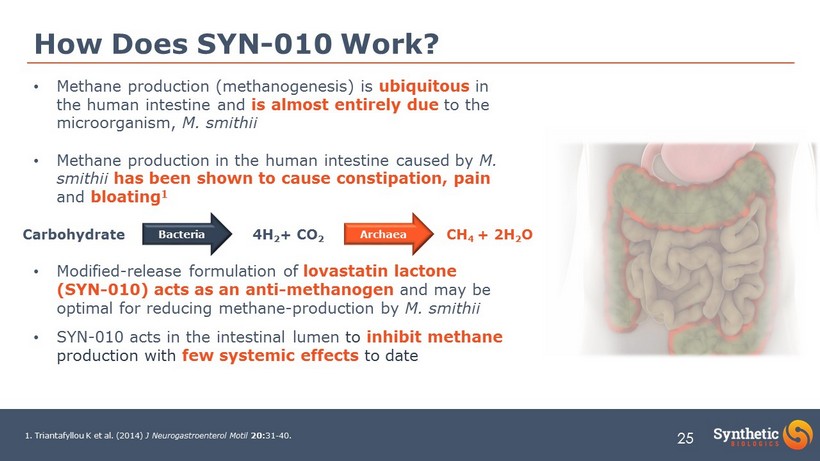
25 • Methane production (methanogenesis) is ubiquitous in the human intestine and is almost entirely due to the microorganism, M. smithii • Methane production in the human intestine caused by M. smithii has been shown to cause constipation, pain and bloating 1 • Modified - release formulation of lovastatin lactone (SYN - 010) acts as an anti - methanogen and may be optimal for reducing methane - production by M. smithii • SYN - 010 acts in the intestinal lumen to inhibit methane production with few systemic effects to date How Does SYN - 010 Work? 1. Triantafyllou K et al. (2014) J Neurogastroenterol Motil 20: 31 - 40. Bacteria Archaea Carbohydrate 4H 2 + CO 2 CH 4 + 2H 2 O
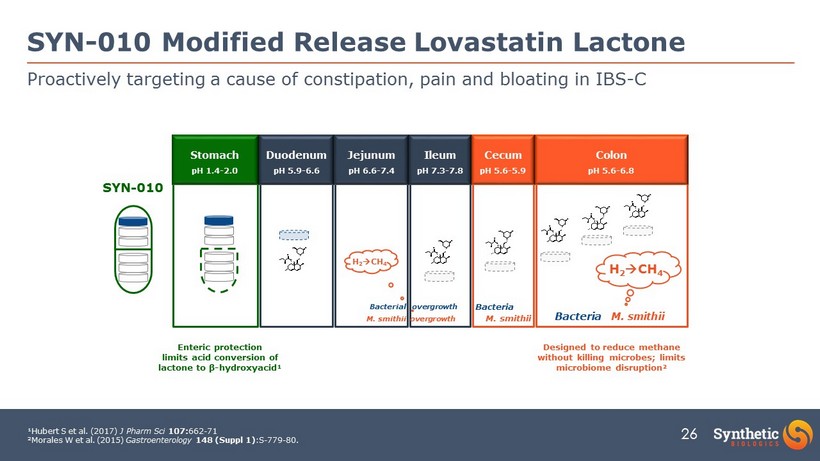
26 Proactively targeting a cause of constipation, pain and bloating in IBS - C SYN - 010 Modified Release Lovastatin Lactone SYN - 010 ¹Hubert S et al. (2017) J Pharm Sci 107: 662 - 71 ²Morales W et al. (2015) Gastroenterology 148 (Suppl 1) :S - 779 - 80. Stomach pH 1.4 - 2.0 Duodenum pH 5.9 - 6.6 Jejunum pH 6.6 - 7.4 Ileum pH 7.3 - 7.8 Cecum pH 5.6 - 5.9 Colon pH 5.6 - 6.8 O O H O OH O O O H O OH O O O H O OH O O O H O OH O O O H O OH O O O H O OH O M. smithii Bacteria M. smithii Bacteria M. smithii overgrowth Bacterial overgrowth H 2 CH 4 H 2 CH 4 Designed to reduce methane without killing microbes; limits microbiome disruption² Enteric protection limits acid conversion of lactone to β - hydroxyacid¹
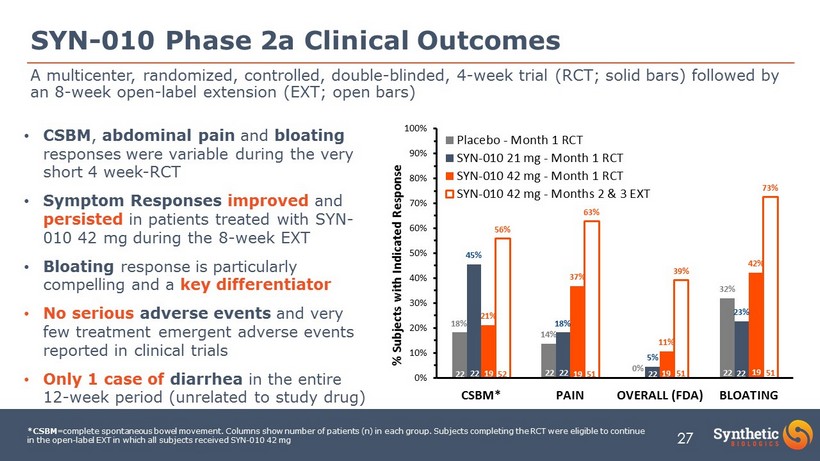
27 18% 14% 0% 32% 45% 18% 5% 23% 21% 37% 11% 42% 56% 63% 39% 73% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% CSBM* PAIN OVERALL (FDA) BLOATING % Subjects with Indicated Response Placebo - Month 1 RCT SYN-010 21 mg - Month 1 RCT SYN-010 42 mg - Month 1 RCT SYN-010 42 mg - Months 2 & 3 EXT 52 51 51 51 22 22 19 19 19 22 19 22 22 22 22 SYN - 010 Phase 2a Clinical Outcomes *CSBM =complete spontaneous bowel movement. Columns show number of patients (n) in each group. Subjects completing the RCT were eli gib le to continue in the open - label EXT in which all subjects received SYN - 010 42 mg • CSBM , abdominal pain and bloating responses were variable during the very short 4 week - RCT • Symptom Responses improved and persisted in patients treated with SYN - 010 42 mg during the 8 - week EXT • Bloating response is particularly compelling and a key differentiator • No serious adverse events and very few treatment emergent adverse events reported in clinical trials • Only 1 case of diarrhea in the entire 12 - week period (unrelated to study drug) A multicenter, randomized, controlled, double - blinded, 4 - week trial (RCT; solid bars) followed by an 8 - week open - label extension (EXT; open bars)
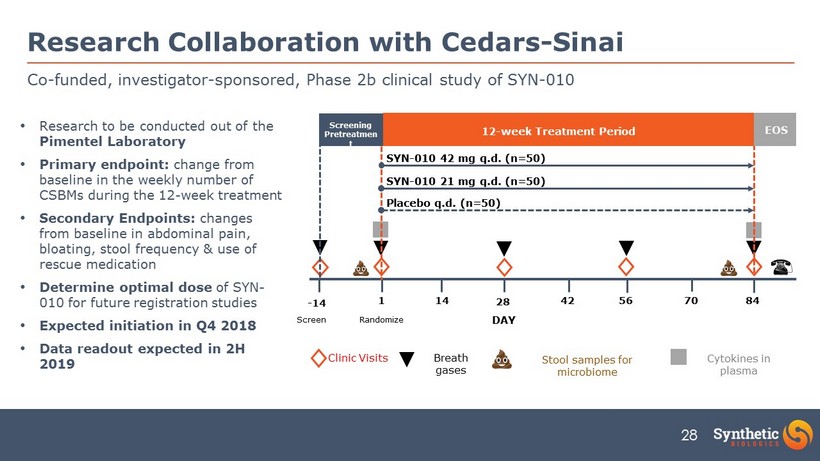
28 Co - funded, investigator - sponsored, Phase 2b clinical study of SYN - 010 Research Collaboration with Cedars - Sinai Clinic Visits Breath gases Cytokines in plasma Stool samples for microbiome - 14 1 14 28 42 56 70 84 DAY Randomize Screen Screening Pretreatmen t 12 - week Treatment Period EOS SYN - 010 42 mg q.d. (n=50) SYN - 010 21 mg q.d. (n=50) Placebo q.d. (n=50) • Research to be conducted out of the Pimentel Laboratory • Primary endpoint: change from baseline in the weekly number of CSBMs during the 12 - week treatment • Secondary Endpoints: changes from baseline in abdominal pain, bloating, stool frequency & use of rescue medication • Determine optimal dose of SYN - 010 for future registration studies • Expected initiation in Q4 2018 • Data readout expected in 2H 2019
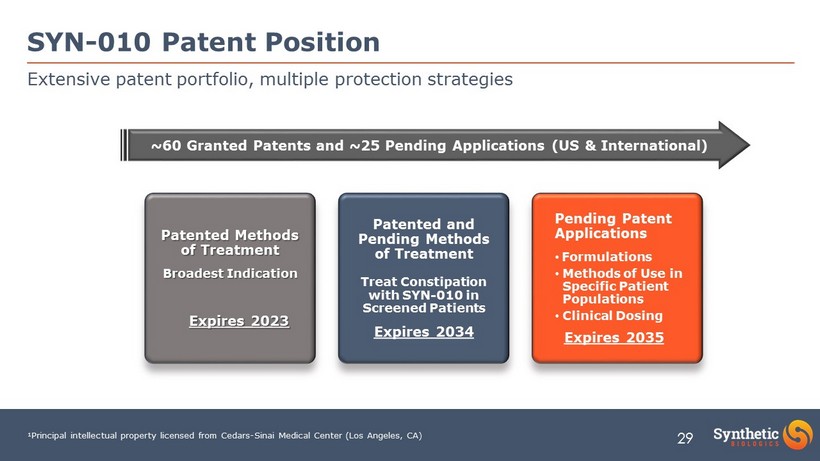
29 Pending Patent Applications • Formulations • Methods of Use in Specific Patient Populations • Clinical Dosing Expires 2035 Patented and Pending Methods of Treatment Treat Constipation with SYN - 010 in Screened Patients Expires 2034 Patented Methods of Treatment Broadest Indication Expires 2023 Extensive patent portfolio, multiple protection strategies SYN - 010 Patent Position ¹Principal intellectual property licensed from Cedars - Sinai Medical Center (Los Angeles, CA) ~60 Granted Patents and ~25 Pending Applications (US & International)

SYN - 020
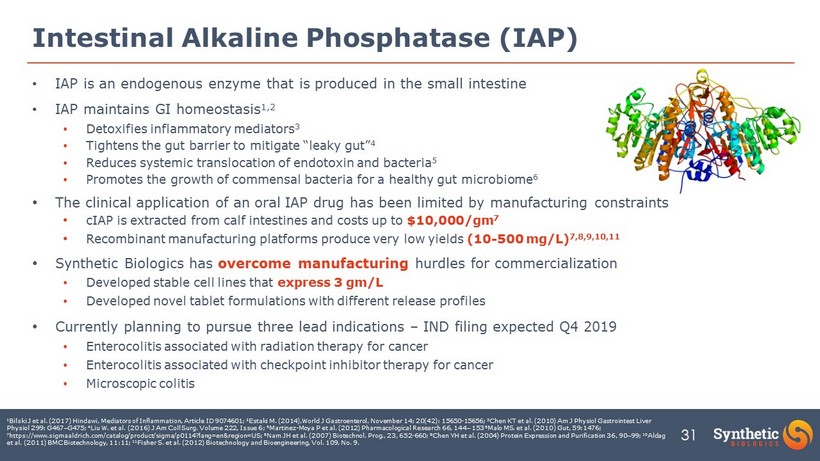
31 Intestinal Alkaline Phosphatase (IAP) • IAP is an endogenous enzyme that is produced in the small intestine • IAP maintains GI homeostasis 1,2 • Detoxifies inflammatory mediators 3 • Tightens the gut barrier to mitigate “leaky gut” 4 • Reduces systemic translocation of endotoxin and bacteria 5 • Promotes the growth of commensal bacteria for a healthy gut microbiome 6 • The clinical application of an oral IAP drug has been limited by manufacturing constraints • cIAP is extracted from calf intestines and costs up to $10,000/gm 7 • Recombinant manufacturing platforms produce very low yields (10 - 500 mg/L) 7,8,9,10,11 • Synthetic Biologics has overcome manufacturing hurdles for commercialization • Developed stable cell lines that express 3 gm/L • Developed novel tablet formulations with different release profiles • Currently planning to pursue three lead indications – IND filing expected Q4 2019 • Enterocolitis associated with radiation therapy for cancer • Enterocolitis associated with checkpoint inhibitor therapy for cancer • Microscopic colitis 1 Bilski J et al. (2017) Hindawi , Mediators of Inflammation, Article ID 9074601; 2 Estaki M. (2014), World J Gastroenterol, November 14; 20(42): 15650 - 15656; 3 Chen KT et al. (2010) Am J Physiol Gastrointest Liver Physiol 299: G467 – G475; 4 Liu W. et al. (2016) J Am Coll Surg. Volume 222, Issue 6; 5 Martinez - Moya P et al. (2012) Pharmacological Research 66, 144 – 153 6 Malo MS. et al. (2010) Gut, 59:1476; 7 https://www.sigmaaldrich.com/catalog/product/sigma/p0114?lang=en®ion=US; 8 Nam JH et al. (2007) Biotechnol. Prog., 23, 652 - 660; 9 Chen YH et al. (2004) Protein Expression and Purification 36, 90 – 99; 10 Aldag et al. (2011) BMC Biotechnology, 11:11; 11 Fisher S. et al. (2012) Biotechnology and Bioengineering, Vol. 109, No. 9.
32 • Radiation is used in 50% of cancer patients and has a role in 25% of cures 1 • Pelvic and abdominal irradiation is used >300,000 times annually in US • 60 - 80% of radiation - treated patients suffer acute bowel toxicity 1 • Estimated that 20 - 50% of survivors progress to chronic enteropathy • Significant unmet need for both acute (inflammatory) and chronic (fibrosing) syndromes • Potential Clinical Trial Concepts • Phase 1 - single & multiple ascending dose studies in healthy volunteers • Phase 2 - dose - ranging study in subjects treated with radiation for pelvic and abdominal cancers • Phase 3 - study in subjects treated with radiation for pelvic and abdominal cancers Radiation therapy secondary to cancer therapy SYN - 020 Potential Indication 32 1 Hauer - Jensen M et al. (2014) Nat Rev Gastroenterol Hepatol , 11(8): 470 – 479.
Investment Opportunity

34 Strategic Priorities • Announced key partnership with Cedars - Sinai Medical Center to advance SYN - 010 • End of Phase 2 Meeting with FDA in Q3 2018 to solidify Phase 3 clinical program for SYN - 004 • Establish cost - effective development pathway for expansion indication for SYN - 004 in specialty patient population • Advancing strategic partnership opportunities in support of development pipeline • Favorable market - access points and development opportunities in China • Recent regulatory reform intended to raise China’s drug regulations to international standards • China National Drug Administration (CNDA) now requires single Phase 3 clinical program for marketing approval • Potential to build and expand franchise of preventative products • Capital Considerations • Continue to prioritize non - dilutive forms of capital • Financial stewardship remains a top priority • Investment in high - impact clinical opportunities Focus on execution and growing shareholder value
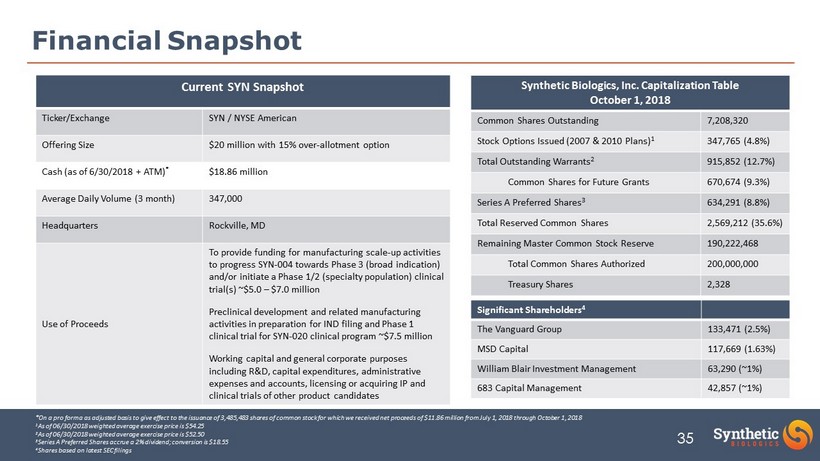
35 Financial Snapshot Synthetic Biologics, Inc. Capitalization Table October 1, 2018 Common Shares Outstanding 7,208,320 Stock Options Issued (2007 & 2010 Plans) 1 347,765 (4.8%) Total Outstanding Warrants 2 915,852 (12.7%) Common Shares for Future Grants 670,674 (9.3%) Series A Preferred Shares 3 634,291 (8.8%) Total Reserved Common Shares 2,569,212 (35.6%) Remaining Master Common Stock Reserve 190,222,468 Total Common Shares Authorized 200,000,000 Treasury Shares 2,328 *On a pro forma as adjusted basis to give effect to the issuance of 3,485,483 shares of common stock for which we received ne t p roceeds of $11.86 million from July 1, 2018 through October 1, 2018 1 As of 06/30/2018 weighted average exercise price is $54.25 2 As of 06/30/2018 weighted average exercise price is $52.50 3 Series A Preferred Shares accrue a 2% dividend; conversion is $18.55 4 Shares based on latest SEC filings Significant Shareholders 4 The Vanguard Group 133,471 (2.5%) MSD Capital 117,669 (1.63%) William Blair Investment Management 63,290 (~1%) 683 Capital Management 42,857 (~1%) Current SYN Snapshot Ticker/Exchange SYN / NYSE American Offering Size $20 million with 15% over - allotment option Cash (as of 6/30/2018 + ATM) * $18.86 million Average Daily Volume (3 month) 347,000 Headquarters Rockville, MD Use of Proceeds To provide funding for manufacturing scale - up activities to progress SYN - 004 towards Phase 3 (broad indication) and/or initiate a Phase 1/2 (specialty population) clinical trial(s) ~$5.0 – $7.0 million Preclinical development and related manufacturing activities in preparation for IND filing and Phase 1 clinical trial for SYN - 020 clinical program ~$7.5 million Working capital and general corporate purposes including R&D, capital expenditures, administrative expenses and accounts, licensing or acquiring IP and clinical trials of other product candidates
APPENDIX

SYN - 004 (ribaxamase) Expansion Programs
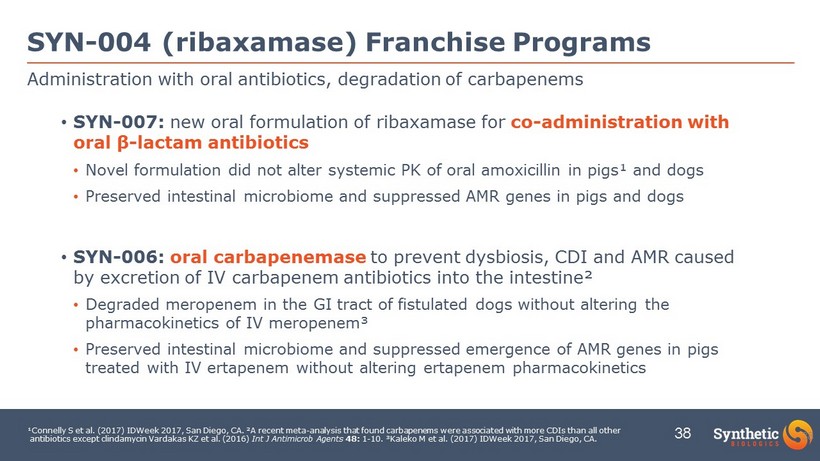
38 • SYN - 007: new oral formulation of ribaxamase for co - administration with oral β - lactam antibiotics • Novel formulation did not alter systemic PK of oral amoxicillin in pigs¹ and dogs • Preserved intestinal microbiome and suppressed AMR genes in pigs and dogs • SYN - 006: oral carbapenemase to prevent dysbiosis, CDI and AMR caused by excretion of IV carbapenem antibiotics into the intestine ² • Degraded meropenem in the GI tract of fistulated dogs without altering the pharmacokinetics of IV meropenem³ • Preserved intestinal microbiome and suppressed emergence of AMR genes in pigs treated with IV ertapenem without altering ertapenem pharmacokinetics Administration with oral antibiotics, degradation of carbapenems SYN - 004 (ribaxamase) Franchise Programs 38 ¹Connelly S et al. (2017) IDWeek 2017, San Diego, CA. ²A recent meta - analysis that found carbapenems were associated with more CDIs than all other antibiotics except clindamycin Vardakas KZ et al. (2016) Int J Antimicrob Agents 48: 1 - 10. ³Kaleko M et al. (2017) IDWeek 2017, San Diego, CA.
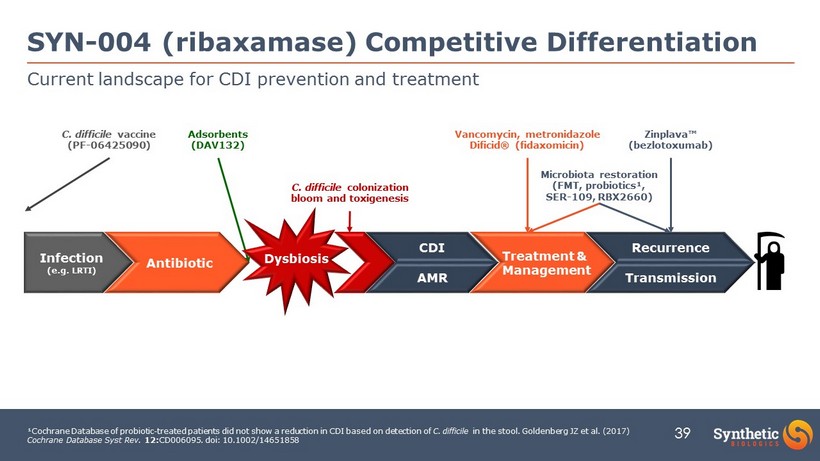
39 Dysbiosis Current landscape for CDI prevention and treatment SYN - 004 (ribaxamase) Competitive Differentiation Infection (e.g. LRTI) Antibiotic Treatment & Management Recurrence Transmission C. difficile colonization bloom and toxigenesis ¹Cochrane Database of probiotic - treated patients did not show a reduction in CDI based on detection of C. difficile in the stool. Goldenberg JZ et al. (2017) Cochrane Database Syst Rev. 12: CD006095. doi : 10.1002/14651858 CDI AMR Zinplava ™ ( bezlotoxumab ) Microbiota restoration (FMT, probiotics¹, SER - 109, RBX2660) Vancomycin, metronidazole Dificid ® (fidaxomicin) C. difficile vaccine (PF - 06425090) Adsorbents (DAV132)
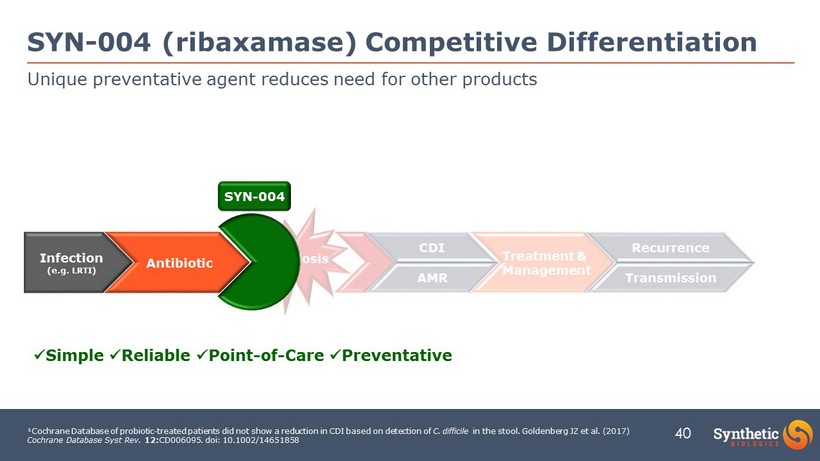
40 Dysbiosis Unique preventative agent reduces need for other products SYN - 004 (ribaxamase) Competitive Differentiation Infection (e.g. LRTI) Antibiotic Treatment & Management Recurrence Transmission ¹Cochrane Database of probiotic - treated patients did not show a reduction in CDI based on detection of C. difficile in the stool. Goldenberg JZ et al. (2017) Cochrane Database Syst Rev. 12: CD006095. doi : 10.1002/14651858 CDI AMR x Simple x Reliable x P oint - of - Care x Preventative SYN - 004
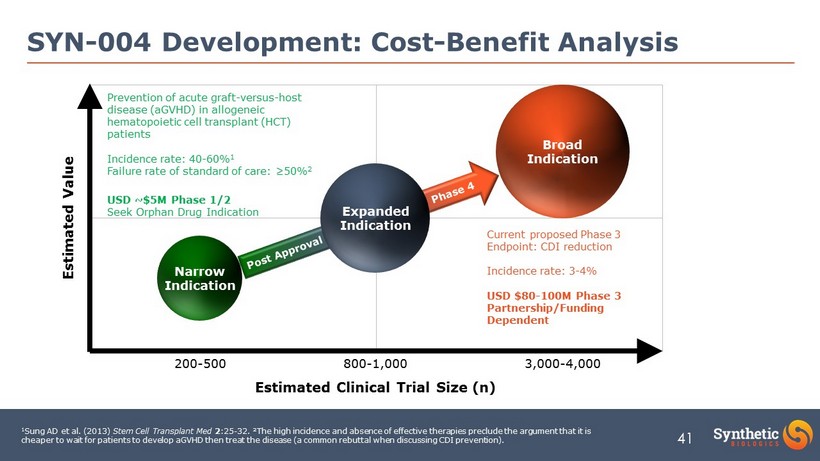
41 SYN - 004 Development: Cost - Benefit Analysis Broad Indication Estimated Clinical Trial Size (n) Estimated Value Current proposed Phase 3 Endpoint: CDI reduction Incidence rate: 3 - 4% USD $80 - 100M Phase 3 Partnership/Funding Dependent Narrow Indication 3,000 - 4,000 800 - 1,000 200 - 500 Expanded Indication Prevention of acute graft - versus - host disease (aGVHD) in allogeneic hematopoietic cell transplant (HCT) patients Incidence rate: 40 - 60% 1 Failure rate of standard of care: ≥50% 2 USD ~$5M Phase 1/2 Seek Orphan Drug Indication 1 Sung AD et al. (2013) Stem Cell Transplant Med 2 :25 - 32. ²The high incidence and absence of effective therapies preclude the argument that it is cheaper to wait for patients to develop aGVHD then treat the disease (a common rebuttal when discussing CDI prevention).
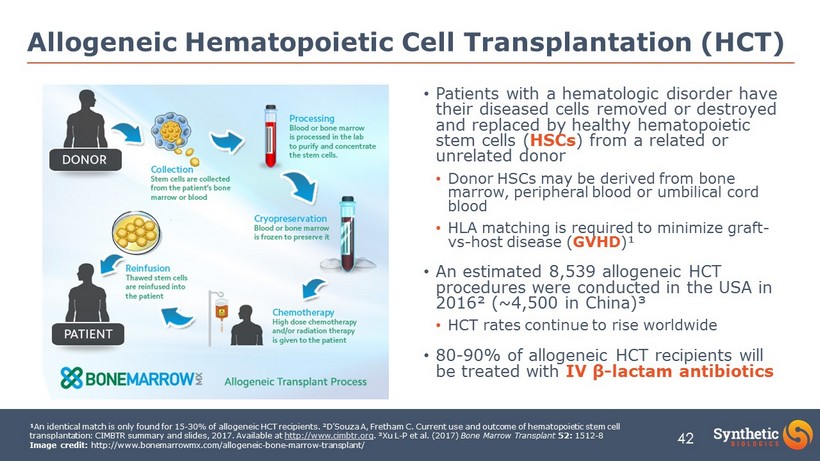
42 • Patients with a hematologic disorder have their diseased cells removed or destroyed and replaced by healthy hematopoietic stem cells ( HSCs ) from a related or unrelated donor • Donor HSCs may be derived from bone marrow, peripheral blood or umbilical cord blood • HLA matching is required to minimize graft - vs - host disease ( GVHD )¹ • An estimated 8,539 allogeneic HCT procedures were conducted in the USA in 2016² (~4,500 in China)³ • HCT rates continue to rise worldwide • 80 - 90% of allogeneic HCT recipients will be treated with IV β - lactam antibiotics Allogeneic Hematopoietic Cell Transplantation (HCT) ¹ An identical match is only found for 15 - 30% of allogeneic HCT recipients. ²D’Souza A, Fretham C. Current use and outcome of hematopoietic stem cell transplantation: CIMBTR summary and slides, 2017. Available at http://www.cimbtr.org . ³Xu L - P et al. (2017) Bone Marrow Transplant 52: 1512 - 8 Image credit: http://www.bonemarrowmx.com/allogeneic - bone - marrow - transplant/
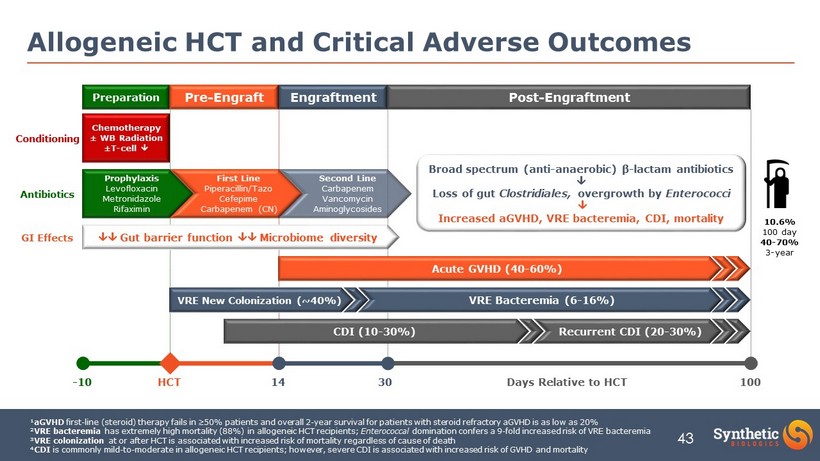
43 Allogeneic HCT and Critical Adverse Outcomes ¹ aGVHD first - line (steroid) therapy fails in ≥50% patients and overall 2 - year survival for patients with steroid refractory aGVHD is a s low as 20% ² VRE bacteremia has extremely high mortality (88%) in allogeneic HCT recipients; Enterococcal domination confers a 9 - fold increased risk of VRE bacteremia ³ VRE colonization at or after HCT is associated with increased risk of mortality regardless of cause of death ⁴ CDI is commonly mild - to - moderate in allogeneic HCT recipients; however, severe CDI is associated with increased risk of GVHD and mo rtality Preparation Engraftment - 10 HCT 14 30 Days Relative to HCT 100 Prophylaxis Levofloxacin Metronidazole Rifaximin Acute GVHD (40 - 60%) Post - Engraftment First Line Piperacillin/ Tazo Cefepime Carbapenem (CN) Second Line Carbapenem Vancomycin Aminoglycosides Chemotherapy ± WB Radiation ± T - cell CDI (10 - 30%) Recurrent CDI (20 - 30%) VRE Bacteremia (6 - 16%) Pre - Engraft 10.6% 100 day 40 - 70% 3 - year VRE New Colonization (~40%) Gut barrier function Microbiome diversity Conditioning Antibiotics GI Effects Broad spectrum (anti - anaerobic) β - lactam antibiotics Loss of gut Clostridiales, overgrowth by Enterococci Increased aGVHD, VRE bacteremia, CDI, mortality
44 • Rationale for Primary Endpoint • Decreased microbiome diversity due to IV β - lactam antibiotics is strongly associated with aGVHD ¹ ‒ aGVHD occurs in 40 - 60% of allogeneic HCT recipients • Prevention of aGVHD in allogeneic HCT recipients is critical to patient outcomes and survival² ‒ First - line aGVHD therapies (steroids) fail in ≥50% of patients resulting in very poor overall survival • Rationale for Secondary Endpoints • Reduced microbiome diversity enables VRE colonization , increases fatal VRE bacteremia ³ and CDI ⁴ • Clinical Trial Concepts • Phase 1/2 study to evaluate SYN - 004 PK, safety and microbiome protection in allogeneic HCT recipient ‒ 1 ƒ Endpoint likely serum PK SYN - 004, antibiotic in allogeneic HCT recipients ‒ 2 ƒ Endpoint changes in stool microbiome (incl. VRE colonization), aGVHD at day 100 in allogeneic HCT recipients • Phase 3 study of SYN - 004 to prevent aGVHD ‒ 1 ƒ Endpoint likely aGVHD - free survival in allogeneic HCT recipients ‒ 2 ƒ Endpoints may include reduced VRE colonization , VRE bacteremia , CDI Prevention of aGVHD in allogeneic HCT recipients SYN - 004 (ribaxamase) Indication Expansion Concept 44 ¹Shono Y et al. (2016) Sci Transl Med 8: 339ra71. ²The high incidence and absence of effective therapies preclude the argument that it is cheaper to wait for patients to develop aGVHD then treat the disease (a common rebuttal when discussing CDI prevention). ³Taur Y et al. (2012) Clin Infect Dis 55: 905 - 14. ⁴Dubberke ER et al. (2010) Clin Transplant 24: 192 - 8
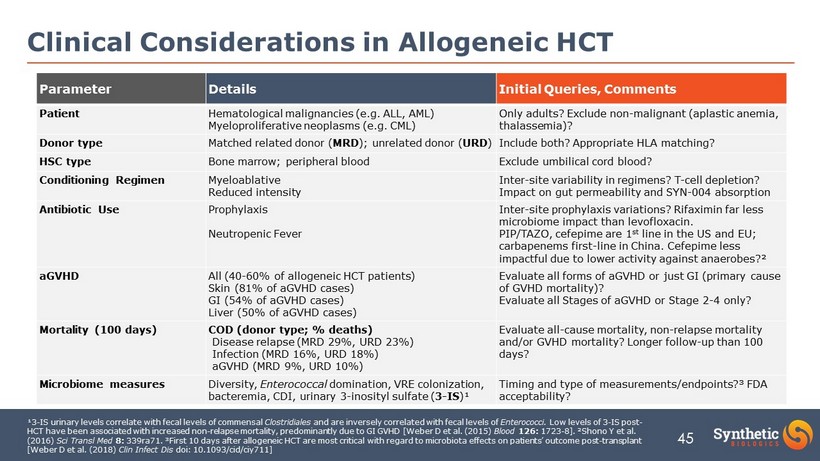
45 Clinical Considerations in Allogeneic HCT Parameter Details Initial Queries, Comments Patient Hematological malignancies (e.g. ALL, AML) Myeloproliferative neoplasms (e.g. CML) Only adults? Exclude non - malignant (aplastic anemia, thalassemia)? Donor type Matched related donor ( MRD ); unrelated donor ( URD ) Include both? Appropriate HLA matching? HSC type Bone marrow; peripheral blood Exclude umbilical cord blood? Conditioning Regimen Myeloablative Reduced intensity Inter - site variability in regimens? T - cell depletion? Impact on gut permeability and SYN - 004 absorption Antibiotic Use Prophylaxis Neutropenic Fever Inter - site prophylaxis variations? Rifaximin far less microbiome impact than levofloxacin. PIP/TAZO, cefepime are 1 st line in the US and EU; carbapenems first - line in China. Cefepime less impactful due to lower activity against anaerobes?² aGVHD All (40 - 60% of allogeneic HCT patients) Skin (81% of aGVHD cases) GI (54% of aGVHD cases) Liver (50% of aGVHD cases) Evaluate all forms of aGVHD or just GI (primary cause of GVHD mortality)? Evaluate all Stages of aGVHD or Stage 2 - 4 only? Mortality (100 days) COD (donor type; % deaths) Disease relapse (MRD 29%, URD 23%) Infection (MRD 16%, URD 18%) aGVHD (MRD 9%, URD 10%) Evaluate all - cause mortality, non - relapse mortality and/or GVHD mortality? Longer follow - up than 100 days? Microbiome measures Diversity, Enterococcal domination, VRE colonization, bacteremia, CDI, urinary 3 - inosityl sulfate ( 3 - IS )¹ Timing and type of measurements/endpoints?³ FDA acceptability? ¹3 - IS urinary levels correlate with fecal levels of commensal Clostridiales and are inversely correlated with fecal levels of Enterococci. Low levels of 3 - IS post - HCT have been associated with increased non - relapse mortality, predominantly due to GI GVHD [Weber D et al. (2015) Blood 126: 1723 - 8]. ²Shono Y et al. (2016) Sci Transl Med 8: 339ra71. ³First 10 days after allogeneic HCT are most critical with regard to microbiota effects on patients’ outcome post - trans plant [Weber D et al. (2018) Clin Infect Dis doi : 10.1093/cid/ciy711 ]