| UNVEILING NEXT GEN CAR - T CELL THERAPIES CORPORATE PRESENTATION JANUARY 2023 NASDAQ: GRCL GRACELLBIO.COM |

| 2 DISCLAIMER This presentation has been prepared by Gracell Biotechnologies Inc. (the “Company”) solely for information purpose and has no t b een independently verified. By viewing or accessing the information contained in this presentation, the recipient hereby acknowledges and agrees that no rep resentations, warranties or undertakings, express or implied, are made by the Company or any of its directors, shareholders, employees, agents, affiliate s, advisors or representatives as to, and no reliance should be placed upon, the accuracy, fairness, completeness or correctness of the information or opinions presented or contained in this presentation. None of the Company or any of its directors, shareholders, employees, agents, affiliates, advisors or representatives accept any resp ons ibility whatsoever (in negligence or otherwise) for any loss howsoever arising from any information presented or contained in this presentation or otherwise arisi ng in connection with the presentation. The information presented or contained in this presentation speaks as of the date of this presentation and is subject to chan ge without notice. Certain statements in this presentation, and other statements that the Company may make, are forward - looking statements within t he meaning of Section 27A of the Securities Act of 1933, as amended (the “Securities Act”), Section 21E of the Securities Exchange Act of 1934, as amended., o r t he Private Securities Litigation Reform Act of 1995. These statements reflect the Company’s intent, beliefs or current expectations about the future. These statements ca n b e recognized by the use of words such as “expects,” “plans,” “will,” “estimates,” “projects,” “intends,” “anticipates,” “believes,” “confident” or words of similar me ani ng. These forward - looking statements are not guarantees of future performance and are based on a number of assumptions about the Company’s operations and other factors, m any of which are beyond the Company’s control, and accordingly, actual results may differ materially from these forward - looking statements. The Company or a ny of its affiliates, advisers or representatives has no obligation and does not undertake to revise forward - looking statements to reflect future events or circum stances. This presentation shall not constitute an offer to sell or the solicitation of an offer to buy any securities in any jurisdic tio n nor shall there be any sale of securities in any state or jurisdiction in which such offer, solicitation or sale would be unlawful prior to registration or qualification unde r t he securities laws of any such state or jurisdiction. No securities of the Company may be sold in the United States without registration with the United States Securities and Exch ang e Commission (the “SEC”) or an exemption from such registration pursuant to the Securities Act and the rules and regulations thereunder. No part of this pre sen tation shall form the basis of or be relied upon in connection with any contract or commitment whatsoever. Specifically, these materials do not constitute a “prospectus” wi thin the meaning of the Securities Act. This presentation does not contain all relevant information relating to the Company or its securities, particularly with resp ect to the risks and special considerations involved with an investment in the securities of the Company and is qualified in its entirety by reference to those risks mor e f ully discussed in the section titled “Risk Factors” in the Company’s most recent annual report on Form 20 - F, as well as discussions of potential risks, uncertainties, and other important factors in the Company’s subsequent filings with the SEC. |

| Developing transformational solutions to broaden the use of breakthrough cell therapies across hematological and solid tumors . REVOLUTIONIZING CAR - T cell therapy. 3 |

| 4 At a Glance Global, Clinical - Stage Biopharma Company Clinically - validated Technology Platforms Rich, highly differentiated Clinical Pipeline Next - day manufacturing autologous CAR - T with enhanced cell fitness Off - the - shelf allogeneic CAR - T with optimized persistence 6 100+ FASTCAR - T GC012F Lead Asset 3 100% MRD - Well capitalized with cash runway for next 24 months Candidates currently in the clinic Patients dosed since 2017, leveraging investigator - initiated studies to accelerate innovation cycle Indications: r/r multiple myeloma, newly - diagnosed multiple myeloma, r/r B - NHL Achieved in all treated r/r and newly - diagnosed multiple myeloma patients |

| William Cao, Ph.D., B.M. Founder, Chairman & CEO Wendy Li, M.D. Chief Medical Officer Kevin Xie, Ph.D., M.B.A. Chief Financial Officer Samuel Zhang, Ph.D. Chief Business Officer Jenny Ni, M.D., Ph.D. Chief Technology Officer • 30+ years in biotech leadership and R&D • Co - founder and CEO of Cellular Biomedicine Group • 100+ issued patents & applications for advanced cell therapies • 20+ years of leading all critical aspects of clinical development and medical affairs • 30+ successful IND, NDA and BLA filings • CMO of EXUMA Biotech • 20+ years in healthcare investment and corporate leadership • President of Fosun Healthcare Holdings • Portfolio manager at Locust Walk Capital, Scopia Capital and Great Point Partners • 20+ years in BD, corporate strategy, and pharmaceutical commercialization • Global I - O s trategy leader at Novartis and BMS • CBO of NeoImmuneTech • 25+ years in gene & cell therapy, vaccine and contract manufacturing • Led CMC development of five IND filings / approvals for hematological and solid malignancies 5 Leadership Team Experienced in R&D and Clinical Development |

| 6 1. Phase 3 may not be required if Phase 2 is registrational 2. IIT (investigator - initiated trial) is optional not mandatory, and it serves as early evidence for safety and potentially efficac y for the individual programs. IND studies will build on IIT results. We intend to use the clinical data generated from China IITs in our IND filings to the FDA and the NMPA; however, we make no guarantee that such data will be ac cep ted by the FDA and/or the NMPA. R/R MM, relapsed or refractory multiple myeloma; Newly Diagnosed MM, newly - diagnosed multiple myeloma; B - NHL, B cell non - Hodgkin ’s lymphoma; B - ALL, B cell acute lymphoblastic leukemia; AML, acute myeloid leukemia; T - ALL, T cell acute lymphoblastic leukemia CAR - T Pipeline Targeting Hematological and Solid Tumor Indications PROGRAM INDICATION PHASE OF DEVELOPMENT Preclinical Phase 1 Phase 2/3 1 GC012F BCMA/CD19 R/R MM Newly Diagnosed MM B - NHL GC019F CD19 Adult B - ALL GC017F AML GC502 CD19/CD7 B - ALL GC027 CD7 Adult T - ALL GC508 MM Donor - derived CAR GC007g CD19 B - ALL SMART CAR - T GC503 Mesothelin Solid tumors GC506 Claudin 18.2 Solid tumors China IIT 2 China IND |

| GC012F BCMA/CD19 Dual - Targeting for Multiple Myeloma & B - NHL Autologous CAR - T Platform |

| 8 FasTCAR Platform Next - Day Manufacturing to Reach Patients Faster 22 to 36 HOURS 1 to 6 WEEKS Conventional CAR - T Manufacturing FASTER Availability to patients ENHANCED T - cell fitness SIGNIFICANT Cost savings ADVANTAGES |

| FasTCAR Cuts Manufacturing Time to 22 - 36 Hours: Combines Activation & Transduction Steps, and Eliminates Need for ex vivo Expansion 9 FasTCAR Platform Activation Transduction ex vivo Expansion 5 days to 5 weeks 1 to 2 days 1 to 3 days Conventional Manufacturing 1 to 6 WEEKS Concurrent Activation - Transduction 22 - 36 HOURS Releasing Tests Apheresis Purification Filling Freezing Release & Infusion Isolation Apheresis Isolation Releasing Tests Purification Filling Freezing Release & Infusion 1 Gracell transforms the three primary production steps — activation, transduction and expansion — into a single “concurrent activatio n - transduction” step. With minimized ex vivo culture time, FasTCAR - T cells are younger and shows enhanced proliferation and tumor clearance activities in preclinical studies , making possible the lower cell dosage and eliminating the need for ex vivo expansion. Expansion happens in patient body, an optimal condition. 2 1 2 |

| CD4 CD8 FasTCAR GC012F Conventional CAR - T With enhanced stemness and proliferation, FasTCAR - T cells may lead to lower dosage requirements and improved therapeutic results 10 Memory T cells, such as Tscm cells and Tcm cells, are indicators of T - cell youth and associated with CAR - T cell therapeutic effe cts. FasTCAR Platform Enhanced T - Cell Fitness Tscm – stem cell - like memory T cells T cm – central memory T cells Tem – effector memory T cells Teff – effector T cells T scm 48.7% T scm 88.5% T scm 38.1% T scm 16.5% FasTCAR preserves high percentage of young Tscm cells 1 |

| 11 1. Boucher K, Parquet N, Widen R, et al. Clin Cancer Res. 2012;18(22):6155 - 6168. 2. Hua Jiang, et al. ASH Annual Meeting 2020, 178. GC012F for Multiple Myeloma MOA Dual - Targeting to Reduce Relapse Risk BCMA/CD19 Dual CAR - T demonstrated effective elimination of MM progenitor cells 2 NT CD19 CAR - T BCMA CAR - T BCMA - CD19 Dual CAR - T Relative Colony Formation 200 150 100 50 0 **0.0053 ***0.0009 *0.0381 0.0944 0.0141 Targeting TWO antigens to address the risk of BCMA antigen loss and drive deep and durable response in the treatment of multiple myeloma (MM) BCMA A proven target for MM CD19 Expressed on MM cells and progenitor cells 1 BCMA - CD19 Dual CAR - T anti - CD19 scFv anti - BCMA scFv CD19 BCMA MM Progenitor MM cell CD19 (Low expression) |

| Consistently Favorable Safety Profile Mostly low - grade CRS in r/r MM No CRS in 75% newly - diagnosed MM patients treated No neurotoxicity or ICANS 12 GC012F for Multiple Myeloma Differentiation Clear Differentiation Across Three Key Attributes Game - changing Next - day Manufacturing Approx. 22 - 36 hours Highly Competitive Efficacy 100% MRD - in all treated r/r MM and newly - diagnosed MM patients BCMA/CD19 Dual - targeting Compelling clinical data in both r/r MM and newly - diagnosed MM |

| 13 GC012F for r/r Multiple Myeloma S tudy Design / Patient Baseline IIT Enrollment and Dosing Completed IIT · First patient in 10/2019 · Enrollment completion 01/2022 · Data presented at ASCO & EHA 2022 IIT, investigator initiated trial; F, fludarabine; C, cyclophosphamide; HSCT, hematopoietic stem cell transplantation a. By mSMART 3.0 b. By presence two of del(17p), t(4;14), t(14;16), t(14;20), gain 1q, or p53 mutation c. PI, IMiD and any other including anti - CD38 antibody; d. ≥ 1 PI (Ixazomib and Bortezomib were approved in China), ≥ 1 IMiDs (only Lenalidomide is approved for MM in China) and ≥ 3 other anti - myeloma drugs of any other class; 90% patients treated classified as high - risk according to mSMART 3.0 guidelines Patient Baseline Characteristics Total N=29 Median age, years (range) 57 (27 - 76) Male, n(%) 17 (59) Type of myeloma, n(%) IgG 13 (45) IgA 6 (21) IgD 5 (18) Light chain 5 (18) Median years since d iagnosis, years (range) 4 (1 - 10) High - risk profile a , n(%) 26 (90) Double - hit b , n(%) 3 (10) Extramedullary plasmacytomas ≥ 1, n(%) 8 (28) Patient Baseline Characteristics Total N=29 Median prior regimens of therapy, n (range) 5 (2 - 11) Median prior lines of therapy, n (range) 5 (2 - 9) Prior auto - HSCT, n (%) 11 (38) Triple - exposed c , n(%) 28 (97) PI refractory 27 (93) IMiD refractory 27 (93) anti - CD38 refractory 10 (34) Penta - exposed d , n(%) 18 (62) Primary refractory, n (%) 3 (10) Refractory to last therapy, n (%) 24 (83) DOSE LEVEL 1 1x10 5 cells/kg DOSE LEVEL 2 2x10 5 cells/kg DOSE LEVEL 3 3x10 5 cells/kg Consent and Screening Apheresis GCO12F Next Day Manufacturing QC Release Lymphodepletion (F:30mg/m 2 /day C:300mg/m 2 /day)*3days GC012F Single infusion Follow - up assessment visits D - 5 to - 3 D0 |

| 6.9% 10.3% 75.9% 14 ORR, overall response rate; sCR, stringent complete response; CR, complete response, VGPR, very good partial response; MRD, m ini mal residual disease *Sensitivity of MRD - : At 10 - 4 in 9 patients tested by Flow cytometry; At 10 - 6 in 20 patients tested by EuroFlow. Choice of MRD test is due to the availability at the study centers. GC012F for r/r Multiple Myeloma E fficacy Fast, Deep & Durable Responses Data cut - off 06/08/2022 · 90% of study population being high risk All patients PR VGPR CR/sCR n = 29 Time to earliest response as first assessment timepoint Median duration of response (DOR) at data cut - off with 90% of study population being high risk (95%, CI: 7.6 - 33.1) Median duration to follow - up Range 4.9 to 34.5 mos. 93.1 % ORR 27/29 patients 100 % 75.9 % MRD - sCR 22/29 patients best response achieved to date MRD - 29/29 patients * 28 DAYS 15.7 MOS. 11.0 MOS. |

| 15 1, Sensitivity of MRD - : At 10 - 4 in 9 patients tested by Flow cytometry; At 10 - 6 in 20 patients tested by EuroFlow. Choice of MRD test is due to the availability at the study centers. 2, Munshi NC, Blood Adv. 2020 Dec 8;4(23):5988 - 5999 GC012F for r/r Multiple Myeloma MRD Negativity 100% MRD - in All Treated Patients Data cut - off 06/08/2022 · 90% of study population being high risk MRD assessment – EuroFlow 10 - 6 0% 20% 40% 60% 80% 100% n = 1 n = 17 MRD+ MRD - 100% of treated patients achieved MRD negativity 1 • 100% of evaluable patients assessed by EuroFlow were MRD negative at Month 6 (n=13; sensitivity 10 - 6 ) • 87.5% of evaluable patients assessed by EuroFlow were MRD negative at Month 12 • Some patients with shorter duration of follow - up could not get re - assessed by time of data cut - off, due to the Covid - 19 pandemic 94.4% 100% 87.5% MRD in evaluable patients by EuroFlow, at month 1 (n=18), month 6 (n=13) and month 12 (n=8) Month 1 n = 18 Month 6 n = 13 Month 12 n = 8 12.5% 5.6% n = 1 n = 7 Patients(%) MRD negativity could be associated with significantly improved survival outcomes 2 |

| 16 1 CRS criteria, ASBMT consensus grading CRS - Cytokine release syndrome, ICANS - Immune effector cell - associated neurotoxicity syndrome GC012F for r/r Multiple Myeloma Safety Consistently Favorable Safety Profile N=29 CRS 1 (n,%) ICANS (n,%) Grade 0 4 (14) 0 (0) Grade 1 14 (48) 0 (0) Grade 2 9 (31) 0 (0) Grade 3 # 2 (7) 0 (0) Grade 4 - 5 0 (0) 0 (0) CRS any grade Median (days) Min, Max (days) Time to onset 6 2,10 Duration 3 1,8 # CRS treated with Tocilizumab, vasopressors and dexamethasone Mostly Low - grade CRS · No Neurotoxicity or ICANS |

| 17 GC012F for Newly Diagnosed Multiple Myeloma S tudy Design / Patient Baseline First Clinical Data Presented at ASH 2022 IIT 1 · First patient in 8/2021 · Patients continue to be assessed for response · Data cut - off 10/14/2022 DOSE LEVEL 1 1x10 5 cells/kg DOSE LEVEL 2 2x10 5 cells/kg DOSE LEVEL 3 3x10 5 cells/kg Consent and Screening GCO12F Next Day Manufacturing QC Release Lymphodepletion GC012F Single infusion Post - infusion treatment based on PI’s evaluation D - 5 to - 3 D0 1. IIT – Investigator Initiated Study. 2. 2 cycles of induction therapy RVd ( lenalidomide, bortezomib, and dexamethasone; PAD cycle in one case) are given before or after apheresis. 3. High - risk is defined as meeting at least one of the following: a) R - ISS stage II or III; b) High - risk cytogenetics: del17p, t(4; 14), t(14;16), or 1q21 ≥4 copies; c) Extramedullary disease; d) IgD or IgE subtype; e) High - risk definition according to mSMART3.0; f) LDH > the upper limit of normal. 4. Except one cycle of PAD (bortezomib, doxorubicin, and dexamethasone). 5. 15 pts evaluable for cytogenetics high risk. Follow - up assessment visits Apheresis RVd induction therapy 2 cycles 2 Patient Baseline Characteristics Total N=16 (%) Median age, years (range) 59 (43 - 69) Male, n (%) 11 (69) Type of myeloma, n (%) IgG 7 (44) IgA 4 (25) IgD 2 (13) Light chain 3 (19) Induction therapy, n (%) 2 cycles RVd 4 15 (94) High - risk, n (%) 16 (100) R - ISS stage ll / lll 15 (94) High - risk cytogenetics 5 7 (47) Extramedullary plasmacytoma ≥1 11 (69) High - risk as mSMART3.0 15 (94) LDH > upper limit of normal 3 (19) ECOG performance status, n (%) 0 3 (19) 1 9 (56) 2 4 (25) Key Eligibility Criteria High - risk 3 , transplant eligible, newly - diagnosed Multiple Myeloma (NDMM) |

| 18 GC012F for Newly Diagnosed Multiple Myeloma S afety Excellent Initial Safety Profile CRS - Cytokine release syndrome, ICANS - Immune effector cell - associated neurotoxicity syndrome 1 CRS graded by ASTCT Consensus criteria; treated with tocilizumab and/or glucocorticoids. 2 ICANS graded by ASTCT Consensus. N=16 CRS (n,%) ICANS (n,%) Grade 0 12 (75) 0 (0) Grade 1 3 (19) 0 (0) Grade 2 1 (6) 0 (0) Grade 3 0 (0) 0 (0) Grade 4 - 5 0 (0) 0 (0) CRS any grade Median (days) Min, Max (days) Time to onset 6 6,7 Duration 2 1,4 No CRS 1 experienced by 75% patients · No Neurotoxicity or ICANS 2 |

| 19 ORR, overall response rate; sCR, stringent complete response; CR, complete response, VGPR, very good partial response; MRD, m ini mal residual disease 1. MRD was tested by Euroflow at a sensitivity of 10 - 6 2. Richardson PG, et al. N Engl J Med 2022;387(2):132 – 47. Data is of the RVd plus autologous stem cell transplant (auto HSCT) group, which includes 3 cycles of RVd (lenalidomide, bortezomib, and dexamethasone) followed by high dose melphalan, auto HSCT, 2 cycles of RVd , and then Lenalidomide maintenance. MRD is measured at the start of the maintenance therapy with sensitivity of 10 - 5 GC012F for Newly Diagnosed Multiple Myeloma ORR 100% ORR Across Dose Levels Data cut - off 10/14/2022 12.5% 20% 87.5% 100% 100 % 80% 0 20 40 60 80 100 All patients (N=16) DL1 (n=1) DL2 (n=5) DL3 (n=10) Patients(%) ORR 100% ORR 100% ORR 100% ORR 100% VGPR CR/sCR 100 % all ≥ VGPR ORR 16/16 patients ▪ Median duration of response (DOR) was not reached at data cut off ▪ Median duration of follow up: 8.0 months (range: 1.3 - 15.4 months) Preliminary efficacy demonstrates tremendous potential for substantial improvement over currently available therapies for NDMM, one of which shows sCR % of 32.9% and MRD negativity rate of 54.4% 2 100 % MRD - 1 16/16 patients 87.5 % MRD - sCR 14/16 patients best response achieved to date |

| 20 GC012F for Newly Diagnosed Multiple Myeloma MRD Negativity 100% MRD - in All Treated Patients Data cut - off 10/14/2022 MRD assessment – EuroFlow 10 - 6 MRD+ MRD - MRD in evaluable patients by EuroFlow, at month 1 (n=13), month 6 (n=8) and month 12 (n=3) Patients(%) 100 % 100% 100 % 0 20 40 60 80 100 Month 1 Month 6 Month 12 n = 13 n = 8 n = 3 • 100% of MRD evaluable patients achieved MRD negativity at Month 1, Month 6 and Month 12 • 100% of MRD evaluable patients achieved MRD negativity in all dose levels * MRD was tested by Euroflow at a sensitivity of 10 - 6 |

| 21 GC012F for Newly Diagnosed Multiple Myeloma Response Plot Fast, Deep & Durable Responses Data cut - off 10/14/2022 DL3 Pt 01 Pt 02 Pt 04 Pt 05 Pt 06 Pt 07 Pt 08 Pt 09 Pt 16 Pt 17 DL2 Pt 03 Pt 14 Pt 12 Pt 13 Pt 11 DL1 Pt 10 0 M1 M2 M3 M4 M5 M6 M7 M8 M9 M10 M11 M12 M13 M14 M15 M16 Months after CAR - T infusion Baseline No. of HR factor 1 1. HR factors include: a) R - ISS stage II or III; b) High - risk cytogenetics: del17p, t(4;14), t(14;16), or 1q21 ≥4 copies; c) Extram edullary disease; d) IgD or IgE subtype; e) High - risk definition according to mSMART3.0; f) LDH > the upper limit of normal. Median time of follow - up: 8.0 months (range: 1.3 – 15.4 months) CRS (<Grade 3) CRS (≥Grade 3) ICANS (<Grade 3) ICANS (≥Grade 3) Before Evaluation ● MRD+ ● MRD – PR VGPR CR sCR In Follow - up PD 4 3 3 4 2 3 3 2 3 3 4 2 4 4 5 4 |

| 22 1. American journal of hematology. 2021; 96(10):1295 - 1312. 2. Lancet Oncol. 2019;20(1):31 - 42. 3. Blood Cancer Journal. 2020; 10:73. 4. Blood. 2017;130:2755. 5. Hum Gene Ther. 2018; 29(5): 585. GC012F for B - NHL MOA Novel Dual - Targeting Approach for B - NHL Targeting both CD19 and BCMA could potentially improve CAR - T efficacy and reduce relapse due to antigen escape CD19 CAR - T is proven to be effective for the treatment of NHL, although its efficacy is yet to be improved 1,2 BCMA is expressed in 39% to 97% clinical samples of NHL 3 - 5 , making it a valid therapeutic target B - NHL Cell CD19 - BCMA Dual CAR - T anti - BCMA scFv anti - CD19 scFv BCMA CD19 |

| 23 GC012F for B - NHL Study Design / Patient Baseline First - in - Human Data Presented at EHA 2022 IIT · Data presented at EHA 2022 DOSE LEVEL 1 2 - 3x10 5 cells/kg DOSE LEVEL 2 4 - 6x10 5 cells/kg DOSE LEVEL 3 8 - 12x10 5 cells/kg Consent and Screening Apheresis GCO12F Next Day Manufacturing QC Release Lymphodepletion (F:30mg/m 2 /day C:300mg/m 2 /day)*3days GC012F Single infusion Follow - up assessment visits D - 5 to - 3 D0 Patient Baseline Characteristics Total (n=3) Median age, years (range) 52 (31 - 60) Lymphoma subtype DLBCL, n (%) 3 (100) Disease stage, n (%) 1 IV 3 (100) ECOG 1, n (%) 3 (100) Anti - CD20 3 (100) Immuno - phenotype, n (%) CD19 3 (100) BCMA 2 (67) Median prior lines of therapy, n (range) 2 (2 - 3) IPI score ≥ 3, n (%) 2 (67) Relapse/refractory subgroup, n (%) Relapse 2 (67) Refractory 1 (33) Prior auto - HSCT, n (%) 0 (0) Heavily pre - treated patients with bulky disease enrolled IIT, investigator initiated trial; F, fludarabine; C, cyclophosphamide, DLBCL, diffuse large B cell lymphoma, HSCT, hematopoietic stem cell transplantation |

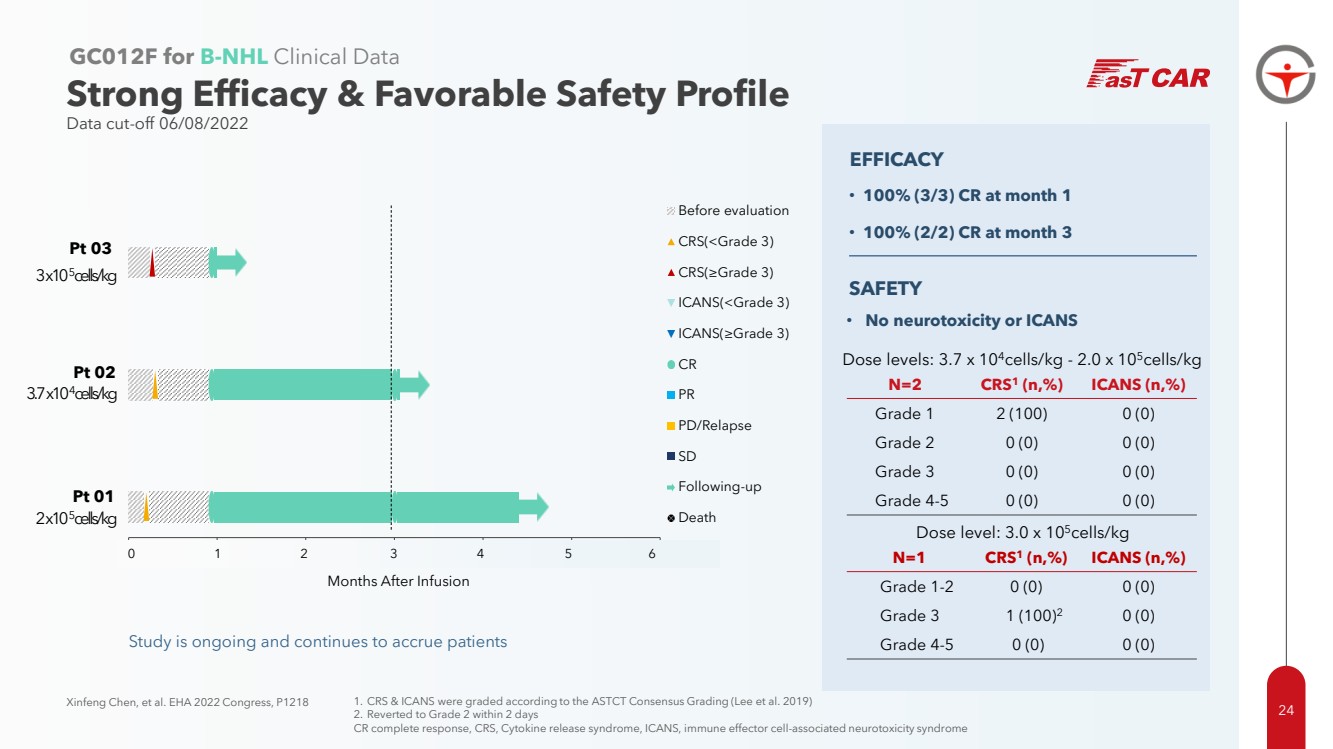
| 0 30 60 90 120 150 180 Months After Infusion Before evaluation CRS(<Grade 3) CRS(≥Grade 3) ICANS(<Grade 3) ICANS(≥Grade 3) CR PR PD/Relapse SD Following-up Death 0 1 2 3 4 5 6 Pt 03 Pt 01 2 x10 5 cells/kg Study is ongoing and continues to accrue patients N=2 CRS 1 (n,%) ICANS (n,%) Grade 1 2 (100) 0 (0) Grade 2 0 (0) 0 (0) Grade 3 0 (0) 0 (0) Grade 4 - 5 0 (0) 0 (0) 24 Xinfeng Chen, et al. EHA 2022 Congress, P1218 GC012F for B - NHL Clinical Data Strong Efficacy & Favorable Safety Profile Data cut - off 06/08/2022 Dose levels: 3.7 x 10 4 cells/kg - 2.0 x 10 5 cells/kg Dose level: 3.0 x 10 5 cells/kg N=1 CRS 1 (n,%) ICANS (n,%) Grade 1 - 2 0 (0) 0 (0) Grade 3 1 (100) 2 0 (0) Grade 4 - 5 0 (0) 0 (0) Pt 02 3 x10 5 cells/kg 3.7 x10 4 cells/kg 1. CRS & ICANS were graded according to the ASTCT Consensus Grading (Lee et al. 2019) 2. Reverted to Grade 2 within 2 days CR complete response, CRS, Cytokine release syndrome, ICANS, immune effector cell - associated neurotoxicity syndrome SAFETY • No neurotoxicity or ICANS • 100% (3/3) CR at month 1 • 100% (2/2) CR at month 3 EFFICACY |
| Allogeneic CAR - T Platform GC502 for B - ALL CD19/CD7 GC027 for T - ALL CD7 |

| 26 Off - the - Shelf TruUCAR Platform MOA Novel Dual - Directed CAR Design to Enhance Persistence Host vs. graft rejection (HvG) hinders the persistence of allogeneic CAR - T cells in patient body Preventing HvG while controlling infection risk poses the key challenge in developing effective and safe off - the - shelf CAR - T therapy Gracell’s Elegant Solution • Reduces risk of rejection and extends persistence of CAR - T cells • Eliminates the need for being co - administered with additional strong immunosuppressant after conventional lymphodepletion CAR2 Tumor antigen CAR targets malignant cells and enables wide applicability for different cancers CD7 CAR Targets a patient’s T and NK cells to suppress rejection of allogeneic CAR - T cells Patient’s T cell or NK cell T - Ag KO Prevent fratricide Avoid GvHD Patient’s normal tissues Cancer cell TCR KO Enhancer Tumor lysis Prevent HvG Industry Challenge |

| 27 * Includes either autologous or donor derived CD19 or CD19 - CD22 targeted CAR - T therapy GC502 for B - ALL Study Design / Patient Baseline First TruUCAR Candidate with Dual - Directed CAR IIT · Data presented at AACR 2022 and EHA 2022 Patient Baseline Characteristics Total (N=4) Median age, years (range) 28 (15 - 34) Median prior lines of therapy (range) 5 (4 - 7) Extramedullary lesions, n (%) 1 (25%) Prior - CAR - T therapy, n (%) * 4 (100%) Prior allo - HSCT, n (%) 1 (25%) CD19/CD7 dual - directed GC502 comprehensively exemplifies the TruUCAR design, which aims for optimized persistence and wide applicability without the need of being co - administered with additional immunosuppressant DOSE LEVEL 1 1.0x10 7 cells/kg DOSE LEVEL 2 1.5x10 7 cells/kg DOSE LEVEL 3 2.0x10 7 cells/kg Consent and Screening Lymphodepletion GC502 Single infusion Follow - up assessment visits D0 |

| 28 Shiqi Li, et al. EHA 2022 Congress, P370 * Patient 01 was assessed MRD - in bone marrow but was assessed PR due to extramedullary disease. This patient received allo - HSCT at day 39 and achieved MRD - CR, however died of infection post transplant on day 95. MRD minimal residual disease, CR complete response, CRi, complete response with incomplete hematologic recovery, PR partial response, allo - HSCT allogeneic hematopoietic stem cell transplant GC502 for B - ALL Clinical Data Promising Response Reported at EHA 2022 Data cut - off 02/22/2022 1X10 6 1X10 5 1X10 4 1X10 3 1X10 2 1X10 1 1X10 0 1X10 - 1 CAR Copies Days post Car - T cell infusion Copies/µg DNA GC502 expansions measured by qPCR were peaked around day 7 - 9 ROBUST EXPANSION SAFETY • Formulation A: 2 out of 2 Grade 3 CRS • Formulation B: 2 out of 2 Grade 2 CRS • No Grade 4 or 5 CRS, no ICANS, no GvHD 0 28 56 84 112 140 Pt 04 Pt 03 Pt 02 Pt 01 Days after infusion Formulation B Formulation A DL1: 1.0x10 7 cells/kg DL2: 1.5x10 7 cells/kg Pt 01 Pt 02 Pt 03 Pt 04 * • 75% patients achieved MRD - CR/CRi EFFICACY ▲ CRS (<Gr 3 ) ▲ CRS ( ≥ Gr 3 ) ▼ ICANS (<Gr 3 ) ▼ ICANS ( ≥ Gr 3 ) Before Evaluation ● MRD+ ● MRD - ◼︎ PR ◼︎ CR/ CRi Allo - HSCT In Follow - up Death |

| Months after infusion 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 29 Lei Gao , et al. AACR Annual Meeting 2021, LB147 1. D.I. Marks, C. Rowntree, Management of adults with T - cell lymphoblastic leukemia, Blood 2017 SOC, standard of care; mOS, median overall survival; MRD, minimal residual disease, CR complete response, CRi, complete respo nse with incomplete hematologic recovery, PD, progressive disease GC027 for T - ALL CD7 Dual - Functioned Allogeneic CAR - T Deep And Durable Responses in T - ALL IIT · Data presented at AACR 2020 / EHA 2020 / AACR 2021 · Data cut - off 02/2021 • 100% CR/CRi (6/6) • 83% MRD - CR/CRi (5/6) • Median PFS: 7.75 months • The longest DOR at cut - off (MRD - CR): 16.8 months EFFICACY • All 6 patients tolerated infusion of GC027 • No ICANS, no GvHD • 6/6 patients experienced CRS, no Grade 5 CRS • AEs were reversible SAFETY Relapsed T - ALL remains a high unmet medical need as SOC only results in 30% - 40% response rate with mOS of six months among responders 1 Response, Duration of Remission and Adverse Events of GC027 DL 3 KT001 DL 2 KT004 XT004 KT005 DL 1 KT002 KT008 Before Evaluation ● MRD+ ● MRD - ◼︎ CR/ CRi Allo - HSCT In Follow - up ◼︎ PD/Relapse |

| Allogeneic CAR - T from HLA - Matched Donor GC 007 g for B - ALL CD 19 DONOR - DERIVED CAR |

| 31 Allo - HSCT, allogeneic human stem cell transplant GC 007 g for B - ALL Registrational Phase 2 Trial in R/R B - ALL Underway Clinical IIT Update as of June 2019 (n = 13 ) DL1 ( n=3 ) DL2 ( n=9 ) DL3 ( n=1 ) Overall ( n=13 ) ORR (D28) 3 (100%) 7 (77.8%) 1 (100%) 11 (84.6%) MRD - (D28) 3 (100%) 6 (66.7%) 1 (100%) 10 (76.9%) DL1 ( n=3 ) DL2 ( n=9 ) DL3 ( n=2 ) Overall ( n=14 ) CRS 1 (33.3%) 9 (100%) 2 (100%) 12 (85.7%) ≥ 3 CRS 0 1 (11.1%) 0 1 (7.1%) NT 0 0 0 0 ≥ 3 NT 0 0 0 0 aGvHD 0 2 (22.2% ) 0 2 (14.3% ) CD3 ζ CD28 Beacon • Allogeneic donor - derived, CD 19 - directed CAR - T cell therapy • Indication: R/R B - ALL patients who progress or failed allo - HSCT • T cells from HLA - matched healthy donor • No need for leukapheresis of patient • Alternative for patients ineligible for other treatment options including autologous CAR - T therapy Registrational Phase 2 trial ongoing in China |

| Second Generation Enhanced CAR - T for Solid Tumors SMART CAR - T |

| 33 SMART CAR - T for Solid Tumors Novel Mechanism to Conquer TME SMART CAR - T in Preclinical Study ✓ More robust cell proliferation and persistence ✓ Improved resistance to TME ✓ Reduced T cell exhaustion and sustained killing capacity after repeated antigen re - challenges ✓ Persistent anti - tumor activity upon tumor re - challenge Targeting TME could unlock the vast potential of immunotherapies in treating solid tumors Immunosuppressive tumor microenvironment (TME) impacts T - cell activation and survival Solid tumor cell scFv SMART CAR - T Converted into positive signaling Proliferation Persistence Resistance to TME SMART CAR - T Industry Challenge Negative signaling of suppressive TME molecule S uppressive M olecule A ctivated & R ejuvenated T cells |

| 34 Locations State - of - the - Art R&D and GMP Facilities Suzhou Global Headquarters Suzhou GMP Manufacturing Facility Shanghai Headquarters Shanghai R&D Center San Diego Innovation Center • 66,000 sq. ft. standalone facility • Plasmid, vectors and cell production • Vein - to - vein, fully - closed manufacturing capability • Received Medical Products Manufacturing Certificate in 2021 |

| Cash 35 Financial Highlights Strong Financial Position Supporting R&D and Corporate Strategy R&D and Corporate focus • Clinical development to advance key programs • Establishment of U.S. R&D center $ 229.1 million in cash, cash equivalents & short - term investments as of 9/30/22 Cash runway for next 24 months |

| 36 Corporate Milestones Anticipated Milestones Q4 2022 Accomplishments ✓ IND filings submitted in the US and China for FasTCAR - T GC012F in r/r MM ✓ FasTCAR - T GC012F in newly diagnosed MM first clinical data presented at ASH 2022 ✓ Donor - derived CAR - T GC007g in B - ALL entered registrational Phase 2 trial in China Upcoming Milestones • Provide clinical development update upon receipt of IND acceptance from FDA for FasTCAR - T GC012F in r/r MM • Initiate IND trial in US for FasTCAR - T GC012F in r/r MM • Initiate IND trial in China for FasTCAR - T GC012F in r/r MM • Longer - term follow - up data of FasTCAR - T GC012F in r/r MM from the IIT study • Initiate China IIT of SMART CAR - T GC506 targeting Claudin 18.2 - positive solid tumors • Initiate China IIT of FasTCAR - T GC017F in AML • Clinical data updates on other current and new programs at major medical conferences and/or in lead journals |

| THANK YOU INVESTOR CONTACT Gracie Tong Sr. Director of Investor Relations Gracie.Tong @gracellbio.com |
