UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM
(Mark One)
For the fiscal year ended
or
For the transition period from _____________ to _____________
Commission file number:
CLENE INC.
(Exact name of registrant as specified in its charter)
| |
| |
| (State or other jurisdiction of |
| (I.R.S. Employer |
| |
| |
| (Address of principal executive offices) |
| (Zip Code) |
(
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class |
| Trading Symbol(s) |
| Name of each exchange on which registered |
| |
| |
| The |
| |
| |
| The |
Securities registered pursuant to Section 12(g) of the Act: None.
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes ☐
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days.
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files).
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer | ☐ | Accelerated filer | ☐ |
| | ☒ | Smaller reporting company | |
|
|
| Emerging growth company | |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report.
If securities are registered pursuant to Section 12(b) of the Act, indicate by check mark whether the financial statements of the registrant included in the filing reflect the correction of an error to previously issued financial statements.
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant’s executive officers during the relevant recovery period pursuant to §240.10D-1(b). ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes
The aggregate market value of the registrant’s common stock held by non-affiliates as of June 30, 2023, the last business day of the registrant’s most recently completed second fiscal quarter, was approximately $
The number of shares outstanding of the Registrant’s shares of common stock as of March 8, 2024 was
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive proxy statement relating to its 2024 Annual Meeting of Stockholders are incorporated by reference into Part III of this Annual Report on Form 10-K where indicated. The definitive proxy statement will be filed with the U.S. Securities and Exchange Commission within 120 days after the end of fiscal year to which this report relates.
Annual Report on Form 10-K for the Year Ended December 31, 2023
Throughout this Annual Report on Form 10-K (the “Annual Report”), the “Company,” and references to “we,” “us,” or similar such references should be understood to be references to Clene Inc. and its consolidated subsidiaries.
CAUTIONARY NOTE REGARDING FORWARD LOOKING STATEMENTS
Certain statements in this Annual Report may constitute “forward-looking statements” for purposes of the federal securities laws. Our forward-looking statements include, but are not limited to, statements regarding our or our management team’s expectations, hopes, beliefs, intentions or strategies regarding our future operations. In addition, any statements that refer to projections, forecasts or other characterizations of future events or circumstances, including any underlying assumptions, are forward-looking statements. The words “anticipate,” “believe,” “contemplate,” “continue,” “could,” “estimate,” “expect,” “intends,” “may,” “might,” “plan,” “possible,” “potential,” “predict,” “project,” “should,” “will,” “would” and similar expressions may identify forward-looking statements, but the absence of these words does not mean that a statement is not forward-looking. Forward-looking statements in this Annual Report may include, for example, statements about:
| ● |
our future financial performance, including our ability to continue as a going concern; |
| ● |
our plans and strategies to raise additional funding; |
| ● |
the clinical results of our drug candidates; |
| ● |
the likelihood of commercial success for our drug candidates; |
| ● |
our plans and strategies to obtain and maintain regulatory approvals of our drug candidates; |
| ● |
the size and growth potential of the markets for our drug candidates, and our ability to serve those markets, either alone or in combination with others; |
| ● |
changes in the market for our drug candidates; |
| ● |
expansion plans and opportunities; and |
| ● |
other factors detailed under the section entitled “Risk Factors.” |
These forward-looking statements represent our views as of the date of this Annual Report and involve a number of judgments, risks and uncertainties. We anticipate that subsequent events and developments will cause our views to change. We undertake no obligation to update forward-looking statements to reflect events or circumstances after the date they were made, whether as a result of new information, future events or otherwise, except as may be required under applicable securities laws. Accordingly, forward-looking statements should not be relied upon as representing our views as of any subsequent date.
As a result of a number of known and unknown risks and uncertainties, our actual results or performance may be materially different from those expressed or implied by these forward-looking statements. Some factors that could cause actual results to differ include:
| ● |
our substantial dependence on the successful commercialization of our drug candidates, if approved, in the future; |
| ● |
our inability to maintain the listing of our common stock, $0.0001 par value (“Common Stock”) on the Nasdaq Capital Market (“Nasdaq”); |
| ● |
our significant net losses and net operating cash outflows; |
| ● |
our ability to demonstrate the efficacy and safety of our drug candidates; |
| ● |
the clinical results for our drug candidates, which may not support further development or marketing approval; |
| ● |
actions of regulatory agencies, which may affect the initiation, timing, and progress of clinical trials and marketing approval; |
| ● |
our ability to achieve commercial success for our drug candidates, if approved; |
| ● |
our ability to obtain and maintain protection of intellectual property for our technology and drug candidates; |
| ● |
our reliance on third parties to conduct drug development, manufacturing, and other services; |
| ● |
our limited operating history and our ability to obtain additional funding for operations and to complete the licensing or development, and commercialization of our drug candidates; |
| ● |
the impact of epidemics, pandemics, and the ongoing conflicts between Ukraine and Russia and Israel and Palestine on our clinical development, commercial, and other operations; |
| ● |
changes in applicable laws or regulations; |
| ● |
the effects of inflation; |
| ● |
the effects of staffing and materials shortages; |
| ● |
the possibility that we may be adversely affected by other economic, business, and/or competitive factors; and |
| ● |
other risks and uncertainties set forth in the section entitled “Risk Factors.” |
In addition, statements that “we believe” and similar statements reflect our beliefs and opinions on the relevant subject. These statements are based upon information available to us as of the date of this Annual Report, and while we believe such information forms a reasonable basis for such statements, such information may be limited or incomplete, and our statements should not be read to indicate that we have conducted an exhaustive inquiry into, or review of, all potentially available relevant information. These statements are inherently uncertain and you are cautioned not to rely unduly upon these statements.
SUMMARY OF MATERIAL RISKS ASSOCIATED WITH OUR BUSINESS
Our business is subject to numerous material and other risks that you should be aware of before making an investment decision. These risks are discussed more fully in the section entitled “Risk Factors.” These risks include, among others, the following:
| ● |
We depend substantially on the successful commercialization of our drug candidates in the future, which may fail to materialize or may experience significant delays. |
| ● |
We currently do not generate any revenue from the commercial sales of drug candidates and we may not become profitable when expected, or at all. |
| ● |
We have incurred significant net losses and net operating cash outflows since our inception and expect to continue to incur significant net losses for the foreseeable future. |
| ● |
Our ability to continue as a going concern requires that we obtain sufficient funding to finance our operations, which may not be available on acceptable terms, or at all. A failure to obtain this necessary capital when needed could force us to delay, limit, reduce, or terminate our drug development or commercialization efforts. |
| ● |
Unstable market and economic conditions may have serious adverse consequences on our business, financial condition, results of operations, and prospects. |
| ● |
We have a limited operating history, which may make it difficult to evaluate our current business and predict our future performance. |
| ● |
We may encounter difficulties in managing our growth and expanding our operations successfully, which could adversely affect our business, financial condition, results of operations, and prospects. |
| ● |
Changes in government regulation or in practices relating to the pharmaceutical and biotechnology industries, including potential healthcare reform, could decrease the need for our drug candidates, or make it more difficult to obtain regulatory approvals for our drug candidates and commercialize them. |
| ● |
Our internal computer systems, or those used by any CROs or other third-party contractors or consultants we may engage, may fail or suffer security breaches. |
| ● |
We manufacture all of our drug candidates ourselves, and intend to manufacture most, if not all, of any approved drugs ourselves as well, which could have a material adverse effect on our business, financial condition, results of operations, and prospects. |
| ● |
Delays in completing and receiving regulatory approvals for our manufacturing facilities could delay our development plans or commercialization efforts, which could harm our business. |
| ● |
Damage to, destruction of, or interruption of production at our manufacturing facilities would negatively affect our business and prospects. |
| ● |
Significant or sustained inflation could adversely affect our business, financial condition, and results of operations. |
| ● |
Our future success depends on our ability to retain key executives and to attract, train, retain, develop, and motivate qualified and highly skilled personnel. |
| ● |
Our business and operations have been affected by and could be materially and adversely affected in the future by the effects of health epidemics and pandemics, which could also cause material adverse effects on the business and operations of third parties on which we rely. |
| ● |
There is significant uncertainty associated with our drug candidates and their viability as a commercial product. |
| ● |
We have not previously obtained any regulatory approval for a drug candidate and we may be unable to obtain or may be delayed in obtaining regulatory approval for any of our drug candidates. |
| ● |
Preclinical and clinical development of drug candidates involves a lengthy and expensive process with an uncertain outcome, and we are unable to predict if or when we will successfully develop or commercialize any of our drug candidates. |
| ● |
Clinical trials of our drug candidates may fail to demonstrate safety and efficacy to the satisfaction of regulatory authorities, or may not otherwise produce positive results, which may cause us to incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of our drug candidates. |
| ● |
If we are not able to obtain, or experiences delays in obtaining, required regulatory approvals, we will not be able to commercialize our drug candidates, and our ability to generate revenue will be materially impaired. |
| ● |
Any of our drug candidates, if approved, would continue to be subject to ongoing or additional regulatory obligations and regulatory review, which may result in significant additional expense and we may be subject to penalties if we fail to comply with regulatory requirements or experience unanticipated problems with our drug candidates. |
| ● |
Even if we are able to commercialize any approved drug candidates, the drugs may become subject to national or other third-party reimbursement practices or unfavorable pricing regulations, which could harm our business. |
| ● |
Our drug candidates, if approved in the future, may fail to achieve the degree of market acceptance by physicians, patients, third-party payors and others in the medical community necessary for commercial success and the market opportunity for the drug candidate may be smaller than we estimate. |
| ● |
As a company, we have no experience in launching and marketing drugs. If we are unable to develop sales, marketing and distribution capabilities or enter into sales, marketing and distribution agreements or arrangements with third parties, we may not be successful in commercializing any drugs, if approved, or generating drug candidate sales revenue. |
| ● |
We face substantial competition from other pharmaceutical and biotechnology companies, and our operating results may suffer if we fail to compete effectively. |
| ● |
If we are unable to obtain and maintain sufficient patent protection for our drug candidates through intellectual property rights, or if the scope of such intellectual property rights obtained is not sufficiently broad, third parties could develop and commercialize products similar or identical to our products, and our ability to commercialize our approved drugs successfully may be adversely affected. |
| ● |
We do not satisfy all continued listing requirements of Nasdaq. There can be no assurance that we will be able to comply with the continued listing requirements of Nasdaq. |
| ● |
The price of our Common Stock may be volatile. |
Overview
We are a clinical-stage pharmaceutical company pioneering the discovery, development, and commercialization of novel clean-surfaced nanotechnology (“CSN®”) therapeutics. CSN® therapeutics are comprised of atoms of transition elements that, when assembled in nanocrystal form, possess unusually high, unique catalytic activities not present in those same elements in bulk form. These catalytic activities drive, support, and maintain beneficial metabolic and energetic cellular reactions within diseased, stressed, and damaged cells.
Our patent-protected, proprietary position affords us the potential to develop a broad and deep pipeline of novel CSN therapeutics to address a range of diseases with high impact on human health. We innovated an electro-crystal-chemistry drug development platform that draws from advances in nanotechnology, plasma and quantum physics, material science, and biochemistry. Our platform process results in nanocrystals with faceted structures and surfaces that are free of the chemical surface modifications that accompany other production methods. Many traditional methods of nanoparticle synthesis involve the unavoidable deposition of potentially toxic organic residues and stabilizing surfactants on the particle surfaces. Synthesizing stable nanocrystals that are both nontoxic and highly catalytic has overcome this significant hurdle in harnessing transition metal catalytic activity for therapeutic use. Our clean-surfaced nanocrystals exhibit catalytic activities many-fold higher than other commercially available nanoparticles, produced using various techniques, that we have comparatively evaluated.
We have multiple drug assets currently in development and/or clinical trials for applications primarily in neurology. Our development and clinical efforts are currently focused on addressing the high unmet medical needs in central nervous system disorders including amyotrophic lateral sclerosis (“ALS”), multiple sclerosis (“MS”), and Parkinson’s disease (“PD”).
The Clene Approach
The Clene approach to drug development is innovation focused and scientifically driven.
| ● |
Innovation focused. There are a significant number of diseases with a high impact on human health that have proven exceedingly challenging for traditional small-molecule or biologic drug development approaches. Our approach involves the innovation of highly catalytically-active therapeutic nanocrystals with novel mechanisms of action that result from proprietary advances in nanotechnology, plasma and quantum physics, biochemistry, and materials science. This platform affords us the ability to make new drug modalities targeting a wide range of diseases that have eluded intervention using traditional small molecule or monoclonal antibody approaches. |
| ● |
Scientifically driven. Clear scientific rationale and sound experimental design drive our discoveries, from basic science to clinical trials. We believe we have established ourselves as an industry leader in position for the development of therapeutic catalytic nanocrystals. We have deep knowledge of the chemical properties, safety profiles, and catalytic abilities of transitional metal nanocrystals and have proven abilities to produce concentrated, stable, highly active, clean-surfaced nanocrystal suspensions using efficient, “green,” scalable processes. In so doing, we are establishing new classes of nanotherapeutics with the potential to address some of the most serious diseases affecting human health. |
Strategy and Leadership
Our management team is key to the successful execution of this strategic plan and fulfillment of our business model. Our exceptional team brings extensive expertise and industry experience to their roles in leading the Company skillfully and effectively. The members of the executive team have established track records in scientific innovation, early and late-stage pharmaceutical development, commercialization, marketing, and the generation and protection of intellectual property.
Our innovation of CSN therapeutic candidates places us at the forefront of novel drug development for a host of high impact, high unmet need human diseases. As we lead the development of CSN therapeutics, our business strategy can be encapsulated by the following:
| ● |
First mover advantage. We believe that our proprietary knowledge of the processes needed to manufacture clean-surfaced, highly faceted, catalytically active nanocrystals, and of the resulting toxicological and physicochemical properties associated with these nanocrystals, places us in a leadership position in the innovation and development of new candidate therapeutics for diseases that have proven to be extremely difficult to target using traditional methods. |
| ● |
Wide range of applicability. Energy metabolism is a fundamental mechanism in all living cells, and CSN therapeutics that improve cellular energetic production and utilization have the potential to be applied to many different disease states and cell types. An advantage of this approach is that a single drug candidate can be developed to hit multiple targets in multiple diseased cell types, presently being investigated across multiple clinical trials with our lead asset, CNM-Au8®, a catalytically-active gold nanocrystal suspension. We continue to explore ways in which the unique mechanisms of action of CSN therapeutics can be applied across different diseases. |
| ● |
Flexibility and tunability. Catalytic activities are determined by the shape, faceting, size, and chemical composition of nanocrystals. Our CSN platform has demonstrated flexibility in its ability to make, for instance, both pure gold and gold-platinum nanocrystals of consistent and reproducible shapes and sizes, in addition to making solutions of ionic zinc and silver. Because of the ease with which new single elemental and composite nanocrystals can be made of varying shapes and sizes using our proprietary techniques, we plan to continue developing a wide range of CSN therapeutics to generate a deep pipeline of drug candidates to treat a host of different diseases. |
Drug Candidates
Our CSN therapeutic candidates aim to address high unmet medical needs in several disease areas including primarily:
| (1) | disease modification of central nervous system disorders, including ALS, MS, and PD; |
| (2) | the treatment of infectious diseases; and |
| (3) | accelerated wound healing and scar formation. |
In addition to the development of catalytically-active, faceted, clean-surfaced nanocrystals, our electro-crystal-chemistry platform can produce ionic solutions of various transition elements including silver, zinc, and others—elements which have proven historical utility in the treatment of disease.
| ● |
CNM-Au8, our lead asset, is a highly concentrated aqueous suspension of catalytically-active, clean-surfaced, faceted gold nanocrystals. CNM-Au8’s mechanism targets mitochondrial dysfunction by catalyzing the production of a key metabolite, nicotinamide adenine dinucleotide (“NAD+”), that drives energy in the form of adinosine triphosphate (“ATP”) production in diseased cells. In addition, the catalytic activity of CNM-Au8 has been shown to have potent anti-oxidant effects. In this manner, treatment with CNM-Au8 is hypothesized to help neurons circumvent programmed cell death pathways that are triggered by energetic deficits, oxidative stress, and accumulation of misfolded proteins common to neurodegenerative diseases. CNM-Au8 is therefore hypothesized to act as a neuroprotective and remyelinating therapy in neurodegenerative disease states by: (1) driving, supporting, and maintaining beneficial metabolic and energetic cellular reactions within diseased, stressed, and/or damaged cells, (2) directly catalyzing the reduction of harmful, reactive oxygen species (“ROS”), and (3) promoting protein homeostasis via activation of the heat shock factor-1 pathway, recognized to dampen the cytotoxicity caused by misfolded and denatured proteins, which are known to occur ubiquitously in neurodegenerative diseases. We believe that CNM-Au8 is the only drug candidate in development with these unique catalytic mechanisms of action using gold nanocrystals. |
| ● |
CNM-ZnAg is a broad-spectrum antiviral, antibacterial agent comprised of zinc (Zn2+) and silver (Ag+) ions under development to treat infectious disease and to provide immune support for symptom resolution. Zn2+ and Ag+ ions are produced in aqueous solutions using our electrochemistry manufacturing platform; combining Zn2+ and Ag+ ions made in this manner leads to enhanced bioavailability of the ions and potentially, synergistic immune system effects. |
| ● |
CNM-AgZn17 is a gel polymer suspension of Zn2+ and Ag+ under development for treatment of infectious diseases and to support wound healing. We have demonstrated in in vitro assays that CNM-AgZn17 has broad-based anti-viral and anti-bacterial activity against common and antibiotic resistant pathogens such as Methicillin-resistant Staphylococcus aureus. We have also shown enhanced wound healing benefits in animal models of diabetic wound healing and decreased scar formation following burns. |
Dietary Supplements
Our patented electrochemistry manufacturing platform further enables us to develop very low concentration dietary supplements to advance the health and well-being of broad populations. These dietary supplements can vary greatly and include nanocrystals of varying composition, shapes and sizes as well as ionic solutions with diverse metallic constituents.
Dietary supplements are marketed and distributed through our wholly owned subsidiary, dOrbital, Inc. (“dOrbital”), or through an exclusive license with 4Life Research LLC (“4Life”), an international supplier of health supplements, stockholder, and related party. These include:
| ● |
rMetx™ (ZnAg Immune Boost) by dOrbital, is an aqueous zinc-silver ion dietary (mineral) supplement made using our electrochemistry manufacturing platform with bioactive immune-supporting properties. rMetx is sold through dOrbital, and a substantially similar product under the tradename, Zinc Factor™, is sold by 4Life under a supply agreement. |
| ● |
KHC46 (Gold Factor™) by 4Life, is an aqueous gold dietary (mineral) supplement of very low-concentration Au nanoparticles produced using our electrochemistry manufacturing platform. KHC46 has different production methods and uses different devices resulting in different physiochemical properties from our lead drug candidate, CNM-Au8. KHC46 is licensed exclusively to 4Life for worldwide marketing and distribution. |
Clinical Development Pipeline
We have completed clinical trials in ALS, MS, and PD and have several ongoing or completed clinical trial extensions and expanded access programs (“EAPs”):
| ● |
Amyotrophic Lateral Sclerosis. We completed the following clinical programs in ALS: (i) the HEALEY ALS Platform Trial, a Phase 2 clinical trial to evaluate the safety and efficacy of CNM-Au8 in patients with ALS; and (ii) RESCUE-ALS, a Phase 2 proof-of-concept clinical trial to evaluate the efficacy, safety, pharmacokinetics, and pharmacodynamics of CNM-Au8 in patients with early symptomatic ALS. Long-term open-label extensions (“OLE”) of both the HEALEY ALS Platform Trial and RESCUE-ALS are ongoing. We also support compassionate use EAPs for patients with ALS, including (i) an EAP launched in partnership with the Sean M. Healey & AMG Center (“Healey Center”) for ALS at Massachusetts General Hospital, which is closed to new enrollment but remains ongoing for current participants, (ii) a second EAP launched in partnership with Massachusetts General Hospital that includes centers across the United States (“U.S.”) and will enroll up to 200 participants, and (iii) an upcoming EAP in collaboration with Columbia University and Synapticure, a neurology specialty telehealth clinic, which will be funded by a four-year grant from the National Institute of Neurological Disorders and Stroke, a division of the National Institute of Health. |
| ● |
Multiple Sclerosis. We completed the following clinical programs in MS: (i) the first dosing cohort of REPAIR-MS, an open-label, investigator blinded Phase 2 clinical trial which demonstrated target engagement of CNM-Au8 on the brain’s energy metabolites, with a second dosing cohort currently ongoing in participants with non-active progressive MS; (ii) VISIONARY-MS, a Phase 2 clinical trial for the treatment of visual pathway deficits in chronic optic neuropathy to assess the efficacy, safety, tolerability, and pharmacokinetics of CNM-Au8 for remyelination in stable relapsing MS; and (iii) an open-label long-term extension (“LTE”) of VISIONARY-MS for participants in Australia with follow-up through 144 weeks from randomization. |
| ● |
Parkinson’s Disease. We completed REPAIR-PD, an open-label, investigator blinded Phase 2 clinical trial which demonstrated target engagement of CNM-Au8 on the brain’s energy metabolites. |
The chart below reflects the respective stages of clinical programs.
Our CSN Therapeutics Platform
We have developed a new pharmaceutical technology, CSN therapeutics. By uniting concepts from electrochemistry, nanotechnology, plasma and quantum physics, material science, and biochemistry, we have created and refined a proprietary electrocrystallization method that results in single component or multiple component nanocrystals of the transition elements that are clean-surfaced, highly faceted, and biologically catalytically active (see Figure 1 for example nanocrystals). These nanocrystals can be concentrated as aqueous suspensions and orally administered. We are also able to produce ionic solutions of various transition elements utilizing our electrochemistry manufacturing platform. Once in the gastrointestinal system, nanocrystals pass into the blood stream and accumulate in organs such as the liver, kidneys, and spleen, with lower amounts crossing the blood-brain barrier and reaching the brain, spinal cord, and cerebrospinal fluid. Nanocrystals can remain active within the body for days before they are eliminated via the hepatobiliary-fecal system as well as via the urinary system.
Once inside the body, CSN therapeutics cross cellular membranes and enter cells where they directly donate and receive electrons within biological systems. In this way, each nanocrystal acts as a potent catalyst which can drive, support, and maintain beneficial metabolic and energetic cellular reactions within diseased, stressed, and damaged cells. We believe these catalytic, nanocrystal-based therapeutic drugs represent a novel approach to drug development, substantially different from the standard paradigm of small-molecule drugs and large-molecule biologics. Unlike traditional pharmacological approaches, which are limited to single targets or specific signaling pathways, our technology platform has produced metallic nanocrystals that are beneficial through multi-modal activities in multiple cell types across multiple diseases. By utilizing cellular catalysts to support energetic reactions within cells, we believe this technology represents a revolutionary advance in the treatment of the underlying pathophysiology of neurodegeneration and related diseases associated with energetic failure.
Figure 1. Representative CSN Therapeutic Nanocrystals
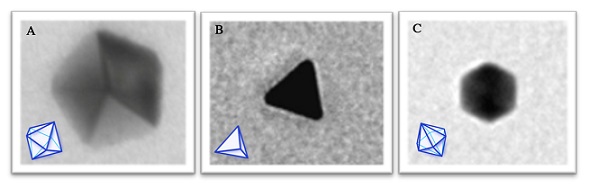
Figure 1. Representative transmission electron micrographs of the commonly observed crystalline shapes of gold nanocrystals (CNM-Au8) resulting from our CSN therapeutic platform. Insets are wireframes illustrating each classic shape: A, pentagonal bipyramid; B, tetrahedron; and C, hexagonal bipyramid. These nanocrystals are 10-13 nm in diameter.
Catalytically-Active Nanocrystals
A catalyst lowers the activation energy of a chemical reaction in such a way as to accelerate the rate of the reaction, without being consumed in the reaction. In doing so, it does not change the equilibrium of the substrates and products, and it can catalyze both forward and reverse reactions until homeostasis, or a balance of substrates and products, has been achieved.
Several industrial uses of metal nanocrystals have been discovered, but to our knowledge, we believe we are the only company currently developing catalytically-active nanocrystals to directly modulate biological systems as therapeutic drug candidates. Prior to our invention of the CSN therapeutic platform, the methods employed to make stable nanoparticles required the use of organic solvents or capping agents, which would contaminate the surfaces of the nanoparticles and were substantially difficult to remove. Multiple conflicting reports exist in scientific literature regarding the toxicity of these nanoparticles, ranging from reportedly non-toxic to highly toxic to living organisms. We believe this lack of consistency may have been due to the varying degrees to which different nanoparticle preparations were contaminated with organic reagents, leading to observed toxic effects. Because our electrocrystal chemistry method does not involve the use of any organic solvents or reduction chemicals, we have observed that our nanocrystals possess substantially higher catalytic activity in living organisms than those reported for nanoparticles made using other methods. Nonclinical toxicology studies completed with our lead asset, CNM-Au8, have demonstrated no adverse effect levels (“NOAELs”) up to maximum feasible dosing levels.
Transition metal nanocrystals are surface catalysts. Unlike enzymes, which are protein catalysts that lower activation energies using active site binding pockets, metal nanocrystals carry out their catalytic activities on their surfaces, where they act as exceptionally efficient electron donors and receivers. For this reason, unmodified, clean surfaces that are free of contaminating chemicals are extremely important for catalytic activity. The facets and vertices of the nanocrystals serve as the surface areas where electron exchange can take place. Metal nanocrystals have been shown to have a variety of different catalytic activities, from superoxide dismutase, peroxidase, and catalase-like activities for reducing ROS, to reactions involving the oxidation of glucose, ascorbic acid, or the energetic metabolite nicotinamide adenine dinucleotide (“NAD”). Figure 2 shows an illustration of catalysis, with a single gold nanocrystal converting molecules of nicotinamide adenine dinucleotide hydride (“NADH”) in the background into NAD in the foreground. Gold nanocrystals have been described as electron reservoirs because their surfaces can both readily accept and donate thousands of electrons per second in order to catalyze biochemical reactions, allowing them to accelerate reaction rates to extraordinarily high levels. For example, the conversion of NADH to NAD is usually very slow at room temperature, but upon addition of our gold nanocrystal suspension, CNM-Au8, we have observed the very rapid conversion of NADH into NAD. Importantly, the NAD reaction drives ATP production in both the mitochondrion as well as in the cytoplasm, via a reaction called glycolysis. ATP is the universal currency of energy in all living things; without the ability to convert NADH to NAD and vice versa, cells would be quickly depleted of ATP energy stores and die. CSN therapeutics capture the natural, extraordinary catalytic activities of faceted, clean-surfaced nanocrystals to produce metabolites of high energetic or protective value to the cell.
Figure 2. Catalytically-Active Nanocrystal Mechanism Representation
Figure 2. Illustration of catalytic activity (Not to scale). A pentagonal bipyramidal gold nanocrystal is shown with its electron cloud to represent the ability of the nanocrystal to rapidly exchange electrons with substrates interacting with its surface. In the background, NADH molecules drawn as dark chemical ball-and-stick figures are catalytically converted into NAD in the foreground as bright pink ball-and-stick figures. A pink and blue mitochondrion on the left can use available NAD for the generation of ATP (Illustrated by Ella Maru).
Our Focus on Central Nervous System Disorders
Over the past several decades, traditional small molecule and biologic drug development approaches have suffered serious setbacks in the attempts to address nervous system disorders. A likely contributor to these setbacks is the multifactorial mechanisms underlying nervous system disorders themselves, which are sufficiently complex they may not be amenable to “one drug-one target” disease modification. In the face of these failures, we believe our new paradigm of nanocrystal drug development, producing novel drugs with unique catalytic, multi-modal mechanisms of action, is advantageous.
Multiple lines of evidence now point to energetic failure as a key contributor to neurodegenerative disease. Neurons, and their associated support cells, in particular oligodendrocytes (“OLs”), are amongst the highest energy-consuming cells in the body: the brain represents only two percent of human body weight, yet it consumes over twenty percent of the body’s metabolic energy. As humans age, the ability of cells to convert food into energy in the form of ATP becomes less efficient. Eventually, the nervous system’s demand for ATP surpasses the cells’ ability to supply it, and consequently neurons begin to fail and die. Genetic and environmental factors determine which neuronal types are most susceptible to energetic failure in any individual. In PD, dopaminergic and other neuronal cell types manifest mitochondrial failure, leading to impaired energy production. In ALS, mitochondrial dysfunction is considered a hallmark of both sporadic and familial ALS, and several genetic causal variants of ALS have been linked to dysregulated neuronal energy metabolism. In MS, the cells capable of remyelinating damaged axons have been shown to be under metabolic stress, rendering them incapable of undergoing the energetically demanding process of repairing damaged myelin. Pathophysiology supports the need for increased energy production and utilization to protect neuronal health and slow neurodegenerative disease progression.
Our preclinical work has shown that CNM-Au8 nanocrystals cross the blood-brain barrier to potentially protect multiple central nervous system cell types, with demonstrated benefits including: OLs receive an energetic boost sufficient to drive myelin production, and dopaminergic, hippocampal, and cortical neurons improve energy production and utilization sufficient to enhance survival and maintain function in response to multiple disease-relevant stressors. Human astrocytes derived from patients with ALS have the capacity to kill motor neurons when grown in a co-culture, and these motor neurons exhibit markedly reduced toxicity when co-cultures are treated with CNM-Au8. By their very nature, faceted, clean-surfaced nanocrystals with catalytic capabilities circumvent many of the challenges that have previously plagued pharmaceutical drug development for central nervous system disorders. Importantly, their catalytic mechanism produces several useful energetic metabolites while reducing the presence of harmful ones. These mechanisms are well suited to address the complex failures that occur in neurodegenerative diseases on multiple levels and within multiple central nervous system cell types.
We believe the innovation of CSN therapeutics positions us to address the most significant challenge posed by numerous central nervous system diseases. Unlike the “one drug—one target” model, faceted clean-surfaced nanocrystals act by multiple mechanisms to enhance mitochondrial function, while simultaneously and independently reducing oxidative stress and stimulating protein homeostasis inside central nervous system cells. Each nanocrystal is capable of exchanging thousands of electrons per second, potentially addressing deficits in diseased central nervous system cells in a manner that does not further deplete the cells of their internal energy stores. We believe our studies show that CSN therapeutics support the cells of the central nervous system with the basic building blocks of energy they require to function normally, thereby replenishing cellular energetic deficiencies.
CNM-Au8 and Restoration of Energetic Metabolism in ALS, MS, and PD
Mechanism of Action
CNM-Au8 is a concentrated, orally-delivered suspension of pure gold nanocrystals in pharmaceutical grade water buffered with sodium bicarbonate. A single 60 ml dose at 30 mg contains over one hundred trillion nanocrystals. The median feret diameter of CNM-Au8 nanocrystals is approximately 13 nanometers with each nanocrystal consisting of an estimated average of 70,000 gold atoms. CNM-Au8’s mechanism targets mitochondrial dysfunction by catalyzing the production of NAD+, a key metabolite that drives energy in the form of ATP production in diseased cells. In addition, the catalytic activity of CNM-Au8 has been shown to have potent anti-oxidant effects. In this manner, treatment with CNM-Au8 is hypothesized to help neurons circumvent programmed cell death pathways that are triggered by energetic deficits, oxidative stress, and accumulation of misfolded proteins common to neurodegenerative diseases. CNM-Au8 is therefore hypothesized to act as a neuroprotective and remyelinating therapy in neurodegenerative disease states by: (1) driving, supporting, and maintaining beneficial metabolic and energetic cellular reactions within diseased, stressed, and/or damaged cells, (2) directly catalyzing the reduction of harmful ROS, and (3) promoting protein homeostasis via activation of the heat shock factor-1 pathway, recognized to dampen the cytotoxicity caused by misfolded and denatured proteins, which are known to occur ubiquitously in neurodegenerative diseases. This unique mechanism of action is summarized in Figure 3.
Figure 3. Catalytic Biological Mechanism of Action
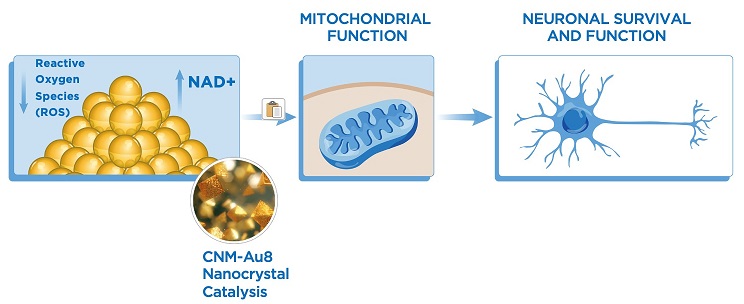
Figure 3. CNM-Au8-mediated catalysis increases intracellular NAD and ATP production and decreases oxidative stress. These catalytic activities enhance mitochondrial function and lead to a cascade of enhanced disease responses in neurons, OLs, and astrocytes – cell types that are extremely vulnerable to energetic deficiencies. CNM-Au8 thereby mediates remyelination and neuroprotective effects in neurodegenerative diseases such as ALS, MS, and PD.
One of the key metabolites catalyzed by CNM-Au8 is the oxidized form of NAD, NAD+ (Fig. 4). NAD+ and its reduced partner NADH are vital for driving cellular energy ATP-generating reactions in living cells (Fig. 4A). Brain imaging studies have shown the ratio of NAD+ to NADH typically decreases with aging. Lowered NAD+ levels in both the blood and brain have been associated with neurological diseases such as schizophrenia, MS, PD, and Huntington’s disease. Boosting NAD+ activity in neurodegenerative disease preclinical models has consistently demonstrated beneficial anti-aging and neuroprotective effects. CNM-Au8 exhibits higher catalytic activity for directly oxidizing NADH into NAD than any other commercially available gold nanoparticle we have tested (Fig. 4C, D). We have shown that treating cultured nervous system cells with CNM-Au8 increases their cellular pools of NAD+ and ATP, demonstrating that CNM-Au8 increases the energetic capacity of central nervous system cells (Fig. 4E, F). This optimization of ATP (Fig. 4F) allows OLs to increase myelin production, as well as help numerous other types of central nervous system cells resist environmental and disease-related stressors that would otherwise cause them to die.
The statistical analyses shown in Figure 4 were conducted by one-way analysis of variance (“ANOVA”) to compare means of each treatment group to mean of the vehicle control (corrected for multiple comparisons). The p-value (Fig. 4E, F) represents the probability of obtaining test results at least as extreme as the results observed in the assay, under the general assumption that there is no difference between the groups (the null hypothesis). The lower (smaller) the p-value, the greater the statistical significance of the observation, and the less likely the null hypothesis is true. The scientific community and regulatory authorities, such as the U.S. Food and Drug Administration (“FDA”), conventionally regard p-values of 0.05 or less to be significant when replicated in independent clinical trials. Consistently statistically significant preclinical results, such as those described here, are used to support investigative New Drug Applications (“NDAs”) to investigate the clinical effects of an investigational product.
One significant stressor shared by many neurodegenerative diseases is the accumulation of harmful ROS within neurons as their energetic demands begin to exceed their ability to produce enough ATP to carry out normal functions. Chronic oxidative stress, caused by accumulation of ROS, can overwhelm the mitochondrial systems that normally tightly regulate ROS levels. Accumulation of excess ROS damages cell membranes, allows calcium ion imbalances, and eventually leads to cell death.
Figure 4. NAD Oxidation and Biological Effects on ATP and NAD+
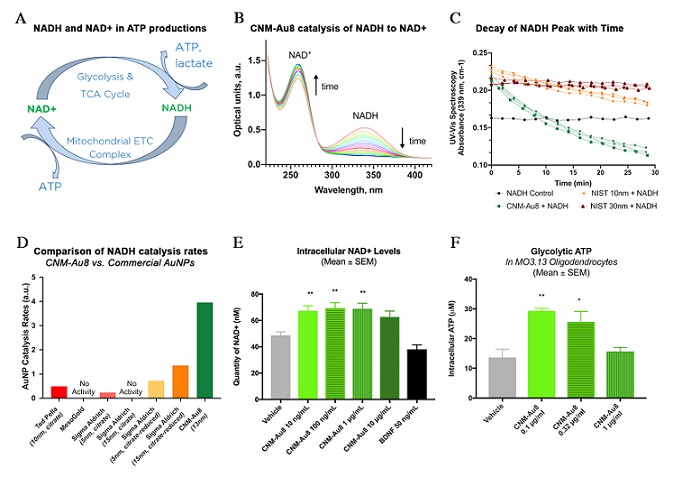
Figure 4. Energetic catalysis by CNM-Au8. A, The NAD-NADH reduction-oxidation couple plays a key role in both ATP-generating reactions, glycolysis and mitochondrial electron transport chain oxidative phosphorylation. B, Ultraviolet-visible light spectroscopy was used to show the catalytic activity of CNM-Au8 with time. As the reaction progresses, NADH is consumed, as demonstrated by the decrease in the NADH absorbance peak at 340 nm, while NAD+ is generated, as shown by the corresponding increase in the NAD+ absorbance peak at 260 nm. C, the rate of decay of the NADH absorbance peak is greater for CNM-Au8 than it is for citrate-reduced gold, nanoparticles of 10 nm (orange) and 30 nm (red) diameters (purchased from the National Institute of Standards and Technology), indicating that CNM-Au8 has a catalytic rate at least three-fold higher than National Institute of Standards and Technology comparators under the same reaction conditions. D, Catalytic rate of CNM-Au8 is demonstrably superior to several commercially available gold nanoparticles. Sigma Aldrich provides reactant-free, “citrate reduced” gold nanoparticles, in which extra procedures are used to clean the surfaces of reactants. “Citrate” gold nanoparticles may still have residual reactants present in the suspensions. E, Cellular NAD+ levels increase in response to CNM-Au8 treatment in primary rodent neuron-glial co-cultures. F, Cellular ATP levels increase in primary rodent OL cultures in response to CNM-Au8 treatment. Panels E-F, quantities shown are group means +/− SEM. One-way ANOVA, corrected for multiple comparisons, was used to compare the mean of each treatment group to the mean of the vehicle control; a statistically significant difference between treatment and vehicle is denoted by asterisks: *p < 0.05; **p < 0.01.
In addition to boosting NAD+ levels inside nervous system cells, CNM-Au8 directly acts to reduce ROS by directly catalyzing their reduction (Fig. 5). CNM-Au8 possesses anti-oxidative catalytic activity and has been demonstrated to directly reduce oxygen radicals in a superoxide dismutase-like manner, as well as convert hydrogen peroxide (“H2O2”) into water and oxygen in a catalase-like manner (Fig. 5A, B). Anti-oxidative activity for CNM-Au8 has been demonstrated in primary mouse OL cultures, in which basal levels of ROS were reduced with treatment (Fig. 5C). In a PD in vitro model, ROS generated by treating primary rodent dopaminergic cells with the neurotoxin 1-methyl-4-phenylpyridinium (“MPP”) was lowered in response to CNM-Au8 treatment in the presence of MPP (Fig. 5D). The statistical analyses shown in Figure 5 were conducted by one-way ANOVA to compare means of each treatment group to the mean of the vehicle control (corrected for multiple comparisons). The p-value (Fig. 5C, D) represents the probability of obtaining test results at least as extreme as the results observed in the assay, under the general assumption that there is no difference between the groups (the null hypothesis).
Previous drug development efforts for neurodegenerative diseases have included numerous antioxidants, all of which failed to show disease-modifying effects. We believe CNM-Au8 remains in a different class from standard antioxidants because, to our knowledge, no other antioxidant demonstrates catalytic ability to increase energetic metabolites NAD+ and ATP, while independently catalytically decreasing ROS.
Figure 5. Reduction of Reactive Oxygen Species
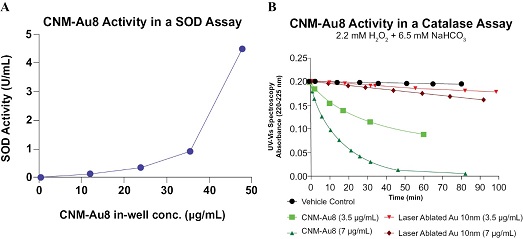
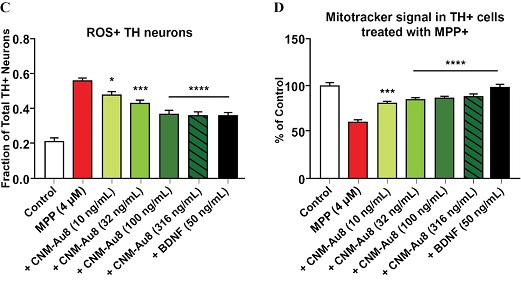
Figure 5. CNM-Au8 is a catalytically active antioxidant. A, SOD-like activity of CNM-Au8 on superoxide radicals was measured using a colorimetric SOD assay kit (Cayman Chemical). B, Decay of the absorbance peak of H2O2 as the dismutation of H2O2 takes place in the presence of CNM-Au8 (green) or comparator AuNPs of similar diameter (red) or no gold (black). C,D, Neurotoxin (MPP+) induced mitochondrial stress and death of dopaminergic neurons in primary E15 rat co-cultures is prevented by CNM-Au8 (green), as determined by TH+ cell number (not shown), reduction of ROS as measured as by the fraction of dopaminergic (“TH”) cells fluorescing with CELLROX Green signal, a marker of cytosolic oxidizing environment (C), and increased mitochondrial membrane potential (Mitotracker Red CMXRos) (D). Panels C-D, quantities shown are group means +/− SEM. One-way ANOVA, corrected for multiple comparisons was used to compare the mean of each treatment group of MPP with CNM-Au8 treatment to the mean of the MPP (4μM) alone treatment group; a statistically significant difference between each CNM-Au8 treatment group and MPP alone is denoted by asterisks: *p < 0.05; **p < 0.01, ***p < 0.001; ****p < 0.000. Untreated “Control” group is included to demonstrate the significant effect of MPP treatment to increase levels of ROS in TH neurons in Panel C and reduce mitochondrial membrane potential in Panel D, which was not included in the ANOVA analysis.
Previous drug development efforts in the neurodegenerative disease space have targeted misfolded protein aggregates as toxic drivers of disease; for example, alpha-synuclein in PD, amyloid beta in Alzheimer’s Disease, and TAR DNA binding protein 43 (“TDP-43”) in ALS. An important component of the mechanism of action of CNM-Au8 is its ability to dose-dependently reduce aggregated alpha-synuclein and TDP-43 in cellular models of PD and ALS, respectively (Fig. 6). We believe this activity is, at least in part, attributable to the robust induction of twenty gene transcripts of the Heat Shock Factor 1 pathway, which we observed in OLs in response to CNM-Au8 treatment (Robinson, et al. Nanocatalytic activity of clean-surfaced, faceted nanocrystalline gold enhances remyelination in animal models of MS. Sci Rep 10, 1936 (2020)) as well as due to an indirect cellular response to NAD upregulation, which has been shown to activate autophagic and proteostatic responses.
Figure 6. Reduction in Misfolded Protein Aggregates
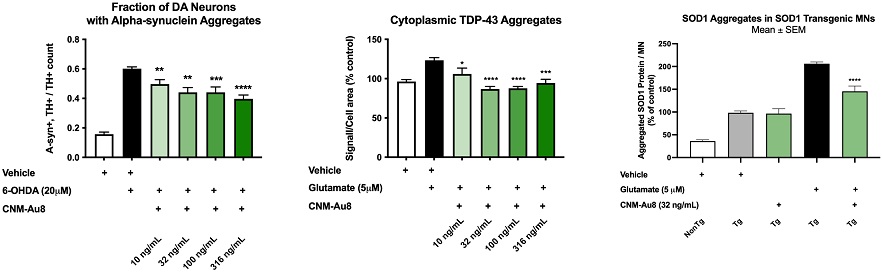
Figure 6. shows the dose-dependent reduction of three different types of protein aggregates in dopaminergic and spinal motor neurons that are typically found in PD (Fig. 6A), sporadic and familial ALS cases (Fig. 6B), and familial SOD1 ALS cases (Fig. 6C). In each of these assays, there was a concomitant dose-dependent increase in neuron survival and preservation of neurite network with CNM-Au8 treatment. These results demonstrate that CNM-Au8 reduces the quantity of toxic protein aggregates in in vitro models representing different neurodegenerative diseases. Group means plotted +/- SEM. * p < 0.05; ** p < 0.01; *** p < 0.001; **** p < 0.0001; treatment vs. vehicle, one-way ANOVA corrected for multiple comparisons.
In summary, CNM-Au8 exhibits a novel mechanism of action via its catalytic activities, involving:
| (1) | enhancement of energetic metabolism via increased production of NAD+ and ATP; |
| (2) | reduction of oxidative stress; and |
| (3) | enhancement of proteostatic, autophagic responses that reduce accumulation of toxic protein aggregates that are hallmarks of neurodegenerative diseases. |
Safety and Tolerability of CNM-Au8
Standard ICH M3(R2) toxicology studies were conducted on CNM-Au8 in four animal species, which yielded no toxicity findings resulting in NOAEL findings up to maximum feasible dosing. We completed a Phase 1 First-In-Human study of CNM-Au8 in 2016 to demonstrate it was safe for further clinical development, and to assess the pharmacokinetic profile at different dosing concentrations. The Phase 1 First-In-Human study of CNM-Au8 was a randomized, placebo-controlled, double-blind, escalating single- and multiple-dose study to evaluate the safety, tolerability, and pharmacokinetics of CNM-Au8 in healthy human volunteers. The study had two phases: a single-ascending dose (“SAD”) phase, where 40 subjects were randomized to CNM-Au8 (n=30) or placebo (n=10) at a 3:1 ratio in single dose escalating cohorts who received CNM-Au8 at 15 mg, 30 mg, 60 mg, or 90 mg, with follow-up study duration for each subject of 17 days; and a multiple-ascending dose (“MAD”) phase, where 46 subjects were randomized to CNM-Au8 (n=35) or placebo (n=11) in multiple dose cohorts who received CNM-Au8 at 15 mg, 30 mg, 60 mg, and 90 mg, with the duration of treatment at 21 days and follow-up of each subject at up to 50 days. The SAD phase was conducted first followed by the MAD phase of the study.
Pharmacokinetics analyses from the MAD phase showed that at the end of 21 days, the maximum concentration of gold in blood was determined to be 1.53 ng/mL, 1.98 ng/mL, 2.35 ng/mL, and 3.33 ng/mL for each group dosed with 15, 30, 60, or 90 mg, respectively. Pharmacokinetics analyses of the Phase 1 results demonstrated that CNM-Au8 has a half-life of 14-21 days. The end-of-study drug exposure levels in humans either matched or exceeded the equivalent exposure that demonstrated neuroprotection and remyelination efficacy in animal models.
Safety assessments revealed no significant findings. All doses used in the study were determined to be well-tolerated based on the frequency of reported treatment emergent adverse events (“TEAEs”). TEAEs occurred more frequently on placebo (86%) than in the CNM-Au8 dosing groups in both the SAD and MAD phases combined (75%). No subjects discontinued the study due to TEAEs and no SAEs were reported across any treatment group. The most frequently reported TEAEs were almost entirely of Grade 1 (mild) severity and transient. The most frequently reported TEAEs consisted of headaches, somnolence, fatigue, abdominal pain, diarrhea, nausea, and dizziness. We have continued to accumulate human safety exposure in our Phase 2 clinical trials and OLEs, LTEs, and EAPs (see “Overview—Clinical Development Pipeline” above). To date, we have not observed concerning or dose-limiting safety signals.
Amyotrophic Lateral Sclerosis
ALS Market Opportunities
ALS is the most prevalent adult-onset, progressive, and fatal neurodegenerative disorder of the neuromuscular system, affecting approximately 30,000 patients in the U.S. and over 200,000 patients worldwide, with an average life expectancy of only three to five years after initial diagnosis. ALS involves the progressive degeneration of motor neurons in the spinal cord and the brain, which are responsible for controlling voluntary muscle movement. This progressive loss of motor neurons leads to muscle weakness, loss of muscle mass, inability to control movement, and paralysis. The onset of disease for the majority of individuals with ALS occurs between the age of 40 and 60 and is more common in men. After the age of 65, the difference in incidence between males and females decreases. We estimate that global ALS sales will be greater than $1 billion by 2029.
ALS Current Therapies and Limitations
Current ALS treatment therapies are largely palliative, aiming only to provide temporary relief from symptoms without addressing the underlying disease progression. For example, one approach to the loss of respiratory function, which is the most common cause of ALS-related death, is non-invasive ventilation. Despite the great need for an effective disease-modifying treatment, and significant research efforts by the pharmaceutical industry to meet this need, there have been limited clinical successes and no curative therapies approved to date. Four therapeutic agents have been approved by the FDA for the treatment of ALS: riluzole, an anti-glutamatergic agent; edaravone, a free-radical scavenger; tofersen, an antisense oligonucleotide (for SOD1-ALS); and sodium phenylbutyrate and taurursodiol, an apoptosis inhibitor. However, these treatments are acknowledged to have limited disease-modifying effects and do not substantially halt or reverse the progressive nature of the disease: Riluzole extends participant lifespans by an average of only two to three months; edaravone slows the decline of the ALSFRS-R score, a clinical measure of functional decline, in only a small subset of participants at an early stage of disease; tofersen slows decline of certain clinical outcomes in patients with SOD1-ALS, which represents only a small percentage of ALS cases; and sodium phenylbutyrate and taurursodiol slowed the decline of the ALSFRS-R score and had longer median overall survival in a limited exploratory analysis in a Phase 2 trial, but in a subsequent Phase 3 trial did not demonstrate a statistically significant treatment benefit as measured by the ALSFRS-R score and quality of life patient-reported outcome assessments, including overall survival and respiratory function. The commercial promotion of sodium phenylbutyrate and taurursodiol was paused in March 2023, with anticipated future engagement with regulatory authorities and the potential voluntarily withdrawal of the drug from the market. An urgent unmet need clearly exists for the development of safe and effective disease-modifying therapies (“DMTs”) for ALS.
Potential Advantages of CNM-Au8 for ALS
We believe that CNM-Au8 has the potential to be a first-in-class disease modifying nanotherapeutic drug for ALS. In a human induced pluripotent stem cell (“iPSC”) model of ALS, CNM-Au8 demonstrated clearly superior human motor neuron protection compared to riluzole. Furthermore, oral delivery of CNM-Au8 to ALS model mice extended the median lifespan of these animals by over three times the lifespan extension attributed to edaravone or riluzole treatment reported in the literature. While the mechanism of action of edaravone shares one similar component with CNM-Au8, namely, reduction of oxidative stress, we believe the important difference in activity lies in CNM-Au8’s demonstrated potential to enhance energetic activity in diseased neurons as well as to significantly reduce oxidative stress. Furthermore, we believe the complex nature of many of the neurodegenerative diseases, including ALS, calls for a therapeutic drug with multimodal activity that can act to enhance the energetic profile of multiple central nervous system cell types; for this, CNM-Au8 may be uniquely suited to address the therapeutic challenges posed by such complicated and devastating diseases.
Summary of Nonclinical Pharmacology Neuroprotection Studies for ALS
Motor neurons progressively degenerate during the course of ALS. To demonstrate neuroprotection of motor neurons by CNM-Au8, in vitro neuroprotection assays were first used. Rat motor neurons were challenged with glutamate to induce excitotoxicity, or with amyloid beta 1-42 peptide (“A-beta”), which is toxic to motor neurons. In Alzheimer’s Disease, A-beta aggregates participate in the formation of amyloid plaques. CNM-Au8 treatment of motor neurons challenged with glutamate or with A-beta increased numbers of surviving motor neurons and preserved neurite networks in a dose-dependent manner.
Aggregation of misfolded proteins that display neurotoxic properties is a hallmark of many neurodegenerative diseases, including ALS. Accumulation of mis-localized, cytoplasmic TDP-43 in motor neurons is associated with over 90% of ALS cases, and TDP-43 aggregates have been shown to disrupt cellular functions in motor neurons. In neuron-glial co-culture assays, application of glutamate or A-beta to rat motor neurons causes TDP-43 aggregates to accumulate in the cytoplasm of motor neurons. Treatment of the glutamate- or A-beta-challenged motor neurons with CNM-Au8 significantly reduced the accumulation of TDP-43 aggregates in a dose-dependent manner.
In addition to animal models, iPSCs have emerged as a new technique for neurodegenerative disease modeling using human-derived cells. iPSCs can be generated from human skin or blood samples, and then differentiated in vitro into astrocytes and motor neurons. Using this technique, ALS patient-derived astrocytes were shown to be toxic to normal healthy human motor neurons. Introduction of CNM-Au8 to these toxic ALS patient astrocyte-motor neuron co-cultures resulted in a significant, dose-dependent rescue of human motor neurons and preservation of motor neuron neurite networks. Collectively, these results indicated that CNM-Au8 exerts motor neuron protection effects in several different models, including in response to excitotoxic stress, A-beta toxicity, and toxic astrocytes.
To investigate the efficacy of CNM-Au8 in an in vivo model of ALS, two studies were conducted in separate transgenic (SOD1G93A) mouse model strains that model the human SOD1 familial form of ALS. In a study using rapidly progressing SOD1G93A animals, CNM-Au8 treated animals showed significant reduction of brainstem atrophy and brainstem vacuolization normally seen in untreated SOD1G93A mice. In the study using slower-progressing SOD1G93A animals, CNM-Au8 treated animals showed significant treatment effects in a number of behavioral and functional tests, including overall clinical score, weights hold, static rod orientation time, and average wheel-running velocity. Median survival of CNM-Au8 treated animals significantly exceeded vehicle-treated controls by 23 days (approximately 20% of the animal’s expected life-span).
Clinical Development of CNM-Au8 as a Disease-Modifying Drug for ALS
Orphan Drug Status for ALS
The FDA granted orphan drug designation to CNM-Au8 for the treatment of ALS in May 2019. Following FDA orphan drug designation, sponsors may qualify for seven-year FDA-administered Orphan Drug Exclusivity, partial tax credits for research and development expenses, potential research and development grants, waived FDA fees, and protocol assistance from the FDA.
RESCUE-ALS
RESCUE-ALS was a Phase 2, randomized, double-blind, placebo-controlled trial of the efficacy, safety, pharmacokinetics, and pharmacodynamics of CNM-Au8 in early ALS patients. The trial was conducted over 36 weeks in 45 enrolled participants. The trial randomized participants 1:1 to treatment with CNM-Au8 at 30 mg daily or matching placebo on top of standard of care (riluzole). The primary endpoint of the trial was the percent change of the sum of Motor Unit Number Index (“MUNIX”) from baseline to week 36. MUNIX is a neurophysiological biomarker that estimates the number of functioning lower motor neurons serving selected muscles. Secondary endpoints were the change in forced vital capacity (“FVC”) and the absolute change in MUNIX values to week 36. Exploratory endpoints included multiple clinically relevant measures of ALS disease progression: ALS Functional Rating Scale Revised (“ALSFRS-R”) 6-point decline, ALS Specific Quality of Life (“ALSSQOL-SF”), and additional clinical and neurophysiology endpoints. Results were presented in November 2021 and published in eClinical Medicine in June 2023 (Vucic, S., et al. Efficacy and safety of CNM-Au8 in amyotrophic lateral sclerosis (RESCUE-ALS study): a phase 2, randomised, double-blind, placebo-controlled trial and open label extension. eClinical Medicine 60, 102036 (2023). https://doi.org/10.1016/j.eclinm.2023.102036). While the trial did not meet the primary or secondary endpoints of MUNIX and FVC at week 36, an efficacy signal was observed for the MUNIX endpoint at week 12 (p=0.057). Furthermore, in a pre-specified analysis in the subset of limb onset ALS, CNM-Au8 demonstrated a significant treatment effect in MUNIX at week 12 (p=0.0385) and a trend for improvement at week 36 (p=0.0741). Limb onset ALS accounts for approximately 70% of the ALS population. Clinically relevant exploratory endpoints through trial week 36 demonstrated significant benefits with CNM-Au8 treatment, including, slowing ALS disease progression (p=0.0125), decreasing the proportion of participants with an ALSFRS-R 6-point decline (p=0.035), and improving quality of life as measured by ALSSQOL-SF (p=0.018). In addition, CNM-Au8 treated participants consistently showed directional benefits (i.e., less decline) across measures of respiratory function and the motor function, albeit non-significantly. CNM-Au8 was found to be well-tolerated through 36 weeks of oral daily dosing. No SAEs related to CNM-Au8 treatment were reported. Treatment-emergent adverse events were predominantly mild-to-moderate in severity. The most frequently reported adverse events associated with CNM-Au8 treatment included aspiration pneumonia (n=3) and transient gastrointestinal distress (n=2).
RESCUE-ALS—Open Label Extension
In August 2023, we announced the 24-month data cut of the RESCUE-ALS long-term OLE, which represents a 24-month minimum follow-up for OLE participants from the last-patient, last-visit from the 36-week double-blind treatment period through July 2023. The 24-month data showed (i) cross-over adjusted median survival of 19.3 months using the rank-preserving structural failure time model (“RPSFTM”) (CNM-Au8 median survival of 34.2 months, placebo-adjusted median survival of 14.9 months); RPSFTM estimates the survival gained by receiving active treatment using the data from all study participants and then subtracts the benefit from ex-placebo participants switched to CNM-Au8 during the OLE to provide a comparison of CNM-Au8 versus placebo across the entire study period, and is a well-recognized method that has been used to estimate cross-over treatment effects in a recent ALS trial, and oncology and other rare disease trials; (ii) decreased risk of long-term all-cause mortality of 75% in participants originally randomized to treatment with CNM-Au8 compared to those originally randomized to placebo, after adjusting for benefit received by placebo after switching to CNM-Au8 (hazard ratio=0.252, 95% CI: 0.106 to 0.597; bootstrap log-rank p<0.001); (iii) unadjusted median survival of 10.1 months, when not accounting for the improvement by ex-placebo treated participants who switched to CNM-Au8 at the start of the OLE (CNM-Au8 median survival of 34.2 months; placebo median survival of 24.1 months); (iv) unadjusted decreased risk of long-term all-cause mortality of 46% in participants originally randomized to treatment with CNM-Au8 compared to those originally randomized to placebo, when not accounting for the improvement by ex-placebo treated participants who switched to CNM-Au8 at the start of the OLE (HR: 0.54, 95% CI: 0.25-1.1, log-rank p=0.09); (v) decreased risk of long-term mortality of 70% (Cox adjusted HR= 0.300, 95% CI: 0.09 to 0.79; p=0.03) in participants originally randomized to treatment with CNM-Au8 compared to matched placebo participants derived from the PRO-ACT database, which contains approximately 12,000 ALS patient records from multiple completed clinical trials; and (vi) 52% decreased risk of ALS clinical worsening events (the first occurrence of death, tracheostomy, assisted ventilation, or feeding tube placement) in the participants originally randomized to CNM-Au8 treatment versus original placebo (HR: 0.48, 95% CI: 0.23-1.0, log-rank p=0.049). CNM-Au8 was well tolerated without long term safety concerns or serious adverse events assessed as related to CNM-Au8 treatment; adverse events observed with CNM-Au8 have been characterized as transient and predominantly mild-to-moderate in severity.
HEALEY ALS Platform Trial
In September of 2019, the Healey Center for ALS at Massachusetts General Hospital selected CNM-Au8 as one of the first three drugs for inclusion in the first platform trial for the treatment of ALS. The HEALEY ALS Platform Trial is testing promising experimental therapeutics with a design that allows for the testing of multiple drugs simultaneously in order to rapidly identify and accelerate the development of novel therapies for ALS, while offering the advantages of reduced trial time, reduced costs and increased patient participation. The trial includes substantial financial support from philanthropic donors and the Healey Center, and provides access to over 50 expert ALS clinical trial sites across the U.S. from the Northeast Amyotrophic Lateral Sclerosis consortium. We contributed a direct fee to the Healey Center toward the clinical conduct of the trial and there were no additional licensing fees or milestone requirements. The Investigational New Drug (“IND”) application for the HEALEY ALS Platform Trial is held by Massachusetts General Hospital. We own all CNM-Au8 data while placebo data will be shared across the different treatment regimens within the trial. The trial was a Phase 2, multicenter, double-blind, placebo-controlled registrational clinical trial to assess the safety, efficacy, pharmacokinetics, and pharmacodynamics of CNM-Au8 in treating ALS. Participants were randomized 3:1 between active treatment and placebo with active treatment equally distributed between low dose (30 mg) CNM-Au8 and high dose (60 mg) CNM-Au8. The primary endpoint was rate of change in ALSFRS-R score from baseline to week 24 adjusted for mortality, with secondary endpoints of combined assessment of function and survival (“CAFS”), a combined joint-rank score based on survival and change in ALSFRS-R score from baseline to week 24, changes in slow vital capacity (“SVC”), and survival (time to death or death equivalent). Exploratory endpoints included time to clinical worsening events, voice pathology measurements, and biofluid-based pharmacodynamic and metabolic markers.
We announced topline results for CNM-Au8 in October 2022: the primary endpoint of slope of change in ALSFRS-R adjusted for mortality was not statistically significant (2% slowing, 95% CI: -20% to +19%) at 24 weeks. Secondary endpoints of CAFS and SVC were also not met at 24 weeks across the combined 30 mg and 60 mg CNM-Au8 doses. The prespecified exploratory analyses of the secondary survival endpoint demonstrated a >90% reduction in risk of death alone or in risk of death/permanently assisted ventilation at 24 weeks, when adjusted for baseline imbalances in risk (p=0.028 to p=0.075, unadjusted for multiple comparisons) with the CNM-Au8 30 mg dose. These survival results were statistically consistent for the 30 mg dose between the regimen only and full analysis sets, which included shared placebo from other regimens participating in the HEALEY ALS Platform Trial (Regimens A, B, and D). This survival signal is consistent with results previously reported by Clene in the Phase 2 RESCUE-ALS trial with CNM-Au8. CNM-Au8 was well-tolerated, and no drug-related serious adverse events or significant safety findings were reported. Based on these findings, Clene selected the CNM-Au8 30 mg dose for continued development in ALS.
In March 2023, we announced exploratory results for time to clinical worsening events based on prespecified risk adjusted Cox proportional hazard analyses. Treatment with the CNM-Au8 30 mg dose was associated with a 74% decreased risk (lower hazard) of the composite endpoint of time to clinical worsening events, which included the first instance of death, tracheostomy, initiation of permanently assisted ventilation (>22 hours per day of non-invasive ventilatory support), or placement of a feeding tube (p=0.035). Treatment with CNM-Au8 was also associated with statistically significant and directional trends across all prespecified time to clinical worsening event analyses (not adjusted for multiple comparisons), including (i) 98% decreased risk of death or permanently assisted ventilation (p=0.028), (ii) 95% decreased risk of death (p=0.053), (iii) 74% decreased risk of feeding tube placement (p=0.035), (iv) 63% decreased risk of assisted ventilation (p=0.058), (v) 84% decreased risk of ALS-related hospitalization (p=0.107), and (vi) 69% decreased risk of all-cause hospitalization (p=0.065). Supportive sensitivity analyses incorporating baseline neurofilament light chain (“NfL”) levels were similarly robust and resulted in increased effect sizes and smaller nominal p-values in the same “within regimen” analyses.
In June 2023, we announced a statistically significant reduction of plasma NfL levels across all CNM-Au8 (Regimen C) participants compared to placebo (CNM-Au8 or placebo, n=161). NfL is a key blood-based biomarker of neurodegeneration and is released from neurons following axonal injury, especially in people living with ALS, where higher levels of NfL have been found to predict more rapid decline in clinical function and increased mortality risk. Surrogate biomarkers such as NfL have recently been used to support the FDA approval of a drug for the treatment of ALS. The results are based on an analysis of the plasma NfL biomarker as the least-square (“LS”) mean change of the natural logarithm (“Ln”) of the plasma NfL values with the standard error (“SE”) for the 24-week difference: CNM-Au8 = -0.024 (SE: 0.024); placebo = +0.076 (SE: 0.042); CNM-Au8 versus placebo difference = -0.100 (SE: 0.048), p=0.040. Additional sensitivity analyses showed consistent reduction in plasma NfL levels versus placebo in specific populations generally considered at greater risk of ALS disease progression, including:
| ● |
Faster progressors (baseline pre-treatment ALSFRS-R slope >0.45 points/month (post hoc, n=107); difference of LS means on a Ln scale (SE) = -0.144 (0.058); p=0.014. |
| ● |
Definite or probable ALS diagnosis per El Escorial criteria (post hoc, n=125); difference of LS means on a Ln scale (SE) = -0.124 (0.054); p=0.023. |
| ● |
Higher mortality risk (baseline plasma NfL > median, post hoc, n=79); difference of LS means on a Ln scale (SE) = -0.150 (0.068); p=0.031. |
HEALEY ALS Platform Trial—Open Label Extension
In September 2023, we announced long-term survival data from the OLE phase of the HEALEY ALS Platform Trial for patients treated with CNM-Au8 30 mg for up to 133 weeks (n=59). These post hoc results showed a statistically significant 49% decreased risk of death for the covariate risk-adjusted analyses compared to matched placebo patients through long-term follow-up from the largest U.S. clinical database of previous ALS trials, PRO-ACT (covariate adjusted hazard ratio=0.510, 95% CI: 0.263 to 0.987, p=0.046). In a pooled analysis of the HEALEY ALS Platform Trial and RESCUE-ALS, participants originally randomized to CNM-Au8 30 mg (n=82) demonstrated a statistically significant 59% decreased risk of death compared to PRO-ACT matched placebo patients through long-term follow-up (covariate adjusted hazard ratio=0.406, 95% CI: 0.220 to 0.749, p=0.004).
In December 2023, we announced a statistically significant reduction of plasma NfL levels from baseline to 76 weeks in patients randomized to CNM-Au8 30 mg compared to patients treated with placebo for 24 weeks prior to crossing over to CNM-Au8 treatment. CNM-Au8 30 mg treatment reduced plasma NfL levels compared to baseline using a mixed model with repeat measures (“MMRM”), LS means on a Ln scale for the 76-week change from baseline of plasma NfL: CNM-Au8 = -0.075 (SE: 0.053); placebo = +0.098 (SE: 0.056); CNM-Au8 30 mg versus original placebo difference = -0.173 (SE: 0.076), p=0.023. Combined analyses of both CNM-Au8 doses (30 mg and 60 mg) also demonstrated nominally significant reductions in plasma NfL, CNM-Au8 versus placebo difference = -0.144 (SE: 0.066), p=0.029. We also announced the results of long-term survival analyses under the prespecified RPSFTM to account for the effects of CNM-Au8 in participants randomized to placebo who crossed-over to treatment with CNM-Au8. Under an assumption of a constant common treatment effect from CNM-Au8, treatment with CNM-Au8 demonstrated a 60% decreased risk of long-term all-cause mortality in participants originally randomized to treatment with CNM-Au8 compared to those originally randomized to placebo, after adjusting for the estimated benefit received after switching to CNM-Au8 (Cox hazard ratio=0.40, 95% CI: 0.19 to 0.85; p=0.017). CNM-Au8 was well-tolerated, and no drug-related serious adverse events or significant safety findings were reported.
Expanded Access Programs
Based on interest in the potential of CNM-Au8 to delay disease progression in ALS patients, clinical experts at Massachusetts General Hospital requested to use CNM-Au8 in two EAPs. An EAP is a pathway for a patient with an immediately life-threatening condition or serious disease or condition to gain access to an investigational medical product (drug, biologic, or medical device) for treatment outside of clinical trials when no comparable or satisfactory alternative therapy options are available. To qualify for an EAP within the U.S. the following should apply: (i) a patient has a serious disease or condition, or whose life is immediately threatened by their disease or condition, (ii) there is no comparable or satisfactory alternative therapy to diagnose, monitor, or treat the disease or condition, (iii) patient enrollment in a clinical trial is not possible, (iv) potential patient benefit justifies the potential risks of treatment, and (v) providing the investigational medical product will not interfere with investigational trials that could support a medical product’s development or marketing approval for the treatment indication. The EAPs are conducted under study protocols filed with the FDA, and commenced in September 2019 and September 2021. The EAPs will collect safety and pharmacokinetic data in ALS patients not otherwise eligible for clinical trials due to standard inclusion and exclusion criteria.
As of February 7, 2024, 84 participants had been enrolled in the first EAP that commenced in September 2019 with long-term exposure up to 228 weeks. Currently, 36 participants are active under the protocol. As of February 7, 2024, 179 participants had been enrolled in the second EAP that commenced in September 2021 with exposure up to 121 weeks. Currently, 153 participants are active under the protocol. An EAP provides additional safety data for FDA review and will be considered as part of the safety data package for CNM-Au8, and may provide supportive long-term safety data to support to an NDA submission in the future. Based on numerous requests from clinical trial sites, we increased the capacity of the second EAP to 200 participants with expansion to sites across the U.S. In February 2024, we announced results from two independent analyses of the pooled EAP data for CNM-Au8 30 mg compared to two independent datasets derived from PRO-ACT and the ALS/MND Natural History Consortium. The EAP dataset as of the date of the analyses was comprised of 256 participants with ALS, of which 220 EAP participants had all baseline values available for matching. These participants were matched for similar baseline characteristics compared to each non-CNM-Au8 treated control. The results in the EAP participants versus the matched controls demonstrated a significant survival benefit for each comparison:
| ● |
CNM-Au8 EAP vs. PRO-ACT matched controls: the baseline risk-adjusted hazard ratio demonstrated a 68% decreased risk of all-cause mortality with CNM-Au8 treatment (hazard ratio=0.320, 95% CI: 0.178 to 0.575, p=0.0001). |
| ● |
CNM-Au8 EAP vs. ALS/MND Natural History Consortium matched controls: the baseline risk-adjusted hazard ratio demonstrated a 57% decreased risk of all-cause mortality with CNM-Au8 treatment (hazard ratio=0.433, 95% CI: 0.282 to 0.663, p=0.0001). |
Analyses of the full dataset of 256 participants compared to the 220 matched controls also showed statistically significant survival benefits with log-rank p-values of p<0.0001 and p=0.006 for the PRO-ACT and ALS/MND Natural History Consortium matched controls, respectively.
In October 2023, in collaboration with Columbia University and Synapticure, a neurology specialty telehealth clinic, we were awarded a four-year grant totaling $45.1 million to support an EAP for CNM-Au8 treatment of ALS. The grant was awarded by the National Institute of Neurological Disorders and Stroke, a division of the National Institute of Health, under the Accelerating Access to Critical Therapies for ALS Act, which was signed into law in December 2021, with a call for increased public support of public-private partnerships that will innovate the development of, and increase access to, potential new treatments for ALS. We are currently working to sign a sub-award agreement with Columbia University, the prime awardee, prior to the commencement of the EAP.
RESTORE-ALS
We are presently planning the design of an international Phase 3 study of CNM-Au8 30 mg, RESTORE-ALS, with expert ALS clinical advisors and expect to initiate the trial in the second half of 2024, contingent upon funding. We plan to work closely with regulatory health authorities from the FDA, European Medicines Agency (“EMA”), ALS experts, and patient representatives to determine the proper path to support potential approval.
Additionally, we met with the FDA in the fourth quarter of 2023 and presented initial clinical and NfL biomarker results from our completed Phase 2 trials. We also presented the evidence of long-term survival data from these studies as well as the supportive safety data of more than 500 years of participant exposure to date without any identified safety signals (across ALS, MS, and PD). The FDA determined that the initial findings on biomarker NfL reduction from the Phase 2 trials were insufficient to support accelerated approval at that time. We are planning to provide supplemental data for further engagement with the FDA in the first half of 2024, including additional long-term clinical evidence and biomarker results of CNM-Au8’s treatment benefit in people living with ALS. We plan to demonstrate how CNM-Au8’s mechanism of action is linked to the reduction in NfL, and the association between observed NfL reductions and improved clinical outcomes in ALS patients, including increased survival time. We do not know when or if we will be able to file an NDA with the FDA which would be based on the outcome of our future meetings with the FDA and our accumulation of clinical evidence.
Multiple Sclerosis
MS Market Opportunities
MS is an inflammatory and degenerative disorder of the central nervous system affecting approximately 800,000 patients in the U.S. and an estimated 2.2 million people worldwide, and we estimate the market size to be approximately $23 billion. MS involves the immune-mediated destruction of the brain, optic nerves, and spinal cord, and results from autoimmune attacks on the myelin sheath, the protective covering wrapping the axons of neurons. When myelin is destroyed by autoinflammatory immune attacks, neurons become damaged and can ultimately die, leading to motor symptoms, cognitive disability, visual impairment and other neurological impairments.
MS typically begins between the age of 20 to 40 and is the leading cause of non-traumatic disability in young adults. Women are affected approximately three times as often as men, except in individuals with the less common, primary-progressive form of the disease, where there is no gender preponderance. MS is the most common inflammatory demyelinating disease, with a prevalence that varies considerably, from high levels in North America and Europe to low rates in Eastern Asia and sub-Saharan Africa. Despite currently available DMTs, approximately 26% of people with MS have developed a non-active, progressive form of the disease, for which there are limited approved, effective therapies, leading to significant loss of quality of life.
The diagnosis of MS is predominantly a clinical one that is aided by radiological tests (e.g., magnetic resonance imaging, or “MRI”). Other diagnostic methods include blood tests, evoked potential tests, lumbar puncture, and optical coherence tomography, which is a new technology for examining the effects of MS on the health of nerve cells and axons in the retina. Ongoing improvements in diagnostic technologies may increase the number of patients diagnosed with MS.
MS Current Therapies and Limitations
All the currently available DMTs for MS either treat the symptoms caused by MS or act to reduce the degree of autoimmune-mediated inflammation. Nearly all the current approved DMTs are approved for the treatment of relapsing forms of MS (“RMS”). They commonly act via immunosuppression or immunomodulation, and thereby act to minimize autoimmune-associated attacks on myelin. Immunomodulatory DMTs reduce the risk of having an inflammatory attack, referred to as a “relapse,” and can slow the development of disability in those patients having attacks (i.e., “active” patients). As a corollary, DMTs may possibly diminish the risk of conversion of RMS to secondary progressive MS. The newer DMTs have been shown to substantially reduce autoimmune-mediated attacks and to delay the progression of the disease in active patients. However, there are no drugs available which can reduce the ongoing loss of function (i.e., disease progression) in non-active (those no longer having attacks) MS patients. None of the approved DMTs have been shown to clinically improve remyelination of damaged and demyelinated axons in MS lesions. Currently available DMTs for the treatment of MS include: Injectable medications, Avonex (interferon beta-1a), Betaseron (interferon beta-1b), Extavia (interferon beta-1b), Copaxone (glatiramer acetate), Plegridy (peginterferon beta-1a), Rebif (interferon beta-1a), Glatiramer acetate generic equivalent (Glatiramer Acetate Injection), Glatopa (glatiramer acetate); Oral medications, Aubagio (teriflunomide), Gilenya (fingolimod), Tecfidera (dimethyl fumarate), Mavenclad (cladribine), Mayzent (siponimod); Infusion medications, Lemtrada (alemtuzumab), Novantrone (mitoxantrone), Ocrevus (ocrelizumab), and Tysabri (natalizumab). Advances in MS treatment with new B-cell depleting therapies, including ocrelizumab, have largely ameliorated inflammatory disease activity as measured by the reduction in risk of having relapses and the lack of occurrence of new gadolinium enhancing (inflammatory) lesions, as detected by MRI. However, despite the stabilization of MS disease activity in active MS patients by these agents for these MS patients, significant improvement in overall function has not been shown. Importantly, for the DMTs that have been approved to date, efficacy and safety are generally inversely correlated.
There is an increasing demand for better treatment strategies. Although current drugs for MS can reduce the risk of an inflammatory attack and slow down the progression of the disease in some MS patients, patients’ responses to drugs can be variable and suboptimal. For non-active MS patients, there is no available DMT that can substantially alter their progressive worsening. Also, the side effects of current MS drugs range from mild to serious, which may lead to reduced patient adherence.
Potential Advantages of CNM-Au8 for MS
We believe that CNM-Au8 has the potential to be a first-in-class remyelinating and neuroprotective disease-modifying nanotherapeutic drug for MS. CNM-Au8 supports neurologic functions by enhancing energetic activities in neurons and OLs that have been attacked by the disease. Unlike the current immunomodulating MS DMTs, CNM-Au8 is thought to act to directly support neuroprotection and remyelination by improving energetics, reducing harmful ROS and inducing protective heat shock protein mechanisms. CNM-Au8 is administered orally, penetrates the blood-brain barrier, and to date has a favorable safety, tolerability, and toxicology profile. Used alternately or in conjunction with standard immunomodulatory DMTs, CNM-Au8 treatment may improve patients’ quality of life and potentially reverse disease progression because of its enhancing energetic activities in neurons and OLs that have been attacked by the disease, even in patients whose inflammatory attacks are well-controlled.
Summary of Nonclinical Pharmacology Myelination Studies for MS
Myelination is a complex process resulting in the wrapping of axons by OL membranes containing specialized proteins and lipids. The resulting myelin sheath provides metabolic support to the axon and facilitates axonal electrical conduction, which in turn allows for central nervous system processing of motor, sensory, and higher order cognitive functions. During active myelination, OLs synthesize on the order of 100,000 proteins per minute and several thousand new lipid molecules per second, reflecting the significant energetic investment needed for biomass generation, and making this cell type among the most energetically demanding in the body. In MS, myelin is destroyed by autoimmune-mediated inflammatory attacks, and neurons whose axons were once protected and supported by myelin become damaged and can ultimately die. OL precursor cells are known to be present near MS lesions and can play a role in remyelination, but studies have shown that these cells are energetically compromised and remyelination is suboptimal in most central nervous system lesions.
Energetic deficits have been noted in the brains of living patients with MS using 31Phosphorus magnetic resonance spectroscopy (“31P-MRS”). In autopsied brains from MS patients, OL precursor cells near MS lesions displayed impaired mitochondrial complex activity and other energetic deficits. These energetic deficits play key roles in MS disease progression. CNM-Au8 is uniquely designed to directly address these important pathophysiological mechanisms.
We investigated the ability of CNM-Au8 to address OL energetic deficits, induce remyelination, and restore functional activities and motor behaviors in a comprehensive remyelination preclinical program involving multiple in vitro and in vivo assays to determine CNM-Au8 efficacy. The peer-reviewed results were published in February 2020 (Robinson, A.P., Zhang, J.Z., Titus, H.E. et al. (2020). Nanocatalytic activity of clean-surfaced, faceted nanocrystalline gold enhances remyelination in animal models of multiple sclerosis. Scientific Reports, 10(1):1936) and the studies were fully funded by us and were the result of collaborations among academic researchers from Northwestern University, George Washington University, and various other academic consultants and our employees. In Robinson et al. (2020), in vitro experiments on primary OL precursor cells demonstrated robust induction of myelin production by CNM-Au8. RNASeq analyses of CNM-Au8 treated OL precursors cells demonstrated that multiple transcripts for known myelination genes are upregulated, and that glycolytic activity and ATP production are also increased. Several in vivo experiments were also conducted to demonstrate that orally delivered CNM-Au8 results in increased remyelination in the brains and spinal cords of animals treated with cuprizone or lysolecithin, two agents that are known to strip neurons of myelin via different mechanisms.
Both orally delivered cuprizone or stereotactically injected lysolecithin are commonly used techniques to cause demyelination of the corpus callosum or spinal cord, respectively. Cuprizone, which is administered to rodents by including this agent in their chow, is a copper chelating agent that specifically causes mature OL death within multiple brain regions, including the corpus callosum. Maximal demyelination due to cuprizone feeding typically occurs within five weeks, which can be visually monitored and quantified using transmission electron microscopy. Lysolecithin injection results in the rapid degradation of myelin within a localized area of the spinal cord, observable using Luxol Fast Blue or toluidine staining for myelin with light microscopy, or also with transmission electron microscopy of the lesion, within a day of injury, allowing for the observation of remyelination within the induced lesion within the following weeks. Remyelination of the corpus callosum or spinal cord using either technique requires the migration of surviving OL precursor cells to the sites of demyelination, differentiation of these cells into mature myelinating OLs, and rapid generation of specialized proteins and lipids for formation of new myelin membrane wraps around axons in this energetically demanding process (Robinson et al., 2020).
In Robinson et al. (2020), multiple independent in vivo remyelination assays, using either cuprizone or lysolecithin as demyelination agents, were performed to demonstrate the remyelinating ability of CNM-Au8. For example, CNM-Au8 was provided either prophylactically, at the same time as the start of cuprizone feeding, or only after two weeks of cuprizone feeding, therapeutically, in order to allow demyelination to start to take place prior to administration of CNM-Au8. In both contexts, CNM-Au8 demonstrated greater recovery of myelin in affected brain areas than vehicle-treated controls. Furthermore, animals that were provided with CNM-Au8 only after full demyelination (five complete weeks of cuprizone treatment) had taken place displayed evidence of higher levels of mature myelin marker expression in their brains than vehicle controls, indicating that CNM-Au8 was not blocking the action of cuprizone but rather inducing recovery by stimulating the differentiation of OLs. Similar results were confirmed by the lysolecithin experiments, which indicated that myelin destroyed by a completely different mechanism could be recovered with the daily oral administration of CNM-Au8 for one or two weeks after focal demyelination by lysolecithin. Treatment with CNM-Au8 significantly improved not only the quantifiable detection of myelinated axons in the brains of experimental animals, but also mouse behaviors and functional movements in the open field test and kinematic assays. For example, quantitation of the number of myelinated versus unmyelinated axons in 587 transmission electron microscope images, averaging 84 images per treatment group (with 15 mice per treatment group, 7 treatment groups total), demonstrated a statistically significant recovery of remyelinated axons in therapeutically treated animals who were dosed with CNM-Au8 by gavage compared to vehicle treated, cuprizone-fed controls (p < 0.0001 using one-way ANOVA corrected for multiple comparisons). In independent demyelination model studies using lysolecithin, lesioned animals treated with CNM-Au8 exhibited a 43% mean increase in myelinated axons within lesions post-LPC injection compared to vehicle controls (p=0.15, unpaired t-test comparing CNM-Au8 treated rats to vehicle treated controls). Finally, in a cuprizone-mediated demyelination model study of both gross and fine motor behaviors, the group of animals receiving therapeutically delivered CNM-Au8 displayed detectable improvements in behaviors in both open field and fine motor kinetics assessments. Principal component analysis of gait metrics showed no statistical difference (p=0.47) between CNM-Au8 treated, cuprizone-fed animals compared to the sham treated group, whereas there was a detectable difference in vehicle-treated, cuprizone-fed animals and sham controls (p=0.032; two-way ANOVA) by the end of study at week 6. Figure 7 shows examples of the observed induction of myelination by CNM-Au8 from selected in vitro and in vivo experiments reported in Robinson et al (2020).
Figure 7. Remyelination Summary
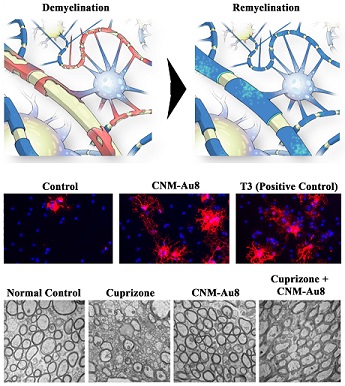
Figure 7. A summary of myelinating activities of CNM-Au8. Top row, Left: illustration of the demyelination (red) of a neuron’s axon (yellow) that occurs in MS. Right: Illustration of restored myelination along the axon (blue) provided by the OL (blue cell). Middle row: isolated primary mouse OL precursors treated with vehicle control (left), 3 μg/mL CNM-Au8, or positive control and myelin-inducing agent tri-iodothyronine. Cells are fixed and stained for Myelin Basic Protein (“MBP”), a marker of mature myelin in red, and the nuclear stain DAPI in blue, to reveal the presence of all OL precursor cells in the field of view. Many more cells expressing MBP are seen in the CNM-Au8 treated cells compared to vehicle-treated cells. Bottom row: transmission electron images of slices of corpus callosum of mice treated with, left to right: no cuprizone, cuprizone for five weeks, CNM-Au8 for five weeks, or cuprizone for five weeks and CNM-Au8 for the last three of the five weeks. Myelin can be seen as dark rings in each micrograph. Cuprizone treatment destroys myelin, while CNM-Au8 treatment alone does not change myelin. CNM-Au8 treatment of cuprizone-treated animals results in the recovery of myelin in the brains of these animals.
Clinical Development of CNM-Au8 as a Disease-Modifying Drug for MS
Based on safety findings in our Phase 1 clinical trial of CNM-Au8 and our robust preclinical remyelination data, we have launched two Phase 2 clinical trials, one of which is complete, to investigate the effects of CNM-Au8 in MS patients. We plan to work closely with regulatory health authorities from the FDA and EMA, MS experts, and patient representatives to determine the proper path to advance CNM-Au8 into Phase 3 clinical trials and potential future approval. We expect to meet with the FDA in an end of Phase 2 meeting in the second half of 2024.
REPAIR-MS
REPAIR-MS is a Phase 2, single-center, active-only, sequential group study to demonstrate central nervous system target engagement by examining the brain metabolic effects, safety, pharmacokinetics and pharmacodynamics of orally-delivered CNM-Au8 in patients who have been diagnosed with MS in vivo within 15 years of screening. These energetic metabolites are measured non-invasively and semi-quantitatively by utilizing 31P-MRS imaging with a 7 Tesla (“7T”) MRI scanner. A full volume head coil was used to collect whole brain spectral waveforms in ~600 voxels with a spatial resolution of 2 cm3 for the following metabolites: NAD pool (both NAD+ and NADH together), α-ATP, ß-ATP, γ-ATP, phosphocreatine, extracellular and cellular inorganic phosphate, uridine diphosphate glucose, phosphocholine, phosphoethanolamine, glycerophosphocholine, and glycerophosphoethanolamine. A partial volume head coil was used in the same patient cohort to measure occipito-parietal levels of individual NAD+ and NADH phosphorous metabolites to determine the ratio of NAD+/NADH.
REPAIR-MS is being conducted at the University of Texas Southwestern, a center with specialized capabilities for conducting and analyzing 7T 31P-MRS imaging studies, and was conducted in conjunction with the REPAIR-PD trial, with a pre-specified integrated analyses of both trials performed. REPAIR-MS was approved for clinical conduct by the FDA and commenced in January 2020, and we subsequently enrolled 13 relapsing MS participants in first dosing cohort with exposure to CNM-Au8 up to 18-weeks. REPAIR-MS is ongoing with the initiation of a second dosing cohort of up to 15 participants with non-active progressive MS. We anticipate enrollment concluding in the first half of 2024 with topline results available by the end of 2024.
Results were presented in August 2021 and published in the Journal of Nanobiotechnology in December 2023 (Ren, J., Dewey, R.B., Rynders, A. et al. Evidence of brain target engagement in Parkinson’s disease and multiple sclerosis by the investigational nanomedicine, CNM-Au8, in the REPAIR phase 2 clinical trials. J Nanobiotechnol 21, 478 (2023). https://doi.org/10.1186/s12951-023-02236-z). The pre-specified integrated analyses of REPAIR-MS and REPAIR-PD demonstrated a statistically significant increase in the primary endpoint, the mean change in the brain NAD+/NADH ratio (the ratio of the oxidized to reduced form of NAD), of 0.589 units (+10.4%) following 12 weeks of treatment with CNM-Au8 (p=0.037, paired t-test). Key secondary endpoints for the integrated analyses, mean change from baseline in the in the NAD+ and NADH fractions of the total NAD pool, were concordant with the primary endpoint, demonstrating the NAD+ fraction increased and the NADH fraction decreased (p=0.0264, paired t-test). The independent results for REPAIR-MS also demonstrated consistent trends toward improvement in the primary and secondary endpoints, although neither REPAIR-PD nor REPAIR-MS independently reached a level of statistical significance: the mean change in the brain NAD+/NADH ratio was 0.830 units (+14.3%) following 12-weeks of treatment with CNM-Au8 (p=0.145, paired t-test), and the secondary endpoint of mean change from baseline in the NAD+ fraction of the total NAD pool increased and the NADH fraction decreased (p=0.1157, paired t-test). Analyses of pre-specified exploratory endpoints demonstrated that homeostatic equilibrium was achieved across essential energetic metabolites, including ATP, cellular phosphorous (“Pi(in)”), phosphocholine, and phosphorylation potential index (“ß-ATP/ADP*Pi(in)”). For these metabolites and indices, the percent change from baseline to the week 12 end-of-treatment was significantly inversely correlated with baseline levels, such that participants with relatively lower baseline levels demonstrated increases, and subjects with relatively higher baseline levels demonstrated a re-balancing effect with levels decreased to the baseline population mean. This relationship was observed both on an integrated basis across the two trials and independently in both REPAIR-PD and REPAIR-MS. TEAEs were rated as mild and transient. No SAEs were reported and no participants experienced clinically significant laboratory abnormalities. The results of REPAIR-MS and REPAIR-PD robustly demonstrate target engagement in the brains of MS and PD patients and provide the first clinical evidence demonstrating the catalytic effects of CNM-Au8 on brain energetic metabolites.
VISIONARY-MS
The VISIONARY-MS clinical trial, launched in December 2018, was a double-blind, randomized, placebo-controlled Phase 2 trial, which evaluated the efficacy and safety of two doses of CNM-Au8 as a remyelinating and neuroprotective treatment in people who have stable RMS with chronic visual impairment. Enrolled participants had chronic optic neuropathy, defined as visual impairment with no episodes of acute optic neuritis within the six months prior to enrollment, and stable (non-active) disease, defined as no MS relapses within the three months prior to entry. Concomitant immunomodulatory MS DMTs were allowed. Participants were randomized to low-dose CNM-Au8 (15 mg/day), high-dose CNM-Au8 (30 mg/day), or matching placebo. The primary endpoint was improvement in low contrast letter acuity (“LCLA”) from baseline to week 48. Exploratory endpoints included OCT, multi-focal visual evoked potential (“mf-VEP”) amplitude & latency, full field-VEP amplitude & latency, MRI endpoints, visual function (high contrast) and QOL/Expanded Disability Status Scale (“EDSS”).
Contrast is the quantity of lightness or darkness contained by an object in comparison to its background. The smallest difference in contrast distinguished by the eye is known as the contrast threshold, usually reported as its reciprocal value, which is also known as contrast sensitivity (1/contrast threshold). Therefore, if a large amount of contrast is necessary for a patient to identify an object, they have poor contrast sensitivity and will have a low numerical value for this measurement. Contrast sensitivity can be analogized to a spectrum, in which black letters on a white background will be easier for any individual to discern than lower-contrast grey on white letters, regardless of whether or not visual impairment is present. The contrast threshold is the minimum amount of contrast necessary for an individual to discern an object from its background, and for people with MS the contrast threshold has been found to be higher than that of healthy individuals, even when visual acuity (measured at high contrast) is equal between the two groups. Contrast sensitivity is on a spectrum and may elicit more subtle changes in an individual’s contrast threshold that are missed by high contrast visual acuity. LCLA tests low-contrast vision at various spatial frequencies that may be particularly affected by damage to specific inter-neural connections in an individual’s complex visual pathway.
In the VISIONARY-MS trial plan, all participants were to have remained in the double-blind, placebo-controlled treatment period through week 48. However, as announced in February 2022, the trial was stopped prematurely due to COVID-19 pandemic operational challenges and some participants did not complete 48 weeks of treatment, but nearly all participants completed at least 24 weeks of treatment. Double-blind, placebo-controlled data was generated for most patients in the trial through week 48, improving the trial’s ability to assess the long-term effects of CNM-Au8 on clinical endpoints. The TGA, Health Canada, and the FDA all approved conduct of the trial. As a result of the trial ending prematurely, enrollment was limited to 73 out of 150 planned participants. Due to the limited enrollment, the threshold for significance was pre-specified at p=0.10 prior to database lock and submitted to the FDA as part of the statistical analysis plan. The primary analysis was conducted in a modified intent to treat (“mITT”) population, which censored invalid data. The mITT population excluded data from a single site (n=9) with LCLA testing issues and the timed 25-foot walk data from one subject with a change in mobility assist device at a different site. The ITT results, which included the non-valid data, were directionally consistent with the mITT results, although the ITT results were not significant.
We announced results from VISIONARY-MS in August 2022. The mITT population from baseline to week 48 demonstrated clinically-relevant, exposure-related mean standardized improvements in the primary endpoint, LCLA in the clinically affected eye (LS mean difference, 3.13; 95% CI: -0.08 to 6.33, p=0.056), as well the secondary endpoint of modified MS Functional Composite sub-scales (“mMSFC”), including mMSFC mean standardized change (LS mean difference, 0.28; 95% CI: 0.05 to 0.51, p=0.0197) and the mMSFC average rank score (LS mean difference, 12.94; 95% CI: 3.46 to 22.42, p=0.0083); and the secondary endpoint of time to first repeated clinical improvement to week 48 (45% versus 29%, log-rank p=0.3991). The integrated composite of the mMSFC sub-scales included Symbol Digit Modalities Test (“SDMT,” cognition), 9-Hole Peg Test (“9HPT,” upper extremity function), and Timed 25-foot Walk (“T25FWT,” gait) in the population as a whole. These analyses compared changes in mMSFC scores over the trial treatment period to the baseline values of trial participants with mild disease, as defined by Baseline EDSS scores of 1.5 or less. The baseline scores for these participants were chosen as a comparator because they demonstrated less neurological impairment than those of the overall trial population, providing a valid comparator group to evaluate change over time in the total trial population. Changes in the four MSFC sub-scales (LCLA, SDMT, 9HPT, and T25FW) were compared to baseline scores of this comparator group with mild disease from baseline to week 48. These comparisons were performed at each trial time-point (weeks 12, 24, 36, and 48). At each visit, the overall trial population (randomized 2:1 active CNM-Au8 to placebo) showed notable, exposure-related improvements in mean in overall MSFC scores and key MSFC sub-scales compared to the comparator group (mixed-effects model; p < 0.0001 versus baseline).
Additionally, consistent improvements favoring CNM-Au8 were observed across multiple paraclinical biomarkers, including mf-VEP amplitude and latency, optical coherence tomography (“OCT”), and MRI endpoints, including magnetization transfer ratio and diffusion tensor imaging metrics. Placebo treated patients, in contrast, generally worsened as expected across these measures during the 48-week period. These MRI endpoints provide evidence of brain neuronal structural integrity and demonstrate key metrics of axonal integrity and white matter integrity, which is associated with decreased cognitive functional decline in MS patients. Exploratory MRI endpoint results included all participants with advanced MRI data collection (n=68) and demonstrated (i) fractional anisotropy change within the whole brain (cerebrum) (0.0029, 95% CI: 0.0048 to 0.0054, p=0.0199); (ii) fractional anisotropy change within total cerebral white matter (week-48 LS mean difference, 0.0026, 95% CI: -0.0003 to 0.0055, p=0.0805); and (iii) fractional anisotropy change within total cerebral normal appearing white matter (week 48 LS mean difference, 0.0025, 95% CI: -0.00034 to 0.0054, p=0.0823). Exploratory mf-VEP endpoints in the VEP least effected eye, defined as the eye with the shortest latency at baseline, provided evidence of improved information transmission in the visual system (from the eye to the visual cortex) supported by statistically significant increases in amplitude. Exploratory mf-VEP results included all participants with recorded VEP data (n=64) and demonstrated (i) mf-VEP amplitude percent change in the least affected eye at baseline (week 48 LS mean difference, 9.7%, 95% CI: 3.1% to 16.3%, p=0.0047); (ii) mf-VEP amplitude percent change in the most affected eye at baseline (week 48 LS mean difference, 6.1%, 95% CI: -0.6% to 12.7%, p=0.0730); and (iii) mf-VEP amplitude percent change across both eyes (week 48 LS mean difference, 7.9%, 95% CI: 1.4% to 14.4%, p=0.0184). The increased amplitude signal suggests previously impaired neurons subsequently increase information transmission following CNM-Au8 treatment, supporting improved axonal integrity.
We believe these data support CNM-Au8’s potential to drive meaningful neurological improvements in MS patients. Further, we believe these observations are notable given the expected long-term decline in LCLA, SDMT, 9HPT, and T25FW amongst MS patients reported from data sets including from the MS Outcome Assessments Consortium (“MSOAC”) (Goldman et al. Neurology. 2019 Nov 19;93(21):e1921-e1931). MSOAC includes prospectively acquired RMS patient-level data from fourteen separate MS clinical trials including over 12,776 participants combined into a single database and followed for up to 24-months. When LCLA, SDMT, 9HPT, and T25FW were analyzed as a multidimensional measure rather than individually, progression on any one of these performance measures was more sensitive than the commonly used MS EDSS, and demonstrated long-term declines in RMS patients. The increasing mean improvements observed across the entire trial population (CNM-Au8 and placebo) may suggest a positive clinical effect for CNM-Au8 when contrasted with the anticipated decline reported in publications from the MSOAC data. Figure 9 below summarizes the primary and secondary efficacy outcomes for the VISIONARY-MS trial.
Figure 8. Results of VISIONARY-MS
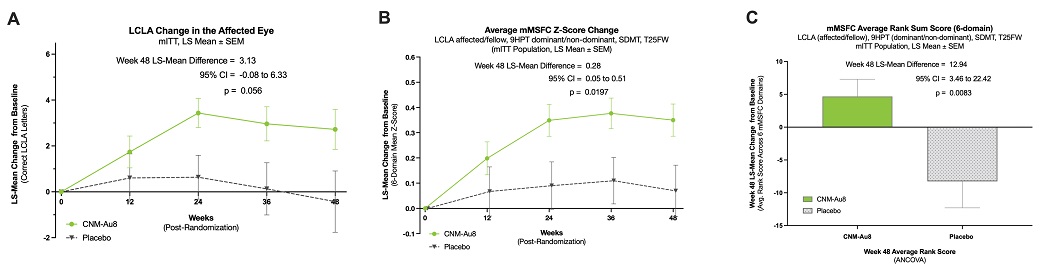
Safety data from VISIONARY-MS indicate that CNM-Au8 was well-tolerated with most adverse events characterized as transient and mild to moderate in severity. No SAEs related to the investigational product (e.g., placebo, CNM-Au8) were reported. The most frequently reported adverse events included upper respiratory infection, headache, back pain, and sore throat.
VISIONARY-MS—Long-Term Extension
VISIONARY-MS participants were treated with CNM-Au8 for up to 48 weeks in the double-blind period and could continue for up to an additional 96 weeks in the LTE. In January 2024, we announced results from the LTE for the mITT population. The LS mean difference (SE) at week 144 for LCLA change across both eyes versus the original randomization baseline of participants assigned to CNM-Au8 was: +8.70 letters (1.88), 95% CI: 5.0 to 12.4, p<0.0001; the LCLA LS squared mean difference (SE) versus the end of the double-blind period was: +4.0 letters (1.67), 95% CI: 0.72 to 7.30, p=0.017. Low contrast vision demonstrated sustained improvement by up to 38 letters across both eyes in individual participants, which represents multiple row gains on a greyed-out MS eye chart. The LS mean difference (SE) at week 144 for SDMT change versus the original randomization baseline of participants assigned to CNM-Au8 was: +8.03 (1.52), 95% CI: 5.01 to 11.0, p<0.0001; the SDMT LS mean difference (SE) versus the end of the double-blind period was: +3.11 (1.3), 95% CI: 0.55 to 5.68, p=0.018. Cognitive improvement, particularly working memory and information processing speed, was improved by up to 35 points in individual participants, where a three-point change in cognitive processing speed has been deemed notable in other MS studies. Additionally, improvements demonstrated during the 48-week double-blind period were maintained in the LTE for T25FWT and 9HPT. Placebo participants who transitioned to CNM-Au8 during the LTE showed significant improvements versus original baseline in LCLA and SDMT that were generally consistent with the increases observed in participants originally randomized to CNM-Au8.
Parkinson’s Disease
PD Market Opportunities
PD is a chronic, progressive neurodegenerative disorder affecting approximately 6.1 million patients worldwide as of 2016, and we estimate the market size will be approximately $6 billion by 2026. PD involves the progressive loss of dopaminergic neurons in the substantia nigra area of the midbrain. The degeneration of dopaminergic neurons leads to resting tremor, bradykinesia, limb rigidity, and gait and balance problems as well as increasingly recognized cognitive loss and behavioral changes due to more generalized neuronal loss. Both genetic and environmental factors are thought to contribute to the development of PD in addition to aging, which is the most significant risk factor for developing the disease. Approximately one in one hundred individuals over the age of 60 is affected by PD.
PD Current Therapies and Limitations
While there are a number of approved PD therapies, such as dopamine agonists, COMT and MAO-B inhibitors, and deep brain stimulation, these treatments are limited to symptomatic improvement. No treatment is currently available to prevent the destruction of dopaminergic neurons. The inexorable progression of loss of dopaminergic innervation leads to progressively worsening symptoms with “on” (dyskinesias) and “off” (rigidity) symptoms that become increasingly difficult to manage. In addition, long-term use of levodopa, a commonly-prescribed dopamine precursor used to treat Parkinsonian symptoms, often results in dyskinesia that in itself becomes disabling. Despite an enormous effort over the past several decades, no disease-modifying or neuroprotective therapeutic for PD is available. A therapeutic that alters or slows the clinical progression, and thus improves PD healthspan and lifespan, would address a very significant unmet need.
Neuronal energetic failure underlies PD, as evidenced by the observed impaired mitochondrial and lysosomal functioning, neuronal sensitivity to glutamate toxicity, accumulation of oxidative stress, autophagic failure in clearing misfolded proteins, and loss of synapse integrity associated with this disease. As such, improvement of cellular energetic efficiency, as is possible with CNM-Au8, represents an important and previously unaddressed therapeutic target for this disease.
Potential Advantages of CNM-Au8 for PD
We believe that CNM-Au8 has the potential to be a first-in-class disease modifying nanotherapeutic drug for PD. While current therapies for PD are designed to stimulate surviving dopaminergic neurons in order to elicit partial functional effects, none of them prevent the inexorable degeneration of dopaminergic neurons to change the course of disease progression. Our nonclinical studies demonstrate that CNM-Au8 is robustly neuroprotective of dopaminergic neurons across a variety of disease-relevant insults created using a variety of toxins and stressors. In addition, CNM-Au8 may have a tolerability profile superior to existing approved products and commonly used drugs for PD, such as levodopa/carbidopa which results in risk of dyskinesias after long-term use.
Summary of Nonclinical Pharmacology and General Neuroprotection Studies for PD
Excitotoxic injury, oxidative stress, and the accumulation of misfolded alpha-synuclein are hallmarks of the failing energetic pathways associated with PD. In order to determine whether CNM-Au8 could act as a neuroprotective agent for PD, we conducted a series of in vitro and in vivo studies designed to test efficacy of CNM-Au8 in protecting various neuronal cell types from a variety of PD relevant disease-related stressors.
The potential of CNM-Au8 to confer neuroprotection in PD disease-specific cellular models was first demonstrated in vitro. Primary rat dopaminergic cells were challenged with 1-methyl-4-phenyl-1,2,3,6-tatrahydropyridine, (“MPTP,” which is metabolized to its active form MPP+) or alternatively with 6-hydroxydopamine (“6-OHDA”), which are both toxins specific to dopaminergic neurons. Treatment of primary neuronal-glial cocultures with CNM-Au8 increased the numbers of surviving dopaminergic neurons in response to either toxin in a dose-dependent manner, as well as affected overall improvement in neuronal health by a variety of metrics, including preservation of neurite network, reduction in oxidative stress, increase in mitochondrial staining, and reduction in alpha-synuclein aggregates. The activity of CNM-Au8 was then tested in the standard 6-OHDA-unilateral lesion model of PD. Lesioned rats, and a sham control group, were orally administered vehicle or CNM-Au8 for 4-weeks (2-weeks post-lesion) or 6-weeks (one-day post lesion) following the establishment of a lesion in the striatum. Significant functional improvements due to CNM-Au8 treatment were demonstrated in both the behavioral apomorphine-induced rotation and cylinder paw placement tests. In addition, larger numbers of surviving dopaminergic neurons were detected in the striatum of CNM-Au8-treated lesioned animals compared to vehicle controls. These studies independently demonstrated that CNM-Au8 treatment has robust neuroprotective properties in preclinical models of PD.
Clinical Development of CNM-Au8 as a Disease-Modifying Drug for PD
REPAIR-PD
REPAIR-PD is a Phase 2, single-center, active-only, sequential group study to demonstrate central nervous system target engagement by examining the brain metabolic effects, safety, pharmacokinetics and pharmacodynamics of orally-delivered CNM-Au8 in patients who have been diagnosed with PD in vivo within three years of screening. These energetic metabolites are measured non-invasively and semi-quantitatively by utilizing 31P-MRS imaging with a 7T MRI scanner. A full volume head coil was used to collect whole brain spectral waveforms in ~600 voxels with a spatial resolution of 2 cm3 for the following metabolites: NAD pool (both NAD+ and NADH together), α-ATP, ß-ATP, γ-ATP, phosphocreatine, extracellular and cellular inorganic phosphate, uridine diphosphate glucose, phosphocholine, phosphoethanolamine, glycerophosphocholine, and glycerophosphoethanolamine. A partial volume head coil was used in the same patient cohort to measure occipito-parietal levels of individual NAD+ and NADH phosphorous metabolites to determine the ratio of NAD+/NADH.
REPAIR-PD was conducted at the University of Texas Southwestern, a center with specialized capabilities for conducting and analyzing 7T 31P-MRS imaging studies, and was conducted in conjunction with the REPAIR-MS trial, with a pre-specified integrated analyses of both trials performed. REPAIR-PD was approved for clinical conduct by the FDA and commenced in December 2019, and we subsequently enrolled 13 participants in the first dosing cohort with exposure to CNM-Au8 up to 21-weeks. A planned second cohort will not be enrolled due to institutional limitations.
Results were presented in September 2021. For the pre-specified integrated analyses of REPAIR-PD and REPAIR-MS, see “Multiple Sclerosis—REPAIR-MS” above. The independent results for REPAIR-PD demonstrated consistent trends toward improvement in the primary and secondary endpoints, although neither REPAIR-PD nor REPAIR-MS independently reached a level of statistical significance: the mean change in the brain NAD+/NADH ratio was 0.386 units (+6.8%) following 12-weeks of treatment with CNM-Au8 (p=0.1077, paired t-test), and the secondary endpoints of mean change from baseline in the NAD+ fraction of the total NAD pool increased (p=0.1336, paired t-test) and NADH fraction of the total NAD pool decreased (p=0.1336, paired t-test). The results of REPAIR-PD and REPAIR-MS robustly demonstrate target engagement in the brains of PD and MS patients and provide the first clinical evidence demonstrating the catalytic effects of CNM-Au8 on brain energetic metabolites.
RESCUE-PD
A second Phase 2 clinical trial is planned, subject to capital availability, to investigate the effects of CNM-Au8 on slowing or preventing disease progression in PD patients. The RESCUE-PD trial will follow patients with PD to determine the effects of CNM-Au8 on stabilizing disease activity as a neuroprotective therapeutic.
Additional CSN Therapeutics in the Pipeline
Two other drug candidates are at various IND-enabling stages of research. Utilizing our CSN therapeutic drug development platform, we have developed additional drug candidates based on the transition elements silver and zinc (CNM-ZnAg) for anti-viral/anti-bacterial and wound healing applications (CNM-AgZn17).
CNM-ZnAg, a Broad Spectrum Anti-Viral and Anti-Bacterial Agent
CNM-ZnAg was developed for use as an orally deliverable, broad-spectrum antiviral and antibacterial agent. It is formulated as an ionic solution of zinc (Zn+2) and silver (Ag+) with a limited presence (<1%) of silver Ag0 nanoparticles, all generated using the CSN platform in a manner that does not involve traditional inorganic synthesis methods utilized to generate zinc and silver compounds. The rationale for integrating a zinc-silver ionic solution was premised on the recognized historical activity of both Zn and Ag (as independent entities) for antimicrobial and antiviral disease treatment. Initial development studies both internally as well as externally from other labs revealed that when Zn2+ and Ag+ are administered together, they exhibit synergistic antiviral and antibacterial properties that are not observed when Zn2+ or Ag+, or Ag0 nanoparticles are administered singly.
In the human body, zinc is an essential structural component of <750 zinc finger transcription factors, and is a catalytic component of approximately 2,000 enzymes, encompassing all known enzyme classes. Most significantly, zinc is essential for the proper function of the immune system, and is specifically involved in multiple steps in the antiviral response. Zinc has demonstrated direct antiviral properties; in addition, zinc stimulates both innate and acquired antiviral responses. Thus, zinc-based treatments are hypothesized to support systemic immunity, while also acting to specifically inhibit viral replication, viral protein processing, and/or viral-infection-related symptoms. Silver has long been studied for its anti-infective activity. Silver’s microbial-treatment properties have been documented for centuries, and silver has been the most extensively studied metal for the purpose of fighting infections and preventing food spoilage. Prophylaxis of silver nitrate against gonococcal ophthalmia neonatorum with silver ions was considered the standard of care in many countries until the end of the twentieth century, prior to the advent of antibiotics. Independent research had demonstrated silver nanoparticles have been shown to be active against several types of viruses including human immunodeficiency virus, hepatitis B virus, herpes simplex virus, respiratory syncytial virus, and monkey pox virus. Silver nanoparticles and silver ions reduce viral infectivity when added concomitantly with the virus inocula, possibly by blocking interaction of the virus with the host cell.
A standard toxicology program based on ICH M3(R2) guidelines was completed for CNM-ZnAg. The toxicity of CNM-ZnAg was evaluated at high concentrations up to the maximum feasible dose administered via oral gavage up to four times daily for 28 days in rats and 7 days in canines. Across all studies, there were no deaths, no test-article-related clinical observations, and no effects on: body weight, food consumption, hematology endpoints, clinical pathology findings, blood coagulation times, urinalysis, or urine chemistry. Standard in vivo genotoxicity studies in rodents, including a 2-day COMET assay and a 28-day evaluation of micronucleated reticulocytes, revealed no test-article effects on genotoxicity.
A seven-day human tolerability study of CNM-ZnAg was previously conducted by an antecedent company to determine the safety and tolerability in 40 healthy human volunteers. No self-reported adverse events occurred and there were no safety findings associated with administration of the dietary supplement. Laboratory assessments indicated no significant changes from baseline in body weight, blood pressure, heart rate, liver enzymes (AST/ALT), blood glucose, and blood lipids (total cholesterol, LDL/HDL, triglycerides).
Clinical Development of CNM-ZnAg as a Therapeutic Treatment for COVID-19
Because of exigent worldwide need, we rapidly developed CNM-ZnAg as a candidate for treatment of COVID-19 based on the hypothesis that CNM-ZnAg may provide immune support benefits. On a limited basis, a dietary supplement version of CNM-ZnAg has been provided to support immune health. Preliminary uncontrolled observational case series with the dietary supplement yielded results suggesting oral administration of CNM-ZnAg to individuals with PCR-confirmed, COVID-19 infections may improve subject well-being and limit the duration of the disease. Given the potential for a clinical effect together with no identified safety signals from animal toxicology or initial human tolerability studies, we initiated a randomized, double-blind, placebo-controlled clinical trial to determine the efficacy and safety of CNM-ZnAg for symptomatic improvement of COVID-19. This clinical trial was conducted in Brazil and fully enrolled with 288 subjects. Substantially all participants were previously vaccinated. The primary endpoint was time to substantial alleviation of COVID-19 symptoms through 28 days, confirmed over a continuous period greater than or equal to 48 hours, in the mITT population (all participants with PCR documented SARS-CoV-2 infection). The trial evaluated two different doses of CNM-ZnAg, which were combined for analyses versus placebo. Trial results were announced in December 2022 and no clinical benefit was observed versus placebo. CNM-ZnAg was safe and well-tolerated, and no safety signals were identified. As a result, we have ceased further clinical development of CNM-ZnAg for treatment of COVID-19.
CNM-AgZn17 for Wound-Healing and Burn Treatment
CNM-AgZn17 consists of an ionic solution of silver and zinc in a polymer gel formulation for topical application to the skin. We have demonstrated in in vitro assays that CNM-AgZn17 has broad-based anti-viral and anti-bacterial activity against common and antibiotic resistant pathogens such as Methicillin-resistant Staphylococcus aureus. We have also shown enhanced wound healing benefits in animal models of diabetic wound healing and decreased scar formation following burns. We are presently completing a standard toxicology program in animals to demonstrate safety in order to advance to first-in-human dosing studies. We have progressed to GLP dermal toxicity studies for topical applications. Subject to regulatory filings of these toxicology findings and other results, and subject to capital availability, we anticipate filing an IND with the FDA and subsequently plan to initiate a standard Phase 1 dermal first-in-human safety study with CNM-AgZn17 with single-ascending dose and multiple-ascending dose cohorts. The goal of this study will be to demonstrate safety sufficient to advance to Phase 2 clinical programs with CNM-AgZn17. Given the multiple preclinical benefits demonstrated to date with CNM-AgZn17, we envision a clinical program focused on healing burn and/or surgical wounds.
Research and Development
Overview
We are deeply invested in our research and development program. Our research and development activities are essential to attaining and sustaining the position as a recognized global leader in the development of CSN therapeutics. Our research and development plan is to continue the innovation of novel catalytically-active nanocrystals and ionic suspensions of metallic transition elements with recognized medicinal value and underexplored, or as yet undiscovered, physicochemical and catalytic properties. We developed all the technologies that are critical to our research and development processes in-house and guard those technologies with appropriate intellectual property protections. We conduct our research activities through both an internal research and development team and by engaging external clinical research collaborations to support our research and development activities.
Internal Research and Development
Our internal research and development activities are executed by a group of experienced in-house research scientists, materials scientists, engineers, molecular biologists, medical doctors, clinical trial operational specialists, and a management team with deep expertise in the biopharmaceutical industry. Our internal research and development team has a full range of capabilities ranging from drug discovery to preclinical development to the design and implementation of clinical trials. We believe our in-house research and development team is experienced, qualified, and will enable us to achieve our long-term goal of developing and commercializing innovative CSN therapeutics for patients worldwide. Our in-house research and development team operates functionally through four sub-teams: (1) research engineering team, (2) biological science discovery team, (3) nonclinical development team, and (4) clinical development team, which work collaboratively to ensure the success of our research and development efforts.
Research Engineering. Our research engineering team is responsible for the development and optimization of new CSN therapeutic candidates along with developing the technical processes and infrastructure to ensure reproducible chemistry, manufacturing, and controls (“CMC”) batch production of our CSN therapeutic candidates. Members of our research engineering team have PhDs and/or master’s degrees in chemistry, material science and engineering, electrical engineering, and solid-state physics. Our research engineering team leader has a degree in electrical engineering and has been instrumental in the design of our electro-crystal-chemistry platform including the various continuous flow apparatuses (“troughs”) used to produce our CSN therapeutics.
Biological Science Discovery. Our biological science discovery team is responsible for the initial characterization of CSN therapeutic candidates, conducting biological assays, assessing the activity and toxicity of drug candidates through in vitro and in vivo assays, and assessing CSN therapeutic candidates once the initial development has been completed by our research engineering team. Our biological science discovery team collaborates with our research engineering team to refine our CSN therapeutic candidate selection characteristics to optimize their biological effects. Our biological science discover team is led by an experienced research scientist who is a medical doctor and has a PhD in molecular science.
Nonclinical Development. Our nonclinical development team is responsible for developing a complete and sufficient dataset of nonclinical animal pharmacology, toxicology, and safety studies to support regulatory filings with human research ethics committees (“HRECs”) and government regulatory authorities, in order to obtain approval for use in human studies. Our nonclinical development team collaborates with our biological science discovery and clinical development teams to translate our findings into animals and prepare for eventual studies in patients. Our nonclinical development team also leads our external collaboration research activities with universities and academic experts. Our nonclinical development team is led by a research scientist with a PhD in Developmental Biology from Stanford University and a Master of Science degree in Genetics from the University of Cambridge where she was a Marshall Scholar. She is also an adjunct faculty member of the University of Utah School of Medicine.
Clinical Development. Our clinical development team designs, implements, and oversees the operational conduct of our clinical trials after our CSN therapeutic candidates have demonstrated sufficient safety and toxicology results to advance to human studies. Our clinical development team is led by our Head of Medical, who is a board-certified neurologist and is also a professor of neurology in the Department of Neurology at the University of Texas Southwestern Medical Center, where he also serves as a director for several neuroscience-related initiatives and research centers.
External Research and Development
In line with industry practice, we also outsource certain research and development to key academic partners, nonclinical research organizations, and third-party CROs. We have collaborated with experts at key academic universities with myelination and neuroprotection expertise who have conducted animal experiments to demonstrate the effects of CNM-Au8 treatment on remyelination and neuroprotection in animals and in cell-based in vitro assays. To support our research efforts, we have partnered with academic experts at Johns Hopkins University for ALS, the University of Cambridge for myelination-related experiments, Northwestern University for myelination-related experiments, George Washington University for myelination-related experiments, and the University of Edinburgh for myelination-related research. In general, we outsource the majority of toxicology, pharmacology, and toxicokinetic studies to expert nonclinical CROs.
To provide maximum flexibility and efficiency to operations, we engage industry-leading CROs to manage, conduct and support our clinical trials and to supplement our internal research and development capabilities. We apply a rigorous process to selecting CROs to conduct our research studies; selection is based on the quality, reputation, and research experience in the field of central nervous system disorders. In addition to the scope, depth, quality of service, and product offerings of CROs, for clinical trial management, we place emphasis on the ability of CROs to facilitate optimal site selection, to recruit patients in a timely manner, and to conduct complex clinical trials efficiently. Our CROs are widely recognized within their functional areas of research.
We enter into separate agreements with CROs and our external partners for each clinical trial or nonclinical research project. All CROs and other external research collaborators were all independent third parties. Principal terms of the service agreements with our key CROs and external partners are summarized as follows:
| ● |
Services. The CRO, nonclinical research organization, or academic site implements and manages the study in accordance with the protocol designed by us as specified in the service agreement. |
| ● |
Term. The CRO, nonclinical research organization, or academic site is required to support the clinical trial or nonclinical studies within the prescribed time limit until the end of the clinical trial. |
| ● |
Payments. We are required to make payments to our partners in accordance with the payment schedule agreed by the parties. |
| ● |
Intellectual property rights. We own intellectual property rights arising from the research activities related to our background intellectual property. |
| ● |
Risk allocation. Each party indemnifies the other party for losses caused by its fault or gross negligence. We indemnify the CRO and external partners for theoretical risks related to CNM-Au8. |
We monitor and evaluate our CROs and external research partners with various activities including site visits, ongoing project team reviews, and/or assessments by third-party assessors. We strive to achieve clinical trial excellence by maintaining strong quality control measures. We perform core functions such as clinical development strategy formulation and protocol design in-house, and exercise control and oversight over key functions of clinical trial management. We conduct regular site visits to oversee site initiation, patient recruitment, and data quality monitoring. We also engage third-party consultants to perform clinical trial audits. Data quality is further assessed by in-house data review, including medical review, document review, and monitoring report review. We will not work with a vendor who does not have processes established surrounding data privacy and safeguards to ensure compliance through the clinical trial. We have maintained a stable relationship with our CROs and other external research partners.
Clinical Trial Management
To support our clinical trials, our internal clinical development team designs, implements, collects and analyzes data for our clinical trials. When additional services are required to support a clinical trial, we conduct a feasibility and qualification assessment for potential vendors and CROs. These vendors are vetted through review of their current operational structure and established procedures, knowledge and experience about the study, indication, or population, and past feedback from participating clinical sites. Our internal clinical development team supervises CROs on key clinical activities, such as patient eligibility review, medical data review, and SAE review, to ensure that the performance of CROs complies with our protocols and applicable laws and to protect the integrity and authenticity of the data from our clinical trials. Our internal clinical development team holds meetings with CROs to evaluate the CRO’s performance by following up on clinical progress and resolving potential issues and risks.
Financial Grants
We have been awarded grants from various organizations, including the National Multiple Sclerosis Society, FightMND, a not-for-profit registered charity in Australia, the Michael J. Fox Foundation, and the National Institute of Neurological Disorders and Stroke, a division of the National Institute of Health. The grants include the following terms:
| ● |
National Multiple Sclerosis Society. |
| ○ |
We received a grant of $0.4 million in September 2019 for biomarker analyses related to our VISIONARY-MS clinical trial. Funding was based upon the achievement of certain analytical milestones. In the event we commercialize CNM-Au8 for the treatment of MS, we would be required to repay between 50% and 450% of grant funds based upon certain sales milestones. We will own all intellectual property rights arising from grant-related activities. |
| ○ |
We received a grant of $0.7 million in May 2023 to fund Cohort 2 of our REPAIR-MS clinical trial. Funding is based upon the achievement of certain clinical milestones. In the event we commercialize CNM-Au8 for the treatment of MS, we would be required to repay between 50% and 450% of grant funds based upon certain sales milestones. We will own all intellectual property rights arising from grant-related activities. |
| ● |
FightMND. We received a grant of AUD1.4 million in August 2019 for our RESCUE-ALS clinical trial. Funding was based upon the achievement of certain patient enrollment targets. In the event that certain intellectual property is created during RESCUE-ALS and subsequently commercialized in Australia, we would be required to repay, at the sole discretion of FightMND, 10% of future net sales proceeds up to 500% of the original grant amount. We will own all intellectual property rights from grant related activities. |
| ● |
The Michael J. Fox Foundation. We received a grant of $0.5 million in January 2021 for preclinical iPSC and animal model studies to assess CNM-Au8 for the treatment of PD. Funding was based upon the achievement of certain analytical milestones. We will own all intellectual property rights from grant related activities. |
| ● |
National Institute of Neurological Disorders and Stroke. A grant of $45.1 million was awarded to us, in collaboration with Columbia University and Synapticure, in October 2023 to support an EAP for CNM-Au8 treatment of ALS. The grant was awarded under the Accelerating Access to Critical Therapies for ALS Act, which was signed into law in December 2021. We are currently working to sign a sub-award agreement with Columbia University, the prime awardee, prior to the commencement of the EAP. |
We also received indirect financial support for the HEALEY ALS Platform Trial, administered by Massachusetts General Hospital, which conducted a platform trial of CNM-Au8 alongside other drugs at significantly lower costs than we would otherwise incur if we were to conduct a comparably designed study at reasonable market rates.
Manufacturing
We manufacture CSN therapeutics at our production facility in North East, Maryland (the “North East Facility”), based on novel manufacturing processes and devices that were entirely invented by us. The North East Facility is compliant with rigorous international Good Manufacturing Processes (“GMP”), and we operate an ISO8-level clean room that contains the specialized electro-crystal-chemistry devices, or continuous flow trough apparatuses, that we invented and patented to produce our CSN therapeutics from highly pure raw materials. We produce a gold nanocrystal suspension, the active pharmaceutical ingredient (“API”) for CNM-Au8, on an ongoing basis. We believe our current production capabilities are sufficient to meet our needs for both research and development and to supply our ongoing and planned clinical trials and EAPs, and we believe our processes can be scaled to achieve early commercially viable quantities.
Additionally, we currently lease a 74,210 square foot production facility in Elkton, Maryland (the “Elkton Facility”), a few miles from our North East Facility. We plan to redevelop the Elkton Facility to support our unique manufacturing needs and to enable us to materially increase our manufacturing capacity in the event of commercialization. We also expanded our North East Facility from approximately 21,000 square feet to approximately 32,600 square feet to further increase our manufacturing capacity. We believe our technical expertise and capabilities are sufficient to expand capacity to support contemplated growth and anticipated commercialization. We have also developed a phased plan to significantly scale our production processes and capabilities as demand increases to supply pre-commercial and commercial marketing needs. We believe our current production environment has established us as the leading world-class manufacturer of CSN therapeutics, and following the completion of our planned expansion, our facilities, equipment, and processes will comply with international practices and support our long-term strategic plans, taking into consideration quality, costs, manageability, expandability, and controls.
We have invested considerable time and substantial resources to fine-tune our production and delivery processes to enable consistent, reliable, and affordable production of our primary drug candidates; and to perfect our handling and storage systems in order to maintain stability and efficacy of our nanocrystal suspensions. In general, the manufacturing process for CSN therapeutics involves the following steps:
| ● |
Sufficient quantities of processing enhancers (e.g., sodium bicarbonate, others) are dissolved in highly purified water. The resulting mixture is referred to as “process water.” |
| ● |
Process water is transferred to the conditioning portion of the trough apparatus at a constant nominal rate where it is exposed to an atmospheric plasma in each trough apparatus, creating “conditioned water.” |
| ● |
Conditioned water flows into the electrochemical crystal growth portion of the trough apparatus, at a constant rate, where it is exposed to a series of wire electrode pairs. The flow of conditioned water is controlled, and the electrodes are continuously monitored and controlled by computerized, automated controllers. |
| ● |
The electrodes are slowly advanced at a nominal rate to ensure that conditioned water is exposed to the same electrochemical processing conditions to ensure batch-to-batch reproducibility, thus maintaining consistent size and shape of nanocrystals in each nanocrystal suspension. |
| ● |
In-process API containing elemental nanocrystals is continuously produced and collected into large containers. |
| ● |
The nominal concentration of active drug ingredients is achieved by treating in-process API with a proprietary concentration procedure. |
| ● |
The concentrated nanocrystal suspension is validated to ensure it adheres to physiochemical release specifications. |
| ● |
The concentrated nanocrystal suspension is subsequently filtered to remove any microbiological contaminants and volumetrically filled into single unit containers. The final product is assayed to ensure it meets release specifications. |
License Arrangements
In August 2018, we entered into a license agreement (the “License Agreement”) and exclusive supply agreement (the “Supply Agreement”) in conjunction with 4Life’s investment in the Company.
| ● |
License Agreement. We granted 4Life an exclusive and royalty-bearing license to develop, manufacture, and sell certain non-pharmaceutical, low-concentration dietary supplement products produced by our electro-crystal-chemistry platform. 4Life pays royalties to us equal to 3% of net sales of licensed products. 4Life is subject to an annual minimum sales requirement; if unmet, 4Life may pay us an additional fee to maintain exclusivity or have the license converted to non-exclusive. The initial term of the exclusive license is five years from the commencement of product sales under the License Agreement, which occurred in July 2020, with an option to renew for additional five-year periods upon mutual agreement. |
| ● |
Supply Agreement. We granted 4Life an exclusive right to purchase certain non-pharmaceutical, low-concentration dietary supplement products produced by our electro-crystal-chemistry platform. 4Life’s price to purchase products from us under the Supply Agreement is equal to our fully encumbered manufacturing costs plus 20%. Upon the occurrence of certain events, 4Life can achieve the right to exclusively manufacture products under the Supply Agreement. The initial term of the Supply Agreement is five years from the minimum sales commencement date, which occurred in April 2021, with an option to renew for additional five-year periods upon mutual agreement. |
We currently provide an aqueous zinc-silver ion dietary (mineral) supplement to 4Life on a non-exclusive basis, which is sold by 4Life under the tradename Zinc Factor™; and an aqueous gold dietary (mineral) supplement of very low-concentration gold nanoparticles on an exclusive basis, which is sold by 4Life under the tradename Gold Factor™ and is subject to royalties.
To date, we have not licensed our electro-crystal-chemistry platform, CSN therapeutics, or drug candidates to any other parties.
Sources and Availability of Raw Materials
Certain critical raw materials are available from a limited number of suppliers in the market. See Item 1A—Risk Factors “—Our business depends on the use of raw materials, and a decrease in the supply or an increase in the cost of these raw materials or any quality issues in such raw materials could materially and adversely affect our business, financial condition, results of operations, and prospects” for further information.
Competition
While the treatment for central nervous system diseases is quite competitive and subject to frequent changes, there are currently no existing FDA-approved therapies that have mechanisms supporting remyelination and neuroprotection in patients. CNM-Au8’s core effects of remyelination and neuroprotection provide us a globally unique first-mover-advantage for the treatment of central nervous system diseases. Together with our expanded intellectual property portfolio, we believe that it would be challenging for any potential competitors entering into the market of remyelination and neuroprotection focused therapeutics to replicate our efforts without violating our intellectual property protections.
Intellectual Property
We are the sole inventors of our manufacturing processes, devices, and drugs. These inventions are protected through extensive global patents, institutional expertise and experience, and specialized technical knowledge, which enables us to maintain our leading position in the development of CSN® therapeutics for high-medical need diseases. As of December 31, 2023, we have over 150 issued patents worldwide and approximately 20 patents pending worldwide. We have world-wide rights to protect and thus commercialize our CSN therapeutics and believe that our issued, and pending patents, provide sufficient protection to secure the future commercial potential of our CSN therapeutics. To date, we have not been involved in any proceedings in respect of, and we have not received notice of any claims of infringement of, any intellectual property rights that may be threatened or pending, in which we may be a claimant or a respondent.
We have filed and obtained patents in the United States (U.S.); Australia (AU); Brazil (BR); Canada (CA); China (CN); European Patent Office (EP), including Belgium (BE), Switzerland (CH), Germany (DE), Denmark (DK), Finland (FI), France (FR), Great Britain (GB), Iceland (IS), Ireland (IE), Italy (IT), Hungary (HU), Netherlands (NL), Norway (NO), Poland (PL), Portugal (PT), Spain (ES), Sweden (SE), Slovenia (SI), and Turkey (TR); Egypt (EG); India (IN); Indonesia (ID); Israel (IL); Japan (JP); Korea (KR); Mexico (MX); New Zealand (NZ); Philippines (PH); Russia (RU); Seychelles (SC), Singapore (SG); and the United Arab Emirates (AE); with multiple fundamental patent families protecting our CSN therapeutics. The following table lists the material granted patent families in connection with our CSN therapeutics.
| Description |
|
Jurisdiction |
|
Application Date (U.S.) |
|
Grant Date (U.S.) |
| Continuous methods for treating liquids and manufacturing certain constituents (e.g., nanoparticles) in liquids, apparatuses and nanoparticles and nanoparticle/liquid solution(s) resulting therefrom (these patents relate to CNM-Au8 and ZnAg) |
|
Issued: U.S. (4), AU (3), CA (2), CN, ID, IL, IN, JP (2), KR, MX, PH; BE, DK, ES, FI, FR, DE, HU, IE, IT, NL, NO, PL, PT, SE, SI, SC, CH, TR, GB
Pending: U.S., EP |
|
July 11, 2007 |
|
December 31, 2013 August 29, 2017 October 9, 2018 May 11, 2021
Expiration dates for these patents will occur in 2028 in the applicable foreign jurisdictions and in 2030 in the U.S.* |
| Continuous methods for treating liquids and manufacturing certain constituents (e.g., nanoparticles) in liquids, apparatuses and nanoparticles and nanoparticle/ liquid solution(s) therefrom |
Issued: U.S. (3)
Pending: U.S. |
January 14, 2009 |
September 24, 2013 July 12, 2016 October 15, 2019
Expiration dates for these patents will occur in 2030 in the U.S. |
|||
| Continuous, semi-continuous and batch methods for treating liquids and manufacturing certain constituents (e.g., nanoparticles) in liquids, apparatuses and nanoparticles and nanoparticle/liquid solution(s) and colloids resulting therefrom (these patents relate to CNM-Au8 and ZnAg) |
Issued: U.S. (3), AU, CA, CN, IN, IS, JP, KR; CH, DE, DK, FI, FR, IE, NL, NO, SE, GB | January 15, 2009 | June 30, 2015 July 31, 2018 May 18, 2021
Expiration dates for these patents will occur in 2030 in the U.S. and the applicable foreign jurisdictions* |
| Description | Jurisdiction | Application Date (U.S.) | Grant Date (U.S.) | |||
| Novel gold-based nanocrystals for medical treatments and electrochemical manufacturing processes therefor (these patents relate to CNM-Au8) | Issued: U.S. (3), AE, AU (5), BR, CA, CN, ID, IN, IL, JP (4), KR (3), MX (2), PH, RU, SG (2); CH, DE, DK, ES, FI, FR, GB, IE, IT, NL, NO, SE
Pending: AU, MX, PH, SG, U.S. (2) |
July 8, 2009 | March 28, 2017 October 22, 2019 April 20, 2021
Expiration dates for these patents will occur in 2030 in the U.S. and the applicable foreign jurisdictions* |
|||
| Novel gold-platinum based bi-metallic nanocrystal suspensions, electrochemical manufacturing processes therefor and uses for the same (these patents do not relate to any specifically named product candidates herein) | Issued: U.S., AE, AU, CA, CN, ID, IL, IN, JP, KR (2), MX, NZ, PH, RU, SG; CH, DE, DK, ES, FI, FR, GB, IE, IT, NL, NO, SE.
Pending: BR, U.S. |
March 30, 2011 | July 12, 2016
Expiration dates for these patents will occur in 2030 in the U.S. and in 2032 in the applicable foreign jurisdictions* |
|||
| Methods and treatment for certain demyelination and dysmyelination-based disorders and/or promoting remyelination (these patents relate to CNM-Au8) | Issued: AU, BR, CA, ID, IL, JP, KR, MX, NZ (2), PH, RU, SG (2); BE, DK, FI, FR, DE, HU, IE, IT, NL, NO, PT, SE, SI, CH, TR, GB
Pending: IN, JP |
NA | NA
Expiration dates for these patents will occur in 2033 in the U.S. and the applicable foreign jurisdictions* |
* Expiration dates do not include possible patent extensions for certain countries.
In addition to filings for U.S. and foreign patents, we will continue to protect and maintain our proprietary position by the use of trademarks, trade secrets, copyright protection, and continued technological innovation. For example, years of intensive research and development were invested in fine-tuning our production and delivery processes to the point where we expect to be able to consistently, reliably, and affordably produce our drug candidates, including our lead asset, CNM-Au8, to meet large scale needs. We believe that any attempts to reverse engineer or otherwise replicate our discoveries would be extraordinarily challenging for potential competitors without violating our intellectual property protections. We are also focused on building a robust and relevant trade secret portfolio, primarily related to the liquid handling and processing of our products from start to finish. We continue to explore additional ways to expand our trade secret portfolio in various aspects of the design, production, control and manufacture of our products.
Government Regulation
The FDA and other regulatory authorities at federal, state, and local levels, as well as in foreign countries, extensively regulate, among other things, the research, development, testing, manufacture, quality control, import, export, safety, effectiveness, labeling, packaging, storage, distribution, record keeping, approval, advertising, promotion, marketing, post-approval monitoring, and post-approval reporting of drugs such as those we are developing. We, along with third-party contractors, are required to comply with the various preclinical, clinical, and commercial approval requirements of the governing regulatory agencies of the countries in which we wish to conduct studies or seek approval or licensure of CNM-Au8 or any future drug candidate.
FDA Drug Approval Process
In the U.S., the FDA regulates drugs under the Federal Food, Drug and Cosmetic Act and implementing regulations and guidance. The process required by the FDA before drug candidates may be marketed in the U.S. generally involves the following:
| ● |
completion of preclinical laboratory tests and animal studies performed in accordance with the FDA’s current Good Laboratory Practices regulations; |
| ● |
submission to the FDA of an IND application, which must become effective before clinical trials may begin and must be updated annually or when significant changes are made; |
| ● |
approval by an independent review board whose role is to review the research before the trial commences and continuously throughout the trial to assure the protection of the rights and welfare of the human subjects. These boards are often called “institutional review boards” (“IRBs”); |
| ● |
performance of adequate and well-controlled human clinical trials to establish the safety and efficacy of the proposed drug candidate for its intended purpose; |
| ● |
preparation of and submission to the FDA of an NDA after completion of all pivotal clinical trials that includes substantial evidence of safety and efficacy from results of nonclinical testing and clinical trials; |
| ● |
a determination by the FDA within 60 days of its receipt of an NDA to file the application for review; |
| ● |
satisfactory completion of an FDA pre-approval inspection of the manufacturing facility or facilities at which the proposed product is produced to assess compliance with GMP and to assure that the facilities, methods, and controls are adequate to preserve the drug candidate’s continued safety, purity and potency, and of selected clinical investigation sites to assess compliance with Good Clinical Practices (“GCP”); |
| ● |
satisfactory completion of an FDA Advisory Committee review, if applicable; and |
| ● |
FDA review and approval of the NDA to permit commercial marketing of the product for particular indications for use in the U.S. |
Preclinical and Clinical Development
Prior to beginning the first clinical trial with a drug candidate in the U.S., we must submit an IND application to the FDA. An IND application is a request for authorization from the FDA to administer an investigational new drug product to humans. The central focus of an IND submission is the general investigational plan and the protocol(s) for clinical trials. The IND also includes results of animal and in vitro studies assessing the toxicology, pharmacokinetics, pharmacology, and pharmacodynamic characteristics of the drug candidate; CMC information; and any available human data or literature to support the use of the investigational product. An IND must become effective before human clinical trials may begin. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30-day time period, raises safety concerns or other questions about the proposed clinical trial. In such a case, the IND may be placed on clinical hold until the IND sponsor and the FDA resolve the outstanding concerns or questions. Submission of an IND therefore may or may not result in FDA authorization to begin a clinical trial.
Clinical trials involve the administration of the investigational product to human subjects under the supervision of qualified investigators in accordance with GCP and regulations governing the protection of human research subjects, including the requirement that all research subjects provide voluntary informed consent for their participation in any clinical trial. Clinical trials are conducted under clinical trial protocols detailing, among other things, the objectives of the trial, the parameters to be used in monitoring safety, and the effectiveness criteria to be evaluated. A separate submission to the existing IND must be made for each successive clinical trial conducted during product development and for any subsequent protocol amendments. For new indications, a separate new IND may be required. An IRB must review and approve the plan for any clinical trial and its informed consent form before the clinical trial begins and must monitor the trial until completed. Often each institution or clinical site has its own IRB. The IRB is responsible for ensuring that human subjects’ rights and privacy are maintained. Regulatory authorities, the IRB, or the sponsor may suspend a clinical trial at any time on various grounds, including a finding that the subjects are being exposed to an unacceptable health risk or that the trial is unlikely to meet its stated objectives. Some studies also include oversight by a DSMB, an independent group of qualified experts organized by the clinical trial sponsor, which provides authorization for whether or not a clinical trial may move forward at designated check points based on access to certain data from the trial. The DSMB may halt the clinical trial if it determines that there is an unacceptable safety risk for subjects or other grounds, such as no demonstration of efficacy. Ongoing clinical trials and clinical trial results are required to be reported to public registries. For purposes of NDA approval, human clinical trials are typically conducted in three sequential phases (which may overlap or be combined):
| ● |
Phase 1. The investigational product is initially introduced into a small number of healthy human subjects or patients with the target disease or condition. These studies are generally designed to test the safety, dosage tolerance, absorption, metabolism, distribution, and elimination of the investigational product in humans, the side effects associated with increasing doses, and, if possible, to gain early evidence on effectiveness. |
| ● |
Phase 2. The investigational product is administered to a larger, but still limited patient population with a specified disease or condition to evaluate the preliminary efficacy (usually based on a biomarker of disease), optimal dosages, and to identify possible adverse side effects and safety risks. Multiple Phase 2 clinical trials may be conducted to obtain information prior to beginning larger, confirmatory Phase 3 clinical trials. |
| ● |
Phase 3. The investigational product is administered to an expanded patient population to provide statistically significant evidence of relevant clinical efficacy and to further test for safety, and potentially further evaluate different dosages, generally at multiple geographically dispersed clinical trial sites. These clinical trials are intended to establish the overall risk/benefit ratio of the investigational product and to provide an adequate basis for product approval by health authorities. |
In some cases, the FDA may require, or companies may voluntarily pursue, additional clinical trials after a product is approved to gain more information about the product. These studies, termed Phase 4 studies, may be implemented as a condition of approval of the NDA. Concurrent with clinical trials, companies may complete additional animal studies and develop additional information about the biological characteristics of the drug candidate, and must finalize a process for manufacturing the product in commercial quantities in accordance with current GMP requirements. The manufacturing process must be capable of consistently producing quality batches of the drug candidate and, among other things, must develop methods for testing the identity, strength, quality and purity of the final product. Additionally, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the drug candidate does not undergo unacceptable deterioration over its shelf life.
Drug companies such as us are subject to legal requirements restricting, or imposing penalties for, the employment or use of individuals who have been debarred or excluded under various laws, including the provisions of 21 U.S.C. Section 335a, 335b, or 335c, 42 U.S.C. Section 1320a-7, in connection with making materially false or fraudulent statements to FDA, the offering or making of any prohibited payment, gratuity or other thing of value to personnel of the FDA or any other governmental entity, or other acts, statements, or omissions subject to FDA’s policy titled “Fraud, Untrue Statements of Material Facts, Bribery, and Illegal Gratuities” set forth in 56 Fed. Reg. 46191 (September 10, 1991), Employment of such individuals, or the occurrence of such violations in the development and regulatory application process may prevent or delay any approval of an NDA.
NDA Submission, Review and Approval
Assuming successful completion of all required testing in accordance with all applicable regulatory requirements, the results of nonclinical studies and clinical trials are submitted to the FDA as part of an NDA requesting approval to market the product for one or more indications. The NDA must include all relevant data available from pertinent preclinical studies and clinical trials, including negative or ambiguous results as well as positive findings, together with detailed information relating to the product’s CMC, and proposed labeling, among other things. The submission of an NDA requires payment of a substantial application user fee to FDA (unless a waiver or exemption applies).
Once an NDA has been submitted, the FDA’s goal is to review standard applications within ten months after it accepts the application for filing (a 60-day process), or, if the application qualifies for priority review, six months after the FDA accepts the application for filing. In both standard and priority reviews, the review process can be significantly extended by FDA requests for additional information or clarification. The FDA reviews an NDA to determine, among other things, whether a product is safe and effective and the facility in which it is manufactured, processed, packaged, or held meets standards designed to assure the product’s continued safety and efficacy. The FDA may convene an advisory committee to provide clinical insight on application review questions. Before approving an NDA, the FDA will typically inspect the facility or facilities where the product is manufactured. The FDA will not approve an application unless it determines that the manufacturing processes and facilities are in compliance with GMP requirements and adequate to assure consistent production of the product within required specifications. Additionally, before approving an NDA, the FDA will typically inspect one or more clinical sites to assure compliance with GCPs. If the FDA determines that the application, manufacturing processes, or manufacturing facilities are not acceptable, it will outline the deficiencies in the submission and often will request additional testing or information. Notwithstanding the submission of any requested additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval.
After the FDA evaluates an NDA and conducts inspections of manufacturing facilities where the investigational product and/or its drug substance will be produced, the FDA may issue an approval letter or a Complete Response Letter. An approval letter authorizes commercial marketing of the product with specific prescribing information for specific indications. A Complete Response Letter will describe all the deficiencies that the FDA has identified in the NDA, except that, where the FDA determines that the data supporting the application are inadequate to support approval, the FDA may issue the Complete Response Letter without first conducting required inspections, testing submitted product lots, and/or reviewing proposed labeling. In issuing the Complete Response Letter, the FDA may recommend actions that the applicant might undertake to resolve any findings and place the NDA in condition for approval, including requests for additional information or clarification. The FDA may delay or refuse approval of an NDA if applicable regulatory criteria are not satisfied, require additional testing or information and/or require post-market testing and surveillance to monitor safety or efficacy of a product.
If regulatory approval of a product is granted, such approval will be granted for particular indications and may entail limitations on the indicated uses for which such product may be marketed. For example, the FDA may approve the NDA with a Risk Evaluation and Mitigation Strategy (“REMS”), to ensure the benefits of the product outweigh its risks. A REMS is a safety strategy to manage a known or potential serious risk associated with a product and to enable patients to have continued access to such medicines by managing their safe use, and could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. The FDA also may condition approval on, among other things, changes to proposed labeling or the development of adequate controls and specifications. Once approved, the FDA may withdraw the product approval if compliance with pre- and post-market requirements is not maintained or if problems occur after the product reaches the marketplace. The FDA may require one or more Phase 4 post-market studies and surveillance to further assess and monitor the product’s safety and effectiveness after commercialization, and may limit further marketing of the product based on the results of these post-market studies.
Expedited Development and Review Programs
A marketing application for a drug candidate submitted to the FDA for approval may be eligible for FDA programs intended to expedite the FDA review and approval process, such as priority review, fast track designation, breakthrough therapy, and accelerated approval.
A product is eligible for priority review if it has the potential to provide safe and effective therapy where no satisfactory alternative therapy exists or to provide a significant improvement in the treatment, diagnosis or prevention of a serious disease or condition compared to marketed products. For products containing new molecular entities, priority review designation means the FDA’s goal is to take action on the marketing application within six months of the 60-day filing date (compared with ten months under standard review).
To be eligible for a fast track designation, the FDA must determine, based on the request of a sponsor, that a product is intended to treat a serious or life-threatening disease or condition and demonstrates the potential to address an unmet medical need by providing a therapy where none exists or a therapy that may be potentially superior to existing therapy based on efficacy or safety factors. Fast track designation provides opportunities for more-frequent interactions with the FDA review team to expedite development and review of the product. The FDA may also review sections of the NDA for a fast track product on a rolling basis before the complete application is submitted, if the sponsor and FDA agree on a schedule for the submission of the application sections, and the sponsor pays any required user fees upon submission of the first section of the NDA. The review clock does not begin until the final section of the NDA is submitted.
In addition, under the provisions of the FDA Safety and Innovation Act enacted in July 2012, a sponsor can request designation of a drug candidate as a “breakthrough therapy.” A breakthrough therapy is defined as a drug that is intended, alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or condition, and preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. Drugs designated as breakthrough therapies are also eligible for accelerated approval. The FDA must take certain actions, such as holding timely meetings and providing advice, intended to expedite the development and review of an application for approval of a breakthrough therapy.
Additionally, products studied for their safety and effectiveness in treating serious or life-threatening diseases or conditions may receive accelerated approval upon a determination that the product has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity, or prevalence of the condition and the availability or lack of alternative treatments. As a condition of accelerated approval, the FDA will generally require the sponsor to perform adequate and well-controlled post-market clinical trials to verify and describe the anticipated effect on irreversible morbidity or mortality or other clinical benefit. As a condition for accelerated approval, the FDA also currently requires pre-approval of promotional materials, which could adversely impact the timing of the commercial launch of a product.
Even if a product qualifies for one or more of these programs, the FDA may later decide that the product no longer meets the conditions for qualification or decide that the time period for FDA review and approval will not be shortened. Furthermore, priority review, fast track designation, breakthrough therapy designation, and accelerated approval do not change the standards for approval but may expedite the development or approval process.
Orphan Drug Designation
Under the Orphan Drug Act, the FDA may grant orphan designation to a drug intended to treat a rare disease or condition, which is a disease or condition that affects fewer than 200,000 individuals in the U.S., or more than 200,000 individuals in the U.S. for which there is no reasonable expectation that the cost of developing and making available in the U.S. a drug for this type of disease or condition will be recovered from sales in the U.S. for that drug. Orphan designation must be requested before submitting an NDA. After the FDA grants orphan designation, the generic identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. The orphan drug designation in and of itself does not convey any advantage in, or automatically shorten the duration of, the regulatory review or approval process. However, a drug granted orphan status allows the sponsor to receive tax credits and a user fee waiver.
If a product that has orphan designation subsequently receives the first FDA approval for the disease for which it has such designation, the product is entitled to orphan drug exclusivity, which means that the FDA may not approve any other applications, including a full NDA, to market the same product for the same indication for seven years, except in limited circumstances, such as a showing of clinical superiority to the product with orphan drug exclusivity. Orphan drug exclusivity does not prevent FDA from approving a different drug for the same disease or condition, or the same drug for a different disease or condition. A designated orphan product may not receive orphan exclusivity if it is approved for a use that is broader than the indication for which it received orphan designation. In addition, exclusive marketing rights in the U.S. may be lost if the FDA later determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantities of the product to meet the needs of patients with the rare disease or condition.
Post-Approval Requirements
Any products manufactured or distributed by us pursuant to FDA approvals are subject to pervasive and continuing regulation by the FDA, including, among other things, requirements relating to quality control and quality assurance, record-keeping, reporting of adverse events, periodic reporting, product sampling, and distribution, and advertising and promotion of the product. After approval, most changes to the approved product, such as adding new indications or other labeling claims, are subject to FDA review and approval. Under continuing user fee requirements, the FDA assesses an annual program fee for each product identified in an approved NDA. Manufacturers and their subcontractors are required to register their establishments and list the drugs they manufacture with the FDA and certain state agencies, and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with GMPs, which impose certain procedural and documentation requirements upon us. Changes to the manufacturing process are strictly regulated, and, depending on the significance of the change, may require prior FDA approval before being implemented. FDA regulations also require investigation and correction of any deviations from GMPs and impose reporting requirements upon us and any third-party manufacturers or packagers that it may decide to use. Accordingly, manufacturers must continue to expend time, money, and effort in the area of production and quality control to maintain compliance with GMP and other aspects of regulatory compliance.
The FDA may withdraw approval if compliance with regulatory requirements and standards is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with manufacturing processes, or failure to comply with regulatory requirements, may result in revisions to the approved labeling to add new safety information; imposition of post-market studies or clinical trials to assess new safety risks; or imposition of distribution restrictions or other restrictions under a REMS program. Other potential consequences include, among other things:
| ● |
restrictions on the marketing or manufacturing of a product, mandated modification of promotional materials or issuance of corrective information, issuance by FDA or other regulatory authorities of safety alerts, Dear Healthcare Provider letters, press releases or other communications containing warnings or other safety information about the product, or complete withdrawal of the product from the market or product recalls; |
| ● |
fines, warning or untitled letters or holds on post-approval clinical trials; |
| ● |
refusal of the FDA to approve pending applications or supplements to approved applications, or suspension or revocation of existing product approvals; |
| ● |
product seizure or detention, or refusal of the FDA to permit the import or export of products; or |
| ● |
injunctions, consent decrees or the imposition of civil or criminal penalties. |
The FDA closely regulates the marketing, labeling, advertising and promotion of drugs and biologics. A company can make only those claims relating to safety, efficacy, and conditions of use of the drug that are approved by the FDA and in accordance with the provisions of the approved label. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses. Failure to comply with these requirements can result in, among other things, adverse publicity, warning letters, corrective advertising, and potential civil and criminal penalties. Physicians may prescribe legally available products for uses that are not described in the product’s labeling and that differ from those tested by us and approved by the FDA. Such off-label uses are common across medical specialties. Physicians may believe that such off-label uses are the best treatment for many patients in varied circumstances. The FDA does not regulate the behavior of physicians in their choice of treatments. The FDA does, however, restrict manufacturer’s communications on the subject of off-label use of their products.
Other U.S. Healthcare Laws and Compliance Requirements
In the U.S., our current and future operations are subject to regulation by various federal, state and local authorities in addition to the FDA, including but not limited to, the Centers for Medicare & Medicaid Services (“CMS”), which is part of the U.S. Department of Health and Human Services (“HHS”), as well as other divisions of HHS (such as the Office of Inspector General, Office for Civil Rights and the Health Resources and Service Administration), the U.S. Department of Justice (“DOJ”) and individual U.S. Attorney offices within the DOJ, and state and local governments. For example, our clinical research, sales, marketing and scientific/educational grant programs have to comply with the anti-fraud and abuse provisions of the Social Security Act (such as the Anti-Kickback Statute), the False Claims Act, the anti-fraud provisions of and the privacy and security provisions of regulations implementing the Health Insurance Portability and Accountability Act (“HIPAA”), the Drug Supply Chain Security Act (“DSCSA”), and similar state laws, each as amended, as applicable. Our business operations and current and future arrangements with investigators, healthcare professionals, consultants, third-party payors, patients, and customers may be subject to healthcare laws, regulations and enforcement by the federal government and by authorities in the states and foreign jurisdictions in which we conduct our business. Such laws govern, without limitation, state and federal anti-kickback, fraud and abuse, patient brokering, false claims, privacy and security, price reporting, drug distribution, and physician sunshine laws. Some of our pre-commercial activities are subject to some of these laws.
The federal Anti-Kickback Statute prohibits, among other things, any person or entity, from knowingly and willfully offering, paying, soliciting or receiving any remuneration, directly or indirectly, overtly or covertly, in cash or in kind, to induce or in return for purchasing, leasing, ordering or arranging for the purchase, lease or order of any item or service reimbursable, in whole or in part, under Medicare, Medicaid, or other federal healthcare programs. The term remuneration has been interpreted broadly to include anything of value. The Anti-Kickback Statute has been interpreted to apply to arrangements between therapeutic product manufacturers and prescribers, purchasers, and formulary managers. A number of statutory exceptions and regulatory safe harbors exist to protect certain activities from prosecution. Exceptions and safe harbors are drawn narrowly and practices involving remuneration that may be alleged to be intended to induce prescribing, purchasing, or recommending may be subject to scrutiny if they do not qualify for an exception or safe harbor. Failure to meet all the requirements of a particular applicable statutory exception or regulatory safe harbor does not make the activity per se illegal under the Anti-Kickback Statute. Instead, the legality of the activity will be evaluated on a case-by-case basis based on a cumulative review of all of its facts and circumstances. Our practices may not in all cases meet all the criteria for protection under a statutory exception or regulatory safe harbor.
Additionally, the intent standard under the Anti-Kickback Statute was amended by the Patient Protection and Affordable Care Act of 2010, as amended by the Health Care and Education Reconciliation Act of 2010 (collectively, the “Affordable Care Act”) to a stricter standard such provides that a person or entity no longer needs to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation. Violations of the Anti-Kickback Statute can result in significant civil and criminal fines and penalties, imprisonment, and exclusion from federal healthcare programs. In addition, a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal False Claims Act (discussed below). In addition, several states have similar state-level anti-kickback statutes.
The federal false claims and civil monetary penalty laws, including the False Claims Act, which imposes significant penalties and can be enforced by private citizens through civil qui tam actions, prohibit any person or entity from, among other things, knowingly presenting, or causing to be presented, a false or fraudulent claim for payment to, or approval by, the federal government, including federal healthcare programs, such as Medicare and Medicaid, knowingly making, using, or causing to be made or used a false record or statement material to a false or fraudulent claim to the federal government, or knowingly making a false statement to improperly avoid, decrease or conceal an obligation to pay money to the federal government. A claim includes “any request or demand” for money or property presented to the U.S. government. For instance, historically, pharmaceutical and other healthcare companies have been prosecuted under these laws for allegedly providing free product to customers with the expectation that the customers would bill federal programs for the product. Other companies have been prosecuted for causing false claims to be submitted because of the companies’ marketing of the product for unapproved, off-label, and thus generally non-reimbursable, uses. Penalties for federal civil False Claims Act violations may include up to three times the actual damages sustained by the government, plus significant mandatory civil penalties, and exclusion from participation in federal healthcare programs.
HIPAA created additional federal criminal statutes that prohibit, among other things, knowingly and willfully executing, or attempting to execute, a scheme to defraud or to obtain, by means of false or fraudulent pretenses, representations or promises, any money or property owned by, or under the control or custody of, any healthcare benefit program, including private third-party payors, willfully obstructing a criminal investigation of a healthcare offense, and knowingly and willfully falsifying, concealing or covering up by trick, scheme or device, a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. Like the Anti-Kickback Statute, the intent standard for certain healthcare fraud statutes under HIPAA does not require actual knowledge of the statute or specific intent to violate it in order to have committed a violation.
We may be subject to data privacy and security regulations by both the federal government and the states in which we conduct our business. HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act (“HITECH”), and its implementing regulations, imposes requirements relating to the privacy, security and transmission of individually identifiable health information. Among other things, HITECH makes HIPAA’s privacy and security standards directly applicable to business associates, which are independent contractors or agents of covered entities that create, receive, maintain, or transmit protected health information in connection with providing a service on behalf of, to or for a covered entity as well as their covered subcontractors. HITECH also created four new tiers of civil monetary penalties, amended HIPAA to make civil and criminal penalties directly applicable to business associates, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce HIPAA and seek attorneys’ fees and costs associated with pursuing federal civil actions. In addition, many state laws govern the privacy and security of health information in specified circumstances, many of which differ from each other in significant ways, are often not pre-empted by HIPAA, and may have a more prohibitive effect than HIPAA, thus complicating compliance efforts.
Additionally, the federal Physician Payments Sunshine Act, and its implementing regulations, require that certain manufacturers of drugs, devices, biological and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program (with certain exceptions) report annually to CMS information related to certain payments or other transfers of value made or distributed to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, or to entities or individuals at the request of, or designated on behalf of, the physicians and teaching hospitals and to report annually certain ownership and investment interests held by physicians and their immediate family members. Failure to report accurately could result in penalties. Beginning in 2022, applicable manufacturers also will be required to report such information regarding its payments and other transfers of value to physician assistants, nurse practitioners, clinical nurse specialists, anesthesiologist assistants, certified registered nurse anesthetists and certified nurse midwives during the previous year. In addition, many states have similar statutes or regulations to the above federal laws that may be broader in scope and may apply regardless of payor. We may also be subject to state laws that require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government, and/or state laws that require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers, drug pricing or marketing expenditures. These laws may differ from each other in significant ways, further complicating compliance efforts. Additionally, to the extent that we have business operations in foreign countries or sell any of our products in foreign countries and jurisdictions, including Canada or the E.U., we may be subject to additional regulation.
We may someday develop products that, once approved, may be administered by a physician. Under currently applicable U.S. law, certain products not usually self-administered (including injectable drugs) may be eligible for coverage under Medicare through Medicare Part B. Medicare Part B is part of original Medicare, the federal healthcare program that provides healthcare benefits to the aged and disabled, and covers outpatient services and supplies, including certain biopharmaceutical products, which are medically necessary to treat a beneficiary’s health condition. As a condition of receiving Medicare Part B reimbursement for a manufacturer’s eligible drugs, the manufacturer is required to participate in other government healthcare programs, including the Medicaid Drug Rebate Program and the 340B Drug Pricing Program. The Medicaid Drug Rebate Program requires pharmaceutical manufacturers to enter into and have in effect a national rebate agreement with the Secretary of HHS as a condition for states to receive federal matching funds for the manufacturer’s outpatient drugs furnished to Medicaid patients. Under the 340B Drug Pricing Program, the manufacturer must extend discounts to entities that participate in the program.
In addition, many pharmaceutical manufacturers must calculate and report certain price reporting metrics to the government, such as average sales price and best price. Penalties may apply in some cases when such metrics are not submitted accurately and timely. Further, these prices for drugs may be reduced by mandatory discounts or rebates required by government healthcare programs or private payors and by any future relaxation of laws that presently restrict imports of drugs from countries where they may be sold at lower prices than in the U.S. It is difficult to predict how Medicare coverage and reimbursement policies will be applied to our products in the future and coverage and reimbursement under different federal healthcare programs are not always consistent. Medicare reimbursement rates may also reflect budgetary constraints placed on the Medicare program.
In order to distribute products commercially, we must comply with state laws that require the registration of manufacturers and wholesale distributors of drug products in a state, including, in certain states, manufacturers and distributors who ship products into the state even if such manufacturers or distributors have no place of business within the state. The federal government as well as some states also impose requirements on manufacturers and distributors to maintain records regarding the history of products in the chain of distribution. Federal law requires manufacturers to provide product tracing information to subsequent supply chain partners. The DSCSA governs the system of tracing certain prescription drugs as they are distributed in the U.S. A goal of the DSCSA is to protect consumers from drugs that may be counterfeit, contaminated, stolen, or adulterated. The law requires manufacturers to, prior to or at the time of each transfer of ownership of a drug, provide the subsequent owner with transaction history, transaction information, and a transaction statement. In the event of a recall or an inquiry regarding a potentially illegitimate product, manufacturers must be able to provide information regarding the transaction history and transaction information of their products. Violations of the DSCSA may result in fines or imprisonment. In addition, many states regulate manufacturers and enforce recordkeeping and licensure requirements.
Several states have enacted legislation requiring pharmaceutical and biotechnology companies to establish marketing compliance programs, file periodic reports with the state, make periodic public disclosures on sales, marketing, pricing, clinical trials and other activities, and/or register their sales representatives, as well as to prohibit pharmacies and other healthcare entities from providing certain physician prescribing data to pharmaceutical and biotechnology companies for use in sales and marketing, and to prohibit certain other sales and marketing practices. All our activities are potentially subject to federal and state consumer protection and unfair competition laws.
Ensuring business arrangements with third parties comply with applicable healthcare laws and regulations is a costly endeavor. If our operations are found to be in violation of any of the federal and state healthcare laws described above or any other current or future governmental regulations that apply to us, we may be subject to penalties, including without limitation, civil, criminal and/or administrative significant penalties, damages, fines, disgorgement, imprisonment, exclusion from participation in government programs, such as Medicare and Medicaid, injunctions, private “qui tam” actions brought by individual whistleblowers in the name of the government, or refusal to allow us to enter into government contracts, contractual damages, reputational harm, administrative burdens, diminished profits and future earnings, additional reporting obligations and oversight if we become subject to a corporate integrity agreement or other agreement to resolve allegations of non-compliance with these laws, and the curtailment or restructuring of our operations, any of which could adversely affect our ability to operate our business and our results of operations.
Coverage, Pricing and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of any drug candidates for which we may obtain regulatory approval. In the U.S. and in foreign markets, sales of any products for which we receive regulatory approval for commercial sale will depend, in part, on the extent to which third-party payors provide coverage and establish adequate reimbursement levels for such products. In the U.S., third-party payors include federal and state healthcare programs, private managed care providers, health insurers and other organizations. Adequate coverage and reimbursement from governmental healthcare programs, such as Medicare and Medicaid in the U.S., and commercial payors are critical to new product acceptance.
Our ability to commercialize any products successfully also will depend in part on the extent to which coverage and reimbursement for these products and related treatments will be available from third-party payors, which decide which therapeutics they will pay for and establish reimbursement levels. Coverage and reimbursement by a third-party payor may depend upon a number of factors, including the third-party payor’s determination that use of a therapeutic is:
| ● |
a covered benefit under its health plan; |
| ● |
safe, effective and medically necessary; |
| ● |
appropriate for the specific patient; |
| ● |
cost-effective; and |
| ● |
neither experimental nor investigational. |
We cannot be sure that coverage or reimbursement will be available for any product that we commercialize and, if coverage and reimbursement are available, what the level of reimbursement will be. Coverage may also be more limited than the purposes for which the product is approved by the FDA or comparable foreign regulatory authorities. Reimbursement may impact the demand for, or the price of, any product for which we obtain regulatory approval.
Third-party payors are increasingly challenging the price, examining the medical necessity, and reviewing the cost-effectiveness, of medical products, therapies and services, in addition to questioning their safety and efficacy. Obtaining reimbursement for our products may be particularly difficult because of the higher prices often associated with branded drugs and drugs administered under the supervision of a physician. We may need to conduct expensive pharmacoeconomic studies in order to demonstrate the medical necessity and cost-effectiveness of our products, in addition to the costs required to obtain FDA approvals. Our drug candidates may not be considered medically necessary or cost-effective by payors. Obtaining coverage and reimbursement approval of a product from a government or other third-party payor is a time-consuming and costly process that could require us to provide to each payor supporting scientific, clinical and cost-effectiveness data for the use of our product on a payor-by-payor basis, with no assurance that coverage and adequate reimbursement will be obtained. A payor’s decision to provide coverage for a product does not imply that an adequate reimbursement rate will be approved. Further, one payor’s determination to provide coverage for a product does not assure that other payors will also provide coverage for the product. Adequate third-party reimbursement may not be available to enable us to maintain price levels sufficient to realize an appropriate return on its investment in product development. If reimbursement is not available or is available only at limited levels, we may not be able to successfully commercialize any drug candidate that we successfully develop.
Different pricing and reimbursement schemes exist in other countries. For example, in the E.U., governments influence the price of biopharmaceutical products through their pricing and reimbursement rules and control of national health care systems that fund a large part of the cost of those products to consumers. Some jurisdictions operate positive and negative list systems under which products may only be marketed once a reimbursement price has been agreed. To obtain reimbursement or pricing approval, some of these countries may require the completion of clinical trials that compare the cost effectiveness of a particular drug candidate to currently available therapies. Other member states allow companies to establish their own prices for medicines, but monitor and control company profits. The downward pressure on health care costs has become intense. As a result, increasingly high barriers are being erected to the entry of new products. In addition, in some countries, cross-border imports from low-priced markets exert a commercial pressure on pricing within a country.
The marketability of any drug candidates for which we receive regulatory approval for commercial sale may suffer if the government and third-party payors fail to provide adequate coverage and reimbursement. In addition, political and economic pressures as well as legislative changes in the U.S. have increased, and we expect will continue to increase, the pressure on drug pricing. The downward pressure on the rise in healthcare costs in general, particularly prescription medicines, medical devices and surgical procedures and other treatments, has become very intense. Coverage policies and third-party reimbursement rates may change at any time. Even if favorable coverage and reimbursement status is attained for one or more products for which we receive regulatory approval, less favorable coverage policies and reimbursement rates may be implemented in the future.
Healthcare Reform
In the U.S. and some foreign jurisdictions, there have been, and continue to be, several legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval of drug candidates, restrict or regulate post-approval activities, and affect the ability to profitably sell drug candidates for which marketing approval is obtained. Among policy makers and payors in the U.S. and elsewhere, there is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality and/or expanding access. In the U.S., the pharmaceutical industry has been a particular focus of these efforts and has been significantly affected by major legislative initiatives.
Some of the provisions of the Affordable Care Act have yet to be implemented, and there have been legal and political challenges to certain aspects of the Affordable Care Act. For example, on June 17, 2021, the U.S. Supreme Court dismissed a challenge on procedural grounds that argued the Affordable Care Act is unconstitutional in its entirety because the “individual mandate” was repealed by Congress. Thus, the Affordable Care Act will remain in effect in its current form. Further, prior to the U.S. Supreme Court ruling, on January 28, 2021, President Biden issued an executive order that initiated a special enrollment period for purposes of obtaining health insurance coverage through the Affordable Care Act marketplace, which began on February 15, 2021 and remained open through August 15, 2021. The executive order also instructed certain governmental agencies to review and reconsider their existing policies and rules that limit access to healthcare, including among others, reexamining Medicaid demonstration projects and waiver programs that include work requirements, and policies that create unnecessary barriers to obtaining access to health insurance coverage through Medicaid or the Affordable Care Act. It is possible that the Affordable Care Act will be subject to judicial or Congressional challenges in the future. It is unclear how any such challenges and the healthcare reform measures of the Biden administration will impact the Affordable Care Act and our business.
Further legislation or regulation could be passed that could harm our business, financial condition and results of operations. Other legislative changes have been proposed and adopted since the Affordable Care Act was enacted. For example, in August 2011, President Obama signed into law the Budget Control Act of 2011, which, among other things, included aggregate reductions to Medicare payments to providers of 2% per fiscal year, which went into effect beginning on April 1, 2013 and will stay in effect through 2030 unless additional Congressional action is taken, with COVID-19 relief legislation suspending the 2% Medicare sequester from May 1, 2020 through December 31, 2021. In January 2013, the American Taxpayer Relief Act of 2012 was signed into law, which, among other things, further reduced Medicare payments to several types of providers, including hospitals, imaging centers and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. Additionally, on March 11, 2021, President Biden signed the American Rescue Plan Act of 2021 into law, which eliminates the statutory Medicaid drug rebate cap, currently set at 100% of a drug’s average manufacturer price, for single source and innovator multiple source drugs, beginning January 1, 2024.
Additionally, there has been increasing legislative and enforcement interest in the U.S. with respect to specialty drug pricing practices. Specifically, there have been several recent U.S. Congressional inquiries and proposed federal legislation designed to, among other things, bring more transparency to drug pricing, reduce the cost of prescription drugs under Medicare, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for drugs. Congress has indicated that it will continue to seek new legislative and/or administrative measures to control drug costs. Additionally, based on a recent executive order, the Biden administration expressed its intent to pursue certain policy initiatives to reduce drug prices. In response to Biden’s executive order, on September 9, 2021, HHS released a Comprehensive Plan for Addressing High Drug Prices that outlines principles for drug pricing reform and sets out a variety of potential legislative policies that Congress could pursue to as well as potential administrative actions HHS can take to advance these principles. No legislation or administrative actions have been finalized to implement these principles. In addition, Congress is considering drug pricing as part of the budget reconciliation process. Individual states in the U.S. have also become increasingly active in passing legislation and implementing regulations designed to control biopharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing.
On August 7, 2022, the U.S. Congress passed the Inflation Reduction Act of 2022, which delayed the implementation of the changes to the Medicare Part D drug rebate program and the U.S. Federal Anti-Kickback Statute until January 2032.
Additionally, the Inflation Reduction Act of 2022 may impact existing Medicare programs that cover prescription drugs. In addition to other relevant provisions, the Inflation Reduction Act of 2022 allows the Medicare program to directly negotiate the price of certain high-expenditure prescription drugs covered under Medicare Parts B and D, starting in the year 2028 and 2026, respectively, by setting certain “maximum fair prices.” Moreover, the Inflation Reduction Act of 2022 requires manufacturers to pay rebates to the U.S. federal government if prices of certain drugs covered under the Medicare program rise faster than the rate of inflation.
The Foreign Corrupt Practices Act
The Foreign Corrupt Practices Act, prohibits any U.S. individual or business from paying, offering, or authorizing payment or offering of anything of value, directly or indirectly, to any foreign official, political party or candidate for the purpose of influencing any act or decision of the foreign entity in order to assist the individual or business in obtaining or retaining business. The Foreign Corrupt Practices Act also obligates companies whose securities are listed in the U.S. to comply with accounting provisions requiring us to maintain books and records that accurately and fairly reflect all transactions of the corporation, including international subsidiaries, and to devise and maintain an adequate system of internal accounting controls for international operations.
Smaller Reporting Company Status
We are a “smaller reporting company” because the market value of our stock held by non-affiliates was less than $250 million as of June 30, 2023. We may continue to be a smaller reporting company in any given year if either (i) the market value of our stock held by non-affiliates is less than $250 million as of June 30 in the most recently completed fiscal year or (ii) our annual revenue is less than $100 million during the most recently completed fiscal year and the market value of our stock held by non-affiliates is less than $700 million as of June 30 in the most recently completed fiscal year. As a smaller reporting company, we are eligible for and may take advantage of certain exemptions from various reporting requirements applicable to other public companies for as long as we continue to be a smaller reporting company, including (i) the choice of presenting only the two most recent fiscal years of audited financial statements in our Annual Report on Form 10-K, (ii) the exemption from the auditor attestation requirements with respect to internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act, and (iii) reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements.
Other Regulations
In addition to the foregoing, state and federal laws regarding environmental protection and hazardous substances, including the Occupational Safety and Health Act, the Resource Conservation and Recovery Act and the Toxic Substances Control Act, affect our business. These and other laws govern our use, handling and disposal of various biological, and chemical substances used in, and wastes generated by, our operations. If our operations result in contamination of the environment or expose individuals to hazardous substances, we could be liable for damages and governmental fines. We believe that we are in material compliance with applicable environmental laws and that continued compliance therewith will not have a material adverse effect on our business. We cannot predict, however, how changes in these laws may affect our future operations.
We are also subject to numerous federal, state and local laws relating to such matters as safe working conditions, manufacturing practices, and fire hazard control. We may incur significant costs to comply with such laws and regulations now or in the future.
Employees and Human Capital Resources
As of December 31, 2023, we had a total of 85 employees, 82 of which were full-time, primarily located in Utah and Maryland. The table below sets forth our employees by role:
| Department |
Count of Employees |
Percent of Total |
||||||
| Manufacturing |
21 | 25 | % | |||||
| Clinical |
7 | 8 | % | |||||
| Quality Control & Bioanalytics |
10 | 12 | % | |||||
| Microbiology Lab |
9 | 11 | % | |||||
| Research and Development |
11 | 13 | % | |||||
| Senior Management |
6 | 7 | % | |||||
| Quality Assurance |
8 | 9 | % | |||||
| Finance |
5 | 6 | % | |||||
| Human Resources |
4 | 5 | % | |||||
| Information Technology |
1 | 1 | % | |||||
| Regulatory |
1 | 1 | % | |||||
| Medical Affairs |
1 | 1 | % | |||||
| Marketing |
1 | 1 | % | |||||
| Total |
85 | 100 | % | |||||
None of our employees are represented by a labor union or are covered by a collective bargaining agreement, and we believe that we have good relations with our employees.
Our human capital resources objectives include, as applicable, identifying, recruiting, retaining, incentivizing, and integrating our existing and additional employees. The principal purposes of our equity incentive plans are to attract, retain, and motivate selected employees, consultants and directors through the granting of stock-based compensation awards and cash-based performance bonus awards.
Corporate Information
The mailing address for our principal executive office is 6550 South Millrock Drive, Suite G50, Salt Lake City, Utah 84121, and our telephone number is (801) 676-9695. Our website address is https://clene.com. The information contained in or accessible from any website referred to in this Form 10-K is not incorporated into this Annual Report, and you should not consider it part of this Annual Report. We have included our website address in this Annual Report solely as an inactive textual reference.
Investing in our securities involves a high degree of risk. You should carefully consider the risks and uncertainties described below, together with the other information in this Annual Report, including our consolidated financial statements and the related notes and “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” before deciding whether to invest in our securities. The occurrence of one or more of the events or circumstances described in these risk factors, alone or in combination with other events or circumstances, may have a material adverse effect on our business, reputation, revenue, financial condition, results of operations, and future prospects, in which event the market price of our Common Stock could decline, and you could lose part or all of your investment. The risks and uncertainties summarized above and described below are not intended to be exhaustive and are not the only ones we face. Additional risks and uncertainties not presently known to us or that we currently deem immaterial may also impair our business operations. This Annual Report also contains forward-looking statements that involve risks and uncertainties, refer to “Cautionary Note Regarding Forward-Looking Statements.” Our actual results could differ materially and adversely from our anticipated results as a result of a number of factors, including the risks described below.
Risks Relating to Our Business and Industry
We depend substantially on the successful commercialization of our drug candidates in the future, which may fail to materialize or may experience significant delays.
As a new biopharmaceutical business, we currently do not have any drugs available for commercial sales nor do we have any drugs that have been approved for sale by the regulatory authorities. We have invested a significant portion of our efforts and financial resources in research and development of our leading drug candidate, CNM-Au8, a catalytically-active gold nanocrystal suspension, which in early-stage studies has shown potential for the treatment of patients with ALS, MS, and PD. Our ability to generate revenue and become profitable in the future depends substantially on the future sales generated by CNM-Au8 and our drug candidates, which in turn depends on the successful research and development, regulatory approval, commercialization and sale of our drug candidates presently under clinical development for the treatment of patients with neurological disorders. We are also developing new drugs based on our technology that have not yet entered into human studies. The ultimate success of our drug candidates is subject to us achieving certain milestones, including without limitation:
| ● |
identifying, assessing, acquiring and obtaining evidence of biological activity of new drug candidates to treat certain diseases; |
| ● |
obtaining satisfactory evidence of safety of these drug candidates in animal toxicology studies; |
| ● |
obtaining regulatory approval for the conduct of, enrollment in, and completion of, clinical trials of our drug candidates; |
| ● |
obtaining satisfactory proof of the clinical efficacy and safety of our drug candidates from these clinical trials; |
| ● |
obtaining approvals and marketing authorizations from regulatory authorities for our drug candidates; |
| ● |
developing sustainable and scalable manufacturing processes to produce these drug candidates; |
| ● |
successfully expanding manufacturing processes to support global commercialization capacity of our drug candidates; and |
| ● |
launching and commercializing any drug candidates for which we may obtain regulatory approvals and marketing authorizations, either directly or with a collaborator or distributor. |
If we do not achieve one or more of these milestones in a timely manner, or at all, we could experience significant delays in our ability to obtain approval for and/or to successfully commercialize our drug candidates, which could materially harm our business and we may not be able to generate sufficient revenues and cash flows to continue our operations.
Even if we are able to generate revenues from any future sales of our drug candidates, we may not become profitable and may need to obtain additional funding to continue operations. Any required funding may not be available on favorable terms or at all. If we fail to become profitable or are unable to sustain profitability on a continuing basis, then we may be unable to continue our operations at planned levels and may be forced to reduce our operations. Even if we do achieve profitability, we may not be able to sustain or increase profitability on a quarterly or annual basis. Our failure to become and remain profitable would decrease our value significantly and could impair our ability to raise capital, expand our business or continue our operations, which in turn may adversely affect our business, financial condition, and results of operations.
We currently do not generate any revenue from the commercial sales of drug candidates and we may not become profitable when expected, or at all.
Our main business is research and development, and if successful, sales of drug candidates. As all of our drug candidates are still in the research and development stage, we currently do not generate revenue from the sale of drug candidates, and we have recorded continued significant net losses. We generate an immaterial amount of revenue related to license and supply agreements for dietary (mineral) supplements; however, such revenue is not expected to be a material contributor to our revenue in the future. If we fail to commercialize our drug candidates as planned due to failures to complete clinical trials, obtain regulatory approval, conduct commercial scale manufacturing or for any other reason, we may experience significant delays or failure in generating revenue and realizing profit from the commercial sale of our drug candidates.
Further, we expect to incur significant costs in the future, in particular for research and development and the commercialization of our drug candidates. Research and development expenses totaled $26.7 million and $31.9 million for the years ended December 31, 2023 and 2022, respectively. As drug candidates presently undergoing preclinical research enter into the clinical trial stage, costs associated with such drug candidates may increase significantly. In the future, as we move more drug candidates into the clinical trial stage, conduct more clinical trials for commercialized products, if any, to broaden their use, and carry out commercial production of our drug candidates, the costs associated with such operations may increase significantly.
As we operate in the highly competitive pharmaceutical market, we compete to commercialize our drug candidates ahead of our competitors, putting us under pressure to incur research and development and other expenses with a potential negative impact on our profitability. On the other hand, our commercialized drug candidates, if any are approved, may fail to realize their sales potential due to competition, insufficient market demand, product defects, or any other reason. Therefore, even if we ever start to generate revenue from the sales of our commercialized drug candidates in the future, we may still not be profitable for an extended period of time or at all.
We have incurred significant net losses and net operating cash outflows since our inception and expect to continue to incur significant net losses for the foreseeable future.
Investment in biopharmaceutical drug development is highly speculative. It entails substantial upfront capital expenditures and significant risk that a drug candidate might fail to gain regulatory approval or become commercially viable. We continue to incur significant expenses related to our ongoing operations. We have incurred substantial losses since our inception. We incurred a loss from operations of $40.5 million and $48.4 million for the years ended December 31, 2023 and 2022, respectively, and a net loss of $49.5 million and $29.9 million for the years ended December 31, 2023 and 2022, respectively. Our accumulated deficit was $242.7 million and $193.2 million as of December 31, 2023 and 2022, respectively. For details, see “Management’s Discussion and Analysis of Financial Condition and Results of Operations.” Substantially all of our operating losses have resulted from costs incurred in connection with our research and development programs and administrative expenses associated with our operations, and we expect that our research and development expenses will continue to increase in the future.
We expect to continue to incur losses for the foreseeable future, and we expect these losses to increase as we continue to expand our development of, and seek regulatory approvals for, our drug candidates, and we continue to build up our commercialization capabilities. Typically, it takes many years to develop one new drug from the drug discovery stage to the time it is available for treating patients. In addition, we will continue to incur costs associated with operating as a public company and in support of our growth as a development-stage or commercial-stage pharmaceutical company. The size of our future net losses will depend, in part, on the number and scope of our drug development programs and the associated costs of those programs, the cost of commercializing any approved products, our ability to generate revenues and the timing and amount of milestones and other payments we make or receive through arrangements with third parties. If any of our drug candidates fails in clinical trials or does not gain regulatory approval, or if approved, fails to achieve market acceptance, we may never become profitable. Our failure to become and remain profitable would decrease our value significantly and impair our ability to raise capital, maintain our research and development efforts, expand our business or continue our operations.
Our ability to continue as a going concern requires that we obtain sufficient funding to finance our operations, which may not be available on acceptable terms, or at all. A failure to obtain this necessary capital when needed could force us to delay, limit, reduce or terminate our drug development or commercialization efforts.
Our cash, cash equivalents, and marketable securities totaled $35.0 million and $23.3 million as of December 31, 2023 and 2022, respectively, and net cash used in operating activities was $30.2 million and $39.0 million for the years ended December 31, 2023 and 2022, respectively. We expect to continue to incur losses and use cash in operating activities for the foreseeable future. For details, please see “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Liquidity and Capital Resources.” We expect that within the next twelve months, we will not have sufficient cash and other resources on hand to sustain our current operations or meet our obligations as they become due unless we obtain additional financing. Additionally, pursuant to our term loan with Avenue Venture Opportunities Fund, L.P. (“Avenue”), we are required to maintain unrestricted cash and cash equivalents of at least $5.0 million to avoid acceleration of the full balance of the loan (see Note 8 to the consolidated financial statements). These conditions raise substantial doubt about the Company’s ability to continue as a going concern.
To mitigate our funding needs, we plan to raise additional funding, including exploring equity financing and offerings, debt financing, licensing or collaboration arrangements with third parties, as well as utilizing our existing at-the-market facility, equity purchase agreement, and potential proceeds from the exercise of outstanding warrants and stock options. These plans are subject to market conditions and reliance on third parties, and there is no assurance that effective implementation of our plans will result in the necessary funding to continue current operations. We have implemented cost-saving initiatives, including delaying and reducing certain research and development programs and commercialization efforts and elimination of certain staff positions. We have concluded that our plans do not alleviate the substantial doubt about our ability to continue as a going concern beyond one year from the date the consolidated financial statements are issued.
Unstable market and economic conditions may have serious adverse consequences on our business, financial condition, results of operations, and prospects.
As a result of changes in the macro environment, including those resulting from geo-political actions, such as the U.S. and foreign government responses to the ongoing conflicts between Ukraine and Russia and Israel and Palestine, the global credit and financial markets have experienced extreme volatility and disruptions, including severely diminished liquidity and credit availability, declines in consumer confidence, and uncertainty about economic stability. There can be no assurance that further deterioration in credit and financial markets and confidence in economic conditions will not occur. Our financing strategy may be adversely affected by any such economic downturn, volatile business environment, or continued unpredictable and unstable market conditions. If the current equity and credit markets deteriorate, it may make any necessary debt or equity financing more difficult, more costly, and more dilutive. Failure to secure any necessary financing in a timely manner and on favorable terms could have a material adverse effect on our business, financial condition, results of operations, and prospects, and could require us to delay or abandon clinical development plans. In addition, one or more of our current CROs, clinical investigators, third-party vendors and clinical sites, and other suppliers may not survive an economic downturn, which could directly affect our ability to achieve our operating goals within our desired timeline and budget.
We have a limited operating history, which may make it difficult to evaluate our current business and predict our future performance.
We are a biopharmaceutical company formed in December 2012 focusing on the discovery and development of innovative drugs for the treatment of neurological diseases and other disorders. Our limited operating history, particularly in light of the rapidly evolving nanocrystal therapies field, may make it difficult to evaluate our current business and predict our future performance.
Investment in biopharmaceutical product development is highly speculative because it entails substantial upfront capital expenditures and significant risk that any potential drug candidate will fail to demonstrate adequate efficacy or an acceptable safety profile, gain regulatory approval and become commercially viable. As a relatively new business, we have not yet demonstrated an ability to manufacture drugs at a commercial scale, to arrange for a third party to do so on our behalf, or to conduct sales and marketing activities necessary for successful commercialization. We have not had any product approved for commercial sale and have not generated any revenue from product sales. In addition, as a business with a limited operating history, we may encounter unforeseen expenses, difficulties, complications, delays and other known and unknown factors and risks frequently experienced by early-stage biopharmaceutical companies in rapidly evolving fields. Consequently, any assessment you make about our current business or future success or viability may not be as accurate as it could be if we had a longer operating history and had been able to reduce some of the uncertainties as set out above. Further, our limited financial track record, without any revenue yet from our expected future principal business, may be of limited reference value for your assessment of our business.
We may encounter difficulties in managing our growth and expanding our operations successfully, which could adversely affect our business, financial condition, results of operations, and prospects.
As we seek to advance our drug candidates through clinical trials, we will need to expand our development, regulatory, compliance, manufacturing, marketing and sales capabilities or contract with third parties to provide these capabilities for us. As our operations expand, we expect that we will need to manage additional relationships with various strategic partners, suppliers and other third parties. Future growth will impose significant added responsibilities on members of our management. Our future financial performance and our ability to commercialize our drug candidates, if approved, and to compete effectively will depend, in part, on our ability to manage any future growth effectively. To that end, we must be able to manage our development efforts and clinical trials effectively and hire, train and integrate additional clinical, regulatory, manufacturing, financial, legal, managerial, administrative, and sales and marketing personnel. We may not be able to accomplish these tasks, and our failure to accomplish any of them could prevent us from successful growth and could harm our business, financial condition, results of operations, and prospects.
Changes in government regulation or in practices relating to the pharmaceutical and biotechnology industries, including potential healthcare reform, could decrease the need for our drug candidates, or make it more difficult to obtain regulatory approvals for our drug candidates and commercialize them.
In recent years, the U.S. Congress, the President, executive branch agencies, and state legislatures have considered various types of healthcare reform to control growing healthcare costs. Similar reform movements have occurred in parts of Europe and Asia. Healthcare reform legislation could also increase the costs of drug development and commercialization or limit reimbursement for marketed drugs that could limit the profits to be made from the development of new drugs. This could adversely affect research and development expenditures by pharmaceutical and biotechnology companies, which could in turn decrease the business opportunities available to us in the U.S. and other countries. We are unable to predict what reform proposals will be adopted in the future, if any.
If we, or any CRO we may engage, fail to comply with environmental, health and safety laws and regulations, we could become subject to fines or penalties or incur costs that could have a material adverse effect on our business, financial condition, results of operations, and prospects.
We and certain of the third parties we contract with, such as our third-party CROs, are subject to numerous environmental, health and safety laws and regulations, including those governing laboratory procedures and the handling, use, storage, treatment, and disposal of hazardous materials and wastes. In addition, our future construction projects may necessitate that certain regulatory procedures be completed with the relevant administrative authorities in charge of environmental protection, health and safety before the project can be put into operation. Our operations involve the use of hazardous and flammable materials, including chemicals and biological materials. Our operations also produce hazardous waste products. We generally contract with third parties for the disposal of these materials and wastes. We cannot entirely eliminate the risk of contamination or injury from these materials. In the event of contamination or injury resulting from our use of hazardous materials, we could be held liable for any resulting damages, and any liability could exceed our resources.
Although we maintain workers’ compensation insurance to cover the costs and expenses we may incur due to injuries to our employees resulting from the use of or exposure to hazardous materials, this insurance may not provide adequate coverage against potential liabilities. We do not maintain insurance for environmental liability or toxic tort claims that may be asserted against us in connection with our storage, use or disposal of biological or hazardous materials.
In addition, the environmental, health and safety laws and regulations applicable to us and our third-party contractors may change and impose stricter requirements in the future. As a result, we may be required to incur substantial costs to comply with future environmental, health and safety laws and regulations. These current or future laws and regulations may impair our research, development or production efforts. Failure to comply with these laws and regulations also may result in substantial fines, penalties or other sanctions, which could have a material adverse effect on our business, financial condition, results of operations, and prospects.
Our internal computer systems, or those used by any CROs or other third-party contractors or consultants we may engage, may fail or suffer security breaches.
Despite the implementation of security measures, our internal computer systems and those of our CROs and other contractors and consultants are vulnerable to damage from computer viruses and unauthorized access. Although, to our knowledge, we have not experienced any material system failure or security breach to date, if such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our development programs and business operations.
In the ordinary course of our business, we collect and store sensitive data, including, among other things, legally protected patient health information, personally identifiable information about our employees, intellectual property, and proprietary business information. We manage and maintain our applications and data utilizing on-site systems and outsourced vendors. These applications and data encompass a wide variety of business-critical information including research and development information, commercial information, and business and financial information. Because information systems, networks and other technologies are critical to many of our operating activities, shutdowns or service disruptions of our systems or those of the vendors that provide information systems, networks or other services to us pose increasing risks. Such disruptions may be caused by events such as computer hacking, phishing attacks, ransomware, dissemination of computer viruses, worms and other destructive or disruptive software, denial-of-service attacks and other malicious activity, as well as security incidents from inadvertent or intentional actions (such as error or theft) by our employees, contractors, consultants, business partners, and/or other third parties, supply chain attacks, power outages, natural disasters (including extreme weather), terrorist attacks or other similar events. Such events could have an adverse impact on us and our business, including loss of data and damage to equipment and data. In addition, system redundancy may be ineffective or inadequate, and our disaster recovery planning may not be sufficient to cover all eventualities. Significant events could result in a disruption of our operations, damage to our reputation or a loss of revenues. In addition, we may not have adequate insurance coverage to compensate for any losses associated with such events.
We could be subject to risks caused by misappropriation, misuse, leakage, falsification or intentional or accidental release or loss of information maintained in our information systems and networks and those of our vendors, including personal information of our employees and patients, and company and vendor confidential data. In addition, outside parties may attempt to penetrate our systems or those of our vendors or fraudulently induce our personnel or the personnel of our vendors to disclose sensitive information in order to gain access to our data and/or systems. Like other companies, we have on occasion experienced, and will continue to experience, threats to our data and systems, including malicious codes and viruses, phishing and other cyber-attacks. The number and complexity of these threats continue to increase over time. If a material breach of our information technology systems or those of our vendors occurs, the market perception of the effectiveness of our security measures could be harmed and our reputation and credibility could be damaged. We could be required to expend significant amounts of money and other resources to repair or replace information systems or networks.
Moreover, despite our efforts, the possibility of these events occurring cannot be eliminated entirely. As we outsource more of our information systems to vendors, engage in more electronic transactions with payors and patients and rely more on cloud-based information systems, the related security risks will increase and we will need to expend additional resources to protect our technology and information systems.
We may also be required to comply with laws, regulations, rules, industry standards, and other legal obligations that require us to maintain the security of personal data. We may also have contractual and other legal obligations to notify customers, collaborators, or other relevant stakeholders of security incidents. Failure to prevent or mitigate cyberattacks could result in unauthorized access to data, including proprietary and personal information. Most jurisdictions have enacted laws requiring companies to notify individuals, regulatory authorities, and others of security breaches involving certain types of data. Such disclosures are costly, could lead to negative publicity, may cause our customer or collaborators or other relevant stakeholders to lose confidence in the effectiveness of our security measures and require us to expend significant capital and other resources to respond to and/or alleviate problems caused by the actual or perceived security incident. In addition, the costs to respond to a cybersecurity event or to mitigate any identified security vulnerabilities could be significant, including costs for remediating the effects of such an event, paying a ransom, restoring data from backups, and conducting data analysis to determine what data may have been affected by the breach. In addition, our efforts to contain or remediate a security incident or any vulnerability exploited to cause an incident may be unsuccessful, and efforts and any related failures to contain or remediate them could result in interruptions, delays, harm to our reputation, and increases to our insurance coverage.
In addition, regulatory response or litigation resulting from security breaches may adversely affect our business. Unauthorized access to our information technology systems could result in litigation with our customers, collaborators, or other relevant stakeholders, or regulatory actions by government entities. These proceedings could force us to spend money in defense or settlement, divert management’s time and attention, increase our costs of doing business, or adversely affect our reputation. We could be required to fundamentally change our business activities and practices in response to such litigation, which could have an adverse effect on our business. If a security breach were to occur and the confidentiality, integrity or availability of our data or the data of our collaborators were disrupted, we could incur significant liability, which could negatively affect our business and damage our reputation.
Furthermore, our insurance may not be adequate to cover losses associated with such events, and in any case, such insurance may not cover all of the types of costs, expenses, or at all, and losses we could incur to respond to and remediate a security breach. The successful assertion of one or more large claims against us that exceeds our available insurance coverage, or results in changes to our insurance policies (including premium increases or the imposition of large deductible or co-insurance requirements), could have an adverse effect on our business. In addition, we cannot be sure that our existing insurance coverage and coverage for errors and omissions will continue to be available on acceptable terms or that our insurers will not deny coverage as to any future claim.
We manufacture all of our drug candidates ourselves, and intend to manufacture most, if not all, of any approved drugs ourselves as well, which could have a material adverse effect on our business, financial condition, results of operations, and prospects.
We currently have manufacturing facilities in the U.S. and may build additional manufacturing facilities in other markets to expand our manufacturing capacity. These facilities may encounter unanticipated delays and expenses due to a number of factors, including regulatory requirements. If construction, regulatory evaluation, and/or approval of our new facilities is delayed, we may not be able to manufacture sufficient quantities of our drug candidates, if approved, which would limit our development and commercialization activities and our opportunities for growth. Cost overruns associated with constructing or maintaining our facilities could require us to raise additional funds from other sources, which may not be available on favorable terms or at all.
Much of the equipment used in our manufacturing process was developed and built by us, and it would be difficult or even impossible to purchase or create suitable replacements in a short period of time. Further, for much of this equipment we have an insufficient amount of or no spare parts available. Were certain equipment, some of which is critical to the production of our drug candidates, to become damaged, lost, or otherwise unusable, we would have to construct new parts, which could take a considerable amount of time, causing a temporary halt to at least a portion of our production operations. Additionally, we are constantly seeking to further fine-tune and develop our advanced manufacturing techniques and process controls to fully utilize our facilities. Advances in manufacturing techniques may render our facilities and equipment inadequate, in which case we may lose any competitive advantage.
To produce our drug candidates in the quantities that we believe will be required to meet anticipated market demand, if approved, we will need to increase or “scale up” the production process by a significant factor over current levels of production. A significant part of the scaling up process will include seeking ways to increase the automation and semi-automation of our production process, which will require additional research and development, investment, potential new regulatory approvals, and cooperation with third parties, some of which may not be successful. If we are unable or are delayed in scaling up, or if the cost of doing so is not economically feasible for us, we may not be able to produce our approved drug candidates in a sufficient quantity to meet any future demand.
Delays in completing and receiving regulatory approvals for our manufacturing facilities could delay our development plans or commercialization efforts, which could harm our business.
Our manufacturing facilities will be subject to ongoing, periodic inspection by various regulatory authorities, including the FDA, EMA, China’s National Medical Products Administration (“NMPA”), Health Canada, and the Australian Therapeutics Goods Administration (“TGA”) or other comparable regulatory agencies to ensure compliance with GMP. Our failure to follow and document our adherence to such GMP or other regulatory requirements may lead to significant delays in the availability of products for clinical or, if approved, commercial use, and may result in the termination of or a hold on a clinical trial, or may delay or prevent filing or approval of marketing applications for our drug candidates or the commercialization of our drugs, if approved. We also may encounter problems with the following:
| ● |
achieving adequate or clinical-grade materials that meet FDA, EMA, NMPA, Health Canada, TGA or other comparable regulatory agency standards or specifications with consistent and acceptable production yield and costs; |
| ● |
shortages of qualified personnel, raw materials or key contractors; and |
| ● |
ongoing compliance with GMP and other requirements of the FDA, EMA, NMPA, Health Canada, TGA or other comparable regulatory agencies. |
Failure to comply with applicable regulations could also result in sanctions being imposed on us, including fines, injunctions, civil penalties, a requirement to suspend or put on hold one or more of our clinical trials, failure of regulatory authorities to grant marketing approval of our drug candidates, delays, suspension or withdrawal of approvals, supply disruptions, license revocation, seizures, or recalls of our drug candidates, operating restrictions and civil or criminal prosecutions, any of which could harm our business.
Damage to, destruction of, or interruption of production at our manufacturing facilities would negatively affect our business and prospects.
If our manufacturing facilities or the equipment in them is damaged or destroyed, we may not be able to quickly or inexpensively replace our manufacturing capacity or replace it at all. In the event of a temporary or protracted loss of the facilities or equipment, we might not be able to transfer manufacturing to a third party. Even if we could transfer manufacturing to a third party, the shift would likely be expensive and time-consuming, particularly since the new facility would need to comply with the necessary regulatory requirements and we would need regulatory agency approval before selling any of our drugs, if approved, manufactured at that new facility. Such an event could delay our clinical trials or reduce our product sales if any of our drug candidates are approved and successfully commercialized. Any interruption in manufacturing operations at our manufacturing facilities could result in our inability to satisfy the demands of our clinical trials or commercialization. Any disruption that impedes our ability to manufacture our drug candidates in a timely manner could materially harm our business, financial condition, results of operations, and prospects.
Currently, we maintain insurance coverage against damage to our property and equipment in amounts we believe are reasonable. However, our insurance coverage may not reimburse us, or may not be sufficient to reimburse us, for any expenses or losses we may suffer. We may be unable to meet the requirements for our drug candidates if there were a catastrophic event or failure of our manufacturing facilities or processes.
Significant or sustained inflation could adversely affect our business, financial condition and results of operations.
Inflation can adversely affect us by increasing our costs, including salary costs. Significant inflation is often accompanied by higher interest rates. Any sustained inflation or significant increases in inflation and interest rates could have a material adverse effect on our business, financial condition and results of operations. Increases in interest rates may also adversely affect the repayment terms of certain of our debt agreements.
Our future success depends on our ability to retain key executives and to attract, train, retain, develop, and motivate qualified and highly skilled personnel.
We are highly dependent on Mark Mortenson, our co-founder and Chief Science Officer, Rob Etherington, our Chief Executive Officer and President, and the other principal members of our management and scientific teams. We do not maintain “key person” insurance for any of our executives or other employees. The loss of the services of any of our executive officers, other key employees, and other scientific advisors, and our inability to find suitable replacements could result in delays in product development and harm our business.
Recruiting, retaining, and developing qualified scientific, technical, clinical, manufacturing, sales, and marketing personnel in the future will also be critical to our success. In addition, we rely on third-party consultants and advisors, including scientific and clinical advisors, to assist us in formulating our discovery, clinical development, operations, and commercialization strategy. The loss of the services of our executive officers or other key employees and consultants could impede the achievement of our research, development, and commercialization objectives and seriously harm our ability to successfully implement our business strategy.
We benefit from certain tax and financial incentives, the expiration of or changes to which could adversely affect our profitability.
We benefit from certain tax treatments, as well as tax concessions in relation to our research and development costs. We receive refundable tax credits through the research and development tax credits in the U.S., Australia, and the state of Maryland. In the U.S., the research and development tax credit is used to offset federal employment taxes on our U.S. payroll. In Australia, we receive a refundable tax offset of eligible research and development activities equal to our corporate tax rate plus 18%. In Maryland, we receive the Basic Research and Development Tax credit, which is used to offset state income taxes and may be applied against following years’ taxes until the credit is used or the credit may be carried forward for seven years. We also receive a tax exemption in Maryland for state personal property and sales tax, as well certain tax credits.
In addition, current or future tax treatments, tax concessions, tax allowances and financial incentives applicable to us may be changed, terminated, or otherwise become unavailable due to many factors, including changes in government policy or administrative decisions by the relevant government authorities. Due to potential changes in government policies, we cannot be certain of the level of government grants we will receive in the future. Our post-tax profitability and cash flows may be adversely affected as a result of one or more of these or other factors.
Our ability to use net operating losses to offset future taxable income may be subject to certain limitations.
We have incurred substantial losses since inception and do not expect to become profitable in the near future, if ever. To the extent that we continue to generate taxable losses, unused losses will carry forward to offset future taxable income, if any. As of December 31, 2023, we had U.S. federal net operating loss (“NOL”) carryforwards of $147.1 million, of which $113.7 million may be carried forward indefinitely to reduce future taxable income but utilization is limited to 80% of our annual taxable income in any given year based on current federal tax laws. The remaining balance of $33.4 million will begin to expire after 2034. As of December 31, 2023, we had state NOL carryforwards of $96.7 million, of which $83.7 million may be carried forward indefinitely to reduce future taxable income but utilization is limited to 80% of our taxable income in any given tax year based on current tax laws. The remaining balance of $12.9 million will begin to expire after 2032. As of December 31, 2023, we had research and development tax credit carryforwards of $5.6 million, which may be available to reduce future tax liabilities and expire at various dates beginning after 2032.
Under U.S. federal tax legislation commonly referred to as the Tax Cuts and Jobs Act (“TCJA”), as modified by the Coronavirus Aid, Relief and Economic Security Act, or the CARES Act, U.S. federal NOLs incurred in taxable years beginning after December 31, 2017 and in future taxable years may carry forward indefinitely, but the deductibility of such U.S. federal NOLs incurred in taxable years beginning after December 31, 2020 are limited. It is uncertain how various states will respond to the TCJA and CARES Act. In addition, under Section 382 of the Internal Revenue Code of 1986, as amended, and corresponding provisions of state law, if a corporation undergoes an “ownership change,” which is generally defined as a greater than 50% change, by value, in its equity ownership over a three-year period, the corporation’s ability to use its pre-change NOL carryforwards and other pre-change tax attributes to offset its post-change income or taxes may be limited. Any future offerings of equity securities, together with other transactions that have occurred since our inception, may trigger such an ownership change pursuant to Section 382 of the Internal Revenue Code of 1986. We have not conducted a study to assess whether any such ownership changes have occurred. We may experience ownership changes as a result of subsequent shifts in our stock ownership, some of which may be outside of our control. If an ownership change occurs and our ability to use our NOL carryforwards is materially limited, it would harm our financial condition and results of operations by effectively increasing our future tax obligations.
Changes in tax laws may adversely affect us, and the Internal Revenue Service or a court may disagree with tax positions taken by us, which may result in adverse effects in our financial condition or the value of our Common Stock.
The TCJA, enacted on December 22, 2017, significantly affected U.S. tax law, including by changing how the U.S. imposes tax on certain types of income of corporations and by reducing the U.S. federal corporate income tax rate to 21%. It also imposed new limitations on a number of tax benefits, including deductions or business interest, use of net operating loss carry forwards, taxation of foreign income and the foreign tax credit, among others.
The CARES Act, enacted on March 27, 2020, in response to the COVID-19 pandemic, further amended the Internal Revenue Code of 1986, including in respect of certain changes that were made by the TCJA, generally on a temporary basis. In addition, the Internal Revenue Service (“IRS”) has yet to issue guidance on a number of important issues regarding the changes made by the TCJA and the CARES Act. In the absence of such guidance, we will take positions with respect to a number of unsettled issues. There is no assurance that the IRS or a court will agree with the positions taken by us, in which case tax penalties and interest may be imposed that could adversely affect our business, cash flows or financial performance.
Additionally, the current administration may propose significant changes to U.S. tax law, some or all of which may be enacted. The passage of such legislation, as well as changes or modifications in existing judicial decisions or in the current positions of the IRS, could substantially modify the tax treatment described in this Annual Report, possibly on a retroactive basis. We cannot predict whether the U.S. Congress or any other legislative body will enact new tax legislation or whether the IRS or any other tax authority will issue new regulations or other guidance, nor can we predict what effect such legislation or regulations might have on us or our financial condition. There can be no assurance that future tax law changes will not increase the rate of the corporate income tax significantly, impose new limitations on deductions, credits or other tax benefits, or make other changes that may adversely affect our business, cash flows or financial performance.
Our business and operations have been affected by and could be materially and adversely affected in the future by the effects of health epidemics and pandemics, which could also cause material adverse effects on the business and operations of third parties on which we rely.
Our business and operations could be adversely affected by health epidemics and pandemics. We, our CROs, clinical investigators, third-party vendors and clinical sites, and other suppliers may experience disruptions in supply of drug candidates and/or procuring items that are essential for our research and development activities, including raw materials used in the manufacturing of our drug candidates, medical and laboratory supplies used in our clinical trials or preclinical studies or animals that are used for preclinical testing, in each case, for which there may be shortages due to future epidemics and pandemics. Any disruption in the supply chain from any potential future epidemics and pandemics could have a material adverse effect on our clinical trial plans and business operations.
We and our third-party CROs have faced disruptions that affected our ability to initiate and complete preclinical studies, caused manufacturing disruptions, and created delays at clinical trial site initiation and clinical trial enrollment, which ultimately led to the early conclusion of a clinical trial. Even if clinical trial sites are actively recruiting, we may face difficulties recruiting or retaining patients in our ongoing and planned clinical trials if patients are affected by or are fearful of visiting or traveling to clinical trial sites because of any potential future epidemics and pandemics. Prolonged delays or closure to enrollment in our trials or patient discontinuations could have a material adverse impact on our clinical trial plans and timelines. Any negative impact from health epidemics or pandemics on the ability of clinical trial sites to recruit or retain patients or collect patient data could cause costly delays to clinical trial activities, which could adversely affect our ability to obtain regulatory approval for and, if approved, to commercialize our drug candidates, increase our operating expenses, and have a material adverse effect on our financial results.
The response to health epidemics and pandemics may redirect our resources with respect to regulatory and intellectual property matters in a way that would adversely affect our ability to obtain regulatory approvals and protect our intellectual property. In addition, we may face impediments to regulatory meetings and approvals due to measures intended to limit in-person interactions.
Health epidemics and pandemics may materially and adversely affect us economically. While the potential global economic impact brought by, and the duration of, health epidemics and pandemics may be difficult to assess or predict, they have caused and could cause future disruption in the global financial markets. This disruption, if sustained or recurrent, could make it more difficult for us to access capital, which could negatively affect our liquidity in the future.
The ultimate impact of potential future epidemics or pandemics is highly uncertain and subject to continued change. These effects could have a material impact on our business and operations, or the businesses and operations of third parties on which we rely.
We have identified material weaknesses in our internal control over financial reporting. If we fail to remediate these material weaknesses, or if we experience additional material weaknesses in the future or otherwise fail to maintain an effective system of internal controls, we may not be able to accurately or timely report our financial condition or results of operations, which may adversely affect investor confidence in us and, as a result, the value of our Common Stock.
Effective internal control over financial reporting is necessary for us to provide reliable financial reports and, together with adequate disclosure controls and procedures, is designed to prevent fraud. Any failure to implement required new or improved controls, or difficulties encountered in their implementation, could cause us to fail to meet our reporting obligations. In addition, any testing by us, as and when required, conducted in connection with Section 404 of the Sarbanes-Oxley Act or any subsequent testing by our independent registered public accounting firm, as and when required, may reveal deficiencies in our internal control over financial reporting that are deemed to be significant deficiencies or material weaknesses or that may require prospective or retroactive changes to our financial statements or identify other areas for further attention or improvement. Inferior internal controls could also cause investors to lose confidence in our reported financial information, which could have a negative effect on the trading price of our Common Stock.
In connection with the audit of our financial statements as of and for the years ended December 31, 2023 and 2022, our management identified material weaknesses in our internal control over financial reporting. A material weakness is a deficiency, or combination of deficiencies, in internal control over financial reporting, such that there is a reasonable possibility that a material misstatement of our annual or interim financial statements will not be prevented or detected on a timely basis. The material weaknesses identified relate to the fact that we did not design or maintain an effective control environment commensurate with our financial reporting requirements. This deficiency in our control environment contributed to the following additional material weaknesses related to control activities and information and communication within our internal control over financial reporting:
| ● |
we did not design and maintain controls over the preparation and review of account reconciliations and the review and segregation of duties over manual journal entries, including controls over the completeness and accuracy of information; and |
| ● |
we did not design and maintain information technology (“IT”) general controls for IT systems that are relevant to the preparation of the financial statements. Specifically, we did not design and maintain: (a) user access controls to ensure appropriate segregation of duties and that adequately restrict user and privileged access to financial applications, programs, and data to our appropriate personnel; (b) program change management controls to ensure that IT program and data changes affecting financial IT applications and underlying accounting records are identified, tested, authorized, and implemented appropriately; (c) computer operations controls to ensure that data backups are authorized and monitored; and (d) testing and approval controls for program development to ensure that new software development is aligned with business and IT requirements. |
Each of the control deficiencies described above could result in a misstatement of one or more account balances or disclosures that would result in a material misstatement to the annual or interim consolidated financial statements that would not be prevented or detected. Accordingly, our management has determined that each of the control deficiencies described above constitute material weaknesses.
Although we have begun to implement measures to address the material weaknesses, the implementation of these measures may not fully address the material weaknesses and deficiencies in our internal control over financial reporting, and we cannot conclude that these matters have been fully remedied. As we continue to evaluate, and work to improve, our internal control over financial reporting, management may determine that additional or different measures to address control deficiencies or modifications to the remediation plan are necessary. Further, in the future we may determine that we have additional material weaknesses. Our failure to remediate the material weaknesses or failure to identify and address any other material weaknesses or control deficiencies could result in inaccuracies in our financial statements and could also impair our ability to comply with applicable financial reporting requirements and related regulatory filings on a timely basis, which could cause investors to lose confidence in our reported financial information, which may result in volatility in and a decline in the market price of our Common Stock.
Pursuant to Section 404, after the Reverse Recapitalization, we, as the surviving entity, are required to furnish a report by our management on the effectiveness of our internal control over financial reporting, including an attestation report on internal control over financial reporting issued by our independent registered public accounting firm. However, while we remain a smaller reporting company, we will not be required to include an attestation report on internal control over financial reporting issued by our independent registered public accounting firm. To achieve compliance with Section 404 within the prescribed period, we will be engaged in a process to document and evaluate our internal control over financial reporting, which is both costly and challenging. In this regard, we will need to continue to dedicate internal resources, potentially engage outside consultants and adopt a detailed work plan to assess and document the adequacy of internal control over financial reporting, continue steps to improve control processes as appropriate, validate through testing that controls are functioning as documented and implement a continuous reporting and improvement process for internal control over financial reporting. Despite our efforts, there is a risk that neither we nor our independent registered public accounting firm, if and when required, will be able to conclude within the prescribed timeframe that our internal control over financial reporting is effective as required by Section 404. This could adversely affect investor confidence in us and, as a result, the value of our Common Stock.
There is significant uncertainty associated with our drug candidates and their viability as a commercial product.
Metallic nanocrystal therapeutic candidates, such as our lead drug candidate, CNM-Au8, are considered emerging and novel investigational products for the potential treatment of neurological diseases and other disorders. We are developing CNM-Au8 for the treatment of neurological disorders such as ALS, MS, and PD through remyelination and/or neuroprotection mechanisms related to catalysis of certain biological reactions. There are currently no approved remyelination therapies and the evidence for an effect of neuroprotection treatments on these indications is thus far limited. Since there is limited clinical trial data and precedent for the development of nanocrystal therapies that promote remyelination and neuroprotection to treat these indications, there is a substantial risk that the design or outcomes of our clinical trials will not be satisfactory to support regulatory approval. In addition, there are generally limited or no regulatory precedents concerning metallic nanocrystal drug marketing authorization, or a regulatory framework to appropriately differentiate approved nanocrystal product labeling. Our lead metallic nanocrystal drug candidate, CNM-Au8, contains nanocrystals made entirely of high purity gold alone. It is unclear how regulatory authorities will identify or classify the active moiety of CNM-Au8, including whether it is classified as a new chemical entity or comparable designation. The inability to obtain sufficiently differentiated active moiety classification from gold generically could potentially limit CNM-Au8 and our drug candidates from ever achieving profitability.
Moreover, the mechanisms of action for nanocrystal therapies are not thoroughly understood, and adverse events or side effects may be observed in clinical trials and reported by medical practitioners in connection with patient usage in the future. If those adverse events or side effects prove significant, they may hamper the ability of our drug candidates to pass through clinical trials or they may outweigh the benefits that patients derive from using our drug candidates, both of which could potentially prevent our drug candidates from ever achieving profitability.
Our drug candidates are not metabolized and may accumulate in the body following long-term usage, making the long-term effects of taking our drug candidates for substantial periods of time uncertain. While all of the current toxicology studies of our drug candidates have resulted in no-adverse-effect levels as of the date of this Annual Report, we have not completed reproductive or carcinogenicity studies, which we are required to complete in the future. Any negative results from these studies could materially and adversely affect our business, results of operations, financial condition, and prospects.
Moreover, the results of clinical trials for nanocrystal therapies could reveal a high and unacceptable severity and prevalence of undesirable side effects. Any such side effects could adversely impact our ability to obtain regulatory approvals. For example, the FDA, NMPA, Health Canada, TGA, EMA or other comparable authorities could order us to suspend or terminate our studies or to cease further clinical development of or deny approval of our drug candidates. In addition, any adverse drug-related side effects could affect patient recruitment or the ability of enrolled patients to complete trials or may result in potential product liability claims. Any of these occurrences may harm our business, financial condition, results of operations, and prospects significantly.
We have not previously obtained any regulatory approval for a drug candidate and we may be unable to obtain or may be delayed in obtaining regulatory approval for any of our drug candidates.
Our business is substantially dependent on our ability to complete the development of, obtain regulatory approval for and successfully commercialize drug candidates in a timely manner. We cannot commercialize drug candidates without obtaining regulatory approval to market each drug from the FDA, NMPA, Health Canada, TGA, EMA and other comparable regulatory authorities. The time required to obtain approval from regulatory authorities is unpredictable but typically takes years following the commencement of preclinical studies and clinical trials and depends upon numerous factors, including the substantial discretion of the regulatory authorities. In addition, approval policies, regulations or the type and amount of clinical data necessary to gain approval may change during the course of a drug candidate’s clinical development and may vary among jurisdictions.
Our drug candidates could fail to receive regulatory approval for many reasons, including:
| ● |
failure to begin or complete clinical trials due to disagreements with regulatory authorities; |
| ● |
failure to begin or complete clinical trials due to inability to recruit sufficient numbers of study participants; |
| ● |
failure to demonstrate that a drug candidate is safe and effective or is safe, pure and potent for our proposed indication; |
| ● |
failure of clinical trial results to meet the level of statistical significance required for approval; |
| ● |
data integrity issues related to our clinical trials; |
| ● |
disagreement with our interpretation of data from preclinical studies or clinical trials; |
| ● |
changes in approval policies or regulations that render our preclinical and clinical data insufficient for approval or require us to amend our clinical trial protocols; |
| ● |
regulatory requests for additional analysis, reports, data, nonclinical studies and clinical trials, or questions regarding interpretations of data and results and the emergence of new information regarding our drug candidates; |
| ● |
insufficient data from the clinical trials of our drug candidates to obtain regulatory approval; |
| ● |
failure by us or our investigators to conduct a clinical trial in accordance with regulatory requirements or our clinical trial protocols; and |
| ● |
clinical sites, investigators or other participants in our clinical trials deviating from a trial protocol, failing to conduct the trial in accordance with regulatory requirements, or dropping out of a trial. |
The FDA, NMPA, TGA, Health Canada, EMA or a comparable regulatory authority may require more information, including additional preclinical or clinical data, to support approval, which may delay or prevent approval and our commercialization plans, or we may decide to abandon the development program.
New or unexpected adverse events, or changes in regulatory requirements and guidance may also occur, and we may need to amend clinical trial protocols submitted to applicable regulatory authorities to reflect these changes. Amendments may require us to resubmit clinical trial protocols to IRBs or HRECs for re-examination, which may impact the costs, timing or successful completion of a clinical trial.
If we experience delays in the completion of, or the termination of, a clinical trial of any of our drug candidates, the commercial prospects of that drug candidate will be harmed, and our ability to generate product sales revenues from any of those drug candidates will be delayed. In addition, any delays in completing our clinical trials will increase our costs, slow down our drug candidate development and approval process, and jeopardize our ability to commence product sales and generate related revenues for that product. Any of these occurrences may harm our business, financial condition, results of operations, and prospects significantly. In addition, many of the factors that cause, or lead to, a delay in the commencement or completion of clinical trials may also ultimately lead to the denial of regulatory approval of our drug candidates.
We may not be able to successfully identify, discover, or develop new drug candidates.
We cannot guarantee that we will be successful in identifying potential drug candidates for clinical development for a number of reasons. For example, our research methodology may be unsuccessful in identifying potential drug candidates or those we identify may be shown to have harmful side effects or other characteristics that make them unmarketable or unlikely to receive regulatory approval. We have devoted significant resources to discovery efforts through our proprietary electro-crystal-chemistry drug development platform, however, we cannot guarantee that we will be successful in identifying additional potential drug candidates.
Research programs to pursue the development of our drug candidates for additional indications and to identify new drug candidates and drug targets require substantial technical, financial, and human resources. Our research programs may initially show promise in identifying potential indications and/or drug candidates, yet fail to yield results for clinical development for a number of reasons, including:
| ● |
the research methodology used may not be successful in identifying potential indications, and/or drug candidates; |
| ● |
potential drug candidates may, after further study, be shown to have harmful adverse effects or other characteristics that indicate they are unlikely to be effective drugs; or |
| ● |
it may take greater human and financial resources to identify additional therapeutic opportunities for our drug candidates or to develop suitable potential drug candidates through internal research programs than we will possess, thereby limiting our ability to diversify and expand our drug portfolio. |
Accordingly, there is no assurance that we will ever be able to identify additional therapeutic opportunities for our drug candidates or to develop suitable potential drug candidates through internal research programs, which could materially and adversely affect our future growth, business, financial condition, results of operations, and prospects. We may focus our efforts and resources on potential drug candidates or other potential programs that ultimately prove to be unsuccessful.
Preclinical and clinical development of drug candidates involves a lengthy and expensive process with an uncertain outcome, and we are unable to predict if or when we will successfully develop or commercialize any of our drug candidates.
There is a risk of failure for each of our drug candidates. Before obtaining regulatory approval for the sale of any of our drug candidates, we must complete preclinical studies and then conduct extensive clinical trials to demonstrate the safety and efficacy of our drug candidates in humans. It is difficult to predict when or if any of our drug candidates will prove effective and safe in humans or receive regulatory approval. Our internal discovery programs for some of our drug candidates are at an early stage of development and will require significant investment and regulatory approvals prior to commercialization. We are not permitted to market or promote any of our drug candidates until we receive regulatory approval from the FDA, NMPA, TGA, Health Canada, EMA or comparable regulatory authorities, and we may never receive such regulatory approval for any of our drug candidates.
We could encounter regulatory delays if a clinical trial is suspended or terminated by us or, as applicable, by the IRBs or the ethics committees of the institutions in which such trials are being conducted, by the DSMB, which is an independent group of experts that is formed to monitor clinical trials while ongoing, or by the FDA, NMPA, TGA, Health Canada, EMA or other regulatory authorities. Such authorities may impose a suspension or termination due to a number of factors, including: (1) a failure to conduct the clinical trial in accordance with regulatory requirements or the applicable clinical protocols, (2) inspection of the clinical trial operations or trial site by the FDA, NMPA, TGA, Health Canada, EMA or other regulatory authorities that results in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, (3) failure to demonstrate a benefit from using a drug, (4) changes in governmental regulations or administrative actions, or (5) lack of adequate funding to continue the clinical trial. Many of the factors that cause a delay in the commencement or completion of clinical trials may also ultimately lead to the denial of regulatory approval of our drug candidates. Further, the FDA, NMPA, TGA, Health Canada, EMA or other regulatory authorities may disagree with our clinical trial design or our interpretation of data from clinical trials, or may change the requirements for approval even after any regulatory authority has reviewed and commented on the design for our clinical trials.
Preclinical studies and clinical trials are expensive, difficult to design and implement, and can take many years to complete. Moreover, preclinical and clinical data are often susceptible to varying interpretations and analysis, and many companies that have believed their drug candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain regulatory approval of their drug candidates. Future clinical trials of our drug candidates may not be successful.
Commencement of clinical trials is subject to finalizing the trial design based on ongoing discussions with the FDA, NMPA, TGA, Health Canada, EMA and/or other regulatory authorities. The FDA, NMPA, TGA, Health Canada, EMA and other regulatory authorities could change their position on the acceptability of trial designs or clinical endpoints, which could require us to complete additional clinical trials or impose approval conditions that we do not currently expect. Successful completion of our clinical trials is a prerequisite to submitting an NDA (or analogous filing) to the FDA, NMPA, TGA, Health Canada, EMA and/or other regulatory authorities for each drug candidate and, consequently, the ultimate approval and commercial marketing of our drug candidates. We do not know whether the clinical trials for our drug candidates will be completed on schedule, if at all.
Results of earlier clinical trials may not be predictive of results of later-stage clinical trials.
The results of preclinical studies and early clinical trials of our drug candidates may not be predictive of the results of later-stage clinical trials. Drug candidates in later stages of clinical trials may fail to show the desired safety and efficacy traits despite having progressed through preclinical studies and initial clinical trials. Future clinical trial results may not be favorable for these and other reasons.
In some cases, there can be significant variability in the safety and/or efficacy results between different trials of the same drug candidate due to numerous factors, including changes in trial procedures set forth in protocols, differences in the size and type of the patient populations, including genetic differences, patient adherence to the dosing regimen, and the rate of dropout among clinical trial participants. As drug candidates are developed through preclinical to early- to late-stage clinical trials towards approval and commercialization, it is customary that various aspects of the development program, such as manufacturing and formulation, are altered along the way in an effort to optimize processes and results. Such changes carry the risk that they will not achieve these intended objectives. In the case of any trials we conduct, results may differ from earlier trials due to the larger number of clinical trial sites and additional countries and languages involved in such trials. Any of these changes could make the results of planned clinical trials or other future clinical trials we may initiate less predictable and could cause our drug candidates to perform differently, which could delay completion of clinical trials, delay approval of our drug candidates, and/or jeopardize our ability to commence commercialization of our drug candidates.
Clinical trials of our drug candidates may fail to demonstrate safety and efficacy to the satisfaction of regulatory authorities, or may not otherwise produce positive results, which may cause us to incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of our drug candidates.
Before obtaining regulatory approval for the sale of our drug candidates, we must conduct extensive clinical trials to demonstrate the safety and efficacy of our drug candidates in humans. We may experience numerous unexpected events during, or as a result of, clinical trials that could delay or prevent us from receiving regulatory approval or commercializing our drug candidates, including:
| ● |
regulators, IRBs, or HRECs may not authorize us or our investigators to commence a clinical trial or conduct a clinical trial at a prospective trial site; |
| ● |
our inability to reach agreements on acceptable terms with prospective CROs, clinical trial vendors, and trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; |
| ● |
manufacturing issues, including problems with manufacturing, supply quality, compliance with GMP, or obtaining from third parties sufficient quantities of a drug candidate for use in a clinical trial; |
| ● |
clinical trials of our drug candidates may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical trials or abandon drug development programs; |
| ● |
the number of patients required for clinical trials of our drug candidates may be larger than we anticipate; |
| ● |
our third-party contractors, including clinical investigators, may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all; |
| ● |
we may not investigate, may not be able to license, or may be unable to properly conduct companion diagnostic tests to identify patients who are likely to benefit from treatment with our drug candidates; |
| ● |
we might have to suspend or terminate clinical trials of our drug candidates for various reasons, including a finding of a lack of clinical response or other unexpected characteristics or a finding that participants are being exposed to unacceptable health risks; |
| ● |
regulators, IRBs or HRECs may require that we or our investigators suspend or terminate clinical research or not rely on the results of clinical research for various reasons, including non-compliance with regulatory requirements; |
| ● |
the cost of clinical trials of our drug candidates may be greater than we anticipate; |
| ● |
the supply or quality of our drug candidates or other materials necessary to conduct clinical trials of our drug candidates may be insufficient or inadequate; and |
| ● |
our drug candidates may have undesirable side effects or unexpected characteristics, causing us or our investigators, regulators, IRBs or ethics committees to suspend or terminate the clinical trials, or reports may arise from preclinical studies or clinical trials of other therapies that raise safety or efficacy concerns about our drug candidates. |
If we are required to conduct additional clinical trials or other testing of our drug candidates beyond those that we currently contemplate, if we are unable to successfully complete clinical trials of our drug candidates or other testing, if the results of these trials or tests are not positive or are only modestly positive or if they raise safety concerns, we may (i) be delayed in obtaining regulatory approval for our drug candidates; (ii) not obtain regulatory approval at all; (iii) obtain approval for indications that are not as broad as intended; (iv) have the drug removed from the market after obtaining regulatory approval; (v) be subject to additional post-market testing requirements; (vi) be subject to restrictions on how the drug is distributed or used; or (vii) be unable to obtain reimbursement for use of the drug.
Significant clinical trial delays may also increase our development costs and could shorten any periods during which we have the exclusive right to commercialize our drug candidates or allow our competitors to bring drugs to market before we do. This could impair our ability to commercialize our drug candidates and may harm our business and results of operations.
If we encounter difficulties enrolling patients in clinical trials, clinical trials of our drug candidates may be delayed or otherwise adversely affected.
The timely completion of clinical trials in accordance with their protocols depends, among other things, on our ability to enroll a sufficient number of patients who remain in the trial until our conclusion. We may experience difficulties in patient enrollment in our clinical trials for a variety of reasons, including:
| ● |
any future health epidemics or pandemics; |
| ● |
the size and nature of the patient population; |
| ● |
the design of the trial, including the patient eligibility criteria defined in the protocol; |
| ● |
the size of the study population required for analysis of the trial’s primary endpoints; |
| ● |
the proximity of patients to trial sites; |
| ● |
our ability to recruit clinical trial investigators with the appropriate competencies and experience; |
| ● |
competing clinical trials for similar therapies or other new therapeutics; |
| ● |
clinicians’ and patients’ perceptions as to the potential advantages and side effects of the drug candidate being studied in relation to other available therapies, including any new drugs or treatments that may be approved for the indications we are investigating; |
| ● |
our ability to obtain and maintain patient consents; |
| ● |
the risk that patients enrolled in clinical trials will not complete a clinical trial; and |
| ● |
the availability of approved therapies that are similar in mechanism to our drug candidates. |
Failure of our timely completion of clinical trials would delay the approval and commercialization of our drug candidates, impair the commercial performance of our drug candidates, and consequently harm our business and results of operations.
If we are not able to obtain, or experiences delays in obtaining, required regulatory approvals, we will not be able to commercialize our drug candidates, and our ability to generate revenue will be materially impaired.
Before obtaining regulatory approvals for the commercial sale of any drug candidate for a target indication, we must demonstrate in preclinical studies and well-controlled clinical trials, and, with respect to approval in the U.S., to the satisfaction of the FDA, that the drug candidate is safe and effective for use for that target indication and that the manufacturing facilities, processes and controls are adequate. In addition to preclinical and clinical data, the NDA must include significant information regarding the CMC for the drug candidate. Obtaining approval of an NDA is a lengthy, expensive and uncertain process, and approval may not be obtained. After we submit an NDA to the FDA, the FDA decides whether to accept or reject the submission for filing. We cannot be certain that any submissions will be accepted for filing and review by the FDA.
We have not yet demonstrated an ability to file for or receive regulatory approval for our drug candidates. For example, we do not have experience in preparing the required materials for regulatory submission or navigating the regulatory approval process. As a result, our ability to successfully submit an NDA and obtain regulatory approval for our drug candidates may involve more inherent risk, take longer, and cost more than it would if we were a company with experience in obtaining regulatory approvals.
Regulatory authorities outside of the U.S., such as the NMPA, TGA, Health Canada and EMA, also have requirements for approval of drugs for commercial sale with which we must comply prior to marketing in those areas. Regulatory requirements can vary widely from country to country and could delay or prevent the introduction of our drug candidates. Clinical trials conducted in one country may not be accepted by regulatory authorities in other countries, and obtaining regulatory approval in one country does not mean that regulatory approval will be obtained in any other country. Approval processes vary among countries and can involve additional product testing and validation, and additional administrative review periods. Seeking non-U.S. regulatory approval could require additional nonclinical studies or clinical trials, which could be costly and time consuming. The non-U.S. regulatory approval process may include all of the risks associated with obtaining FDA approval. For all of these reasons, we may not obtain non-U.S. regulatory approvals on a timely basis, if at all.
The process to develop, obtain regulatory approval for and commercialize drug candidates is long, complex and costly both inside and outside the U.S., and approval is never guaranteed. Even if our drug candidates were to successfully obtain approval from the regulatory authorities, any approval might significantly limit the approved indications for use, or require that precautions, contraindications or warnings be included on the product labeling, or require expensive and time-consuming post-approval clinical trials or surveillance as conditions of approval. Following any approval for commercial sale of our drug candidates, certain changes to the drug, such as changes in manufacturing processes and additional labeling claims, may be subject to additional review and approval by the FDA, NMPA, TGA, Health Canada, EMA and comparable regulatory authorities. Also, regulatory approval for any of our drug candidates may be withdrawn. If we are unable to obtain regulatory approval for our drug candidates in one or more jurisdictions, or any approval contains significant limitations, our target market will be reduced and our ability to realize the full market potential of our drug candidates will be harmed. Furthermore, we may not be able to obtain sufficient funding or generate sufficient revenue and cash flows to continue the development of any other drug candidate in the future.
Disruptions to the normal functioning of the FDA and comparable foreign regulatory authorities and other government agencies could hinder their ability to perform and carry out important roles and activities on which the operation of our business relies, which could negatively impact our business.
The ability of the FDA, NMPA, TGA, Health Canada, and EMA to review and approve new products can be affected by a variety of factors, including government budget and funding levels, ability to hire and retain key personnel and accept the payment of user fees, and statutory, regulatory, and policy changes. Average review times at the FDA have fluctuated in recent years as a result, which may continue in the future. In addition, government funding of other government agencies that fund research and development activities is subject to the political process, which is inherently fluid and unpredictable.
Disruptions at the FDA and other government agencies may slow the time necessary for new product candidates to be reviewed and/or approved by necessary government agencies, which would adversely affect our business. If a prolonged government shutdown occurs, it could significantly impact the ability of the FDA to timely review and process our regulatory submissions, which could have a material adverse effect on our business. Further, future government shutdowns could impact our ability to access the public markets and obtain necessary capital in order to properly capitalize and continue our operations.
Since March 2020, when foreign and domestic inspections of facilities were largely placed on hold, the FDA has been working to resume pre-COVID-19 pandemic levels of inspection activities, including routine surveillance, bioresearch monitoring and pre-approval inspections. Should the FDA determine that an inspection is necessary for approval and an inspection cannot be completed during the review cycle due to restrictions on travel, and the FDA does not determine a remote interactive evaluation to be adequate, the FDA has stated that it generally intends to issue, depending on the circumstances, a complete response letter or defer action on the application until an inspection can be completed. During the COVID-19 pandemic, a number of companies announced receipt of complete response letters due to the FDA’s inability to complete required inspections for their applications. Regulatory authorities outside the U.S. may adopt similar restrictions or other policy measures in response to future health epidemics or pandemics and may experience delays in their regulatory activities.
Favorable designations may not be granted, or if granted, may be withdrawn later, for any of our drug candidates, and may not lead to faster development or regulatory review or approval.
We do not currently have Fast Track Designation or Breakthrough Therapy Designation, but may seek one or more of such designations in the future.
If a drug is intended for the treatment of a serious or life-threatening condition and the drug demonstrates the potential to address unmet medical need for that condition, the drug sponsor may apply for FDA Fast Track Designation. The FDA has broad discretion in deciding whether or not to grant this designation. Even if we believe a particular drug candidate is eligible for this designation, we cannot assure that the FDA would decide to grant it. Even if we do receive Fast Track Designation, we may not experience a development, review or approval process faster than conventional FDA procedures. The FDA may withdraw a Fast Track Designation if it believes that the designation is no longer supported by data from our clinical development program. Many drugs that have received Fast Track Designation have failed to obtain approval from the FDA.
A Breakthrough Therapy is defined as a drug that is intended, alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or condition, and preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. For drugs that have been designated as Breakthrough Therapies, interaction and communication between the FDA and the sponsor can help to identify the most efficient path for development.
Designation as a Breakthrough Therapy is within the discretion of the FDA. Accordingly, even if we believe, after completing early clinical trials, that one of our drug candidates meets the criteria for designation as a Breakthrough Therapy, the FDA may disagree and instead decide not to grant that designation. In any event, the receipt of a Breakthrough Therapy Designation for a drug candidate may not result in a faster development, review or approval process compared to drugs considered for approval under conventional FDA procedures and does not assure ultimate approval by the FDA. In addition, even if one or more of our drug candidates qualify as Breakthrough Therapies, the FDA may later decide that such drug candidates no longer meet the conditions for qualification.
Although we have obtained FDA orphan drug designation for CNM-Au8 for the treatment of ALS, we may not realize any benefit from such designation and it does not increase the chance of approval.
The FDA granted orphan drug designation to our lead drug candidate, CNM-Au8, for the treatment of ALS in May 2019. Regulatory authorities in some jurisdictions, including the U.S. and the European Union, may designate drugs for relatively small patient populations as orphan drugs. Under the Orphan Drug Act, the FDA may designate a drug as an orphan drug if it is a drug intended to treat a rare disease or condition, which is generally defined as a disease with a patient population of fewer than 200,000 individuals in the U.S., or that affects more than 200,000 individuals in the U.S. and for which there is no reasonable expectation that costs of research and development of the product for the indication can be recovered by sales of the product in the U.S. Generally, if a drug with an orphan drug designation subsequently receives the first regulatory approval for the indication for which it has such designation, the drug is entitled to a period of marketing exclusivity, which precludes the FDA or EMA, from approving another marketing application for the same drug for the same indication during the period of exclusivity. The applicable period is seven years in the U.S. and ten years in the European Union. The European exclusivity period can be reduced to six years if a drug no longer meets the criteria for orphan drug designation or if the drug is sufficiently profitable so that market exclusivity is no longer justified. Orphan drug exclusivity may be lost if the FDA or the EMA determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantity of the drug to meet the needs of patients with the rare disease or condition.
Although we have obtained orphan drug designation for CNM-Au8 for the treatment of ALS in the U.S., and may obtain the same designation for other drug candidates or indications, that designation may not effectively protect the drug candidate from competition, if approved, because different drugs can be approved for the same condition and the same drugs can be approved for a different condition but used off-label for any orphan indication we may obtain. Even after an orphan drug is approved, the FDA can subsequently approve a drug that is otherwise the same drug for the same condition if the FDA concludes that the later drug is clinically superior in that it is shown to be safer, more effective, or makes a major contribution to patient care.
Any of our drug candidates, if approved, would continue to be subject to ongoing or additional regulatory obligations and regulatory review, which may result in significant additional expense and we may be subject to penalties if we fail to comply with regulatory requirements or experience unanticipated problems with our drug candidates.
Any of our drug candidates, if approved, will be subject to ongoing or additional regulatory requirements for manufacturing, labeling, packaging, storage, advertising, promotion, sampling, record-keeping, conduct of post-market studies, and submission of safety, efficacy, and other post-market information, including both federal and state requirements in the U.S. and requirements of comparable regulatory authorities in the European Union, China, Australia and other markets.
Manufacturers and manufacturers’ facilities are required to comply with extensive FDA, NMPA, TGA, Health Canada, EMA and other comparable regulatory authority requirements ensuring that quality control and manufacturing procedures conform to GMP. As such, we will be subject to continual review and inspections to assess compliance with GMP and adherence to commitments made in any NDA, other marketing applications, and previous responses to any inspection observations if we were to build manufacturing facilities in the future. Accordingly, we and others with whom we work must continue to expend time, money and effort in all areas of regulatory compliance, including manufacturing, production, and quality control.
Any approvals that we receive for our drug candidates may be subject to limitations on the approved indicated uses for which the drug may be marketed or to the conditions of approval, which could adversely affect the drug’s commercial potential or contain requirements for potentially costly post-market testing and surveillance to monitor the safety and efficacy of the drug candidate. The FDA, NMPA, TGA, Health Canada, EMA or a comparable regulatory authority may also require a risk evaluation mitigation strategy program as a condition of approval of our drug candidates or following approval. In addition, if the FDA, NMPA, TGA, Health Canada, EMA or a comparable regulatory authority approves our drug candidates, we will have to comply with requirements, including, for example, submissions of safety and other post-market information and reports, registration, as well as continued compliance with GMP and GCP, for any clinical trials that we conduct post-approval.
The FDA and other regulatory authorities strictly regulate the marketing, labeling, advertising and promotion of products that are placed on the market. Drugs may be promoted only for their approved indications and for use in accordance with the provisions of the approved label. The FDA, NMPA, TGA, Health Canada, EMA and other regulatory authorities actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is found to have improperly promoted off-label uses may be subject to significant penalties and enforcement actions.
Even if we are able to commercialize any approved drug candidates, the drugs may become subject to national or other third-party reimbursement practices or unfavorable pricing regulations, which could harm our business.
The regulations that govern regulatory approvals, pricing and reimbursement for new therapeutic products vary widely from country to country. In Europe, Canada, Australia, China, and some markets outside China, prescription pharmaceutical pricing remains subject to continuing governmental control even after initial approval is granted. As a result, we might obtain regulatory approval for a drug in a particular country, but then be subject to price regulations that delay our commercial launch of the drug and negatively impact our revenues.
Our ability to commercialize any approved drug candidates successfully also will depend in part on the extent to which reimbursement for these drugs and related treatments will be available from government health administration authorities, private health insurers, and other organizations.
A primary trend in the global healthcare industry is cost containment. Government authorities and these third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications.
In the U.S., no uniform policy of coverage and reimbursement for drugs exists among third-party payors. As a result, obtaining coverage and reimbursement approval of a drug from a government or other third-party payor is a time-consuming and costly process that could require us to provide to each payor supporting scientific, clinical, and cost-effectiveness data for the use of our future approved drugs on a payor-by-payor basis, with no assurance that coverage and adequate reimbursement will be obtained. Even if we obtain coverage for a given drug, the resulting reimbursement rates might not be adequate for us to achieve or sustain profitability or may require co-payments that patients find unacceptably high. Additionally, third-party payors may not cover, or provide adequate reimbursement for, long-term follow-up evaluations required following the use of our future approved drug candidates. Patients are unlikely to use any of our future approved drugs unless coverage is provided and reimbursement is adequate to cover a significant portion of the cost of the drug. Because some of our drug candidates may have a higher cost of goods than conventional small molecule therapies, and may require long-term follow-up evaluations, the risk that coverage and reimbursement rates may be inadequate for us to achieve profitability may be greater.
Increasingly, third-party payors are requiring that companies provide them with predetermined discounts from list prices and are challenging the prices charged for medical products. We cannot assure that reimbursement will be available for any approved drug candidate that we commercialize and, if reimbursement is available, what the level of reimbursement will be. Reimbursement may impact the demand for, or the price of, any approved drug candidate that we commercialize. If reimbursement is not available or is available only to limited levels, we may not be able to successfully commercialize any drug candidate that we successfully develop.
There may be significant delays in obtaining reimbursement for approved drug candidates, and coverage may be more limited than the purposes for which the drug candidates are approved by the FDA, NMPA, TGA, Health Canada, EMA or other comparable regulatory authorities. Moreover, eligibility for reimbursement does not imply that any drug will be paid for in all cases or at a rate that covers our costs, including research, development, manufacture, sale and distribution. Interim payments for new drugs, if applicable, may also not be sufficient to cover our costs and may not be made permanent. Payment rates may vary according to the use of the drug and the clinical setting in which it is used, may be based on payments allowed for lower cost drugs that are already reimbursed, and may be incorporated into existing payments for other services. Net prices for drugs may be reduced by mandatory discounts or rebates required by government healthcare programs or private payors and by any future weakening of laws that presently restrict imports of drugs from countries where they may be sold at lower prices than in the U.S. Our inability to promptly obtain coverage and profitable payment rates from both government-funded and private payors for any future approved drug candidates and any new drugs that we develop could have a material adverse effect on our business, operating results and overall financial condition.
We intend to seek approval alone or in conjunction with partners to market our drug candidates in the U.S., China, the European Union, Australia, Canada, and other jurisdictions. In China, Australia, Canada, and the European Union, the pricing of drugs is subject to governmental control, and it can take considerable time after obtaining marketing regulatory approval to get the future approved drugs reimbursed. Market acceptance and sales of any of our future approved drug candidates will depend significantly on the availability of adequate coverage and reimbursement from third-party payors for drugs and may be affected by existing and future healthcare reform measures.
Our drug candidates, if approved in the future, may fail to achieve the degree of market acceptance by physicians, patients, third-party payors and others in the medical community necessary for commercial success and the market opportunity for the drug candidate may be smaller than we estimate.
Our drug candidates, if approved in the future, may fail to gain sufficient market acceptance by physicians, patients, third-party payors and others in the medical community. For example, current MS treatments are well established in the medical community, and physicians may continue to rely on these treatments to the exclusion of our drug candidates that are in clinical trials for the same or similar indications. In addition, physicians, patients, and third-party payors may prefer other novel products to ours. If our drug candidates do not achieve an adequate level of acceptance, we may not generate significant product sales revenues and we may not become profitable. The degree of market acceptance of our drug candidates, if approved for commercial sale, will depend on a number of factors, including:
| ● |
the clinical indications for which our drug candidates are approved; |
| ● |
whether physicians, hospitals, treatment centers and patients consider our drug candidates as a safe and effective treatment; |
| ● |
the potential and perceived advantages of our drug candidates over alternative treatments; |
| ● |
the prevalence and severity of any side effects; |
| ● |
product labeling or product insert requirements of regulatory authorities; |
| ● |
limitations or warnings contained in the labeling approved by regulatory authorities; |
| ● |
the timing of market introduction of our drug candidates as well as competitive drugs; |
| ● |
the cost of treatment in relation to alternative treatments; |
| ● |
the availability of adequate coverage, reimbursement and pricing by third-party payors and government authorities; |
| ● |
the willingness of patients to pay out-of-pocket in the absence of coverage and reimbursement by third-party payors and government authorities; and |
| ● |
the effectiveness of our sales and marketing efforts. |
If any approved drug candidates that we commercialize fail to achieve market acceptance among physicians, patients, hospitals, treatment centers or others in the medical community, we will not be able to generate significant revenue. Even if any future approved drug candidates achieve market acceptance, we may not be able to maintain that market acceptance over time if new products or technologies are introduced that are more favorably received than our drug candidates, are more cost-effective or render our drug candidates obsolete.
If our drug candidates cause, or are perceived to cause, undesirable side effects, it can result in delays or failure to receive regulatory approval or limitations on the commercial profile of an approved label.
Undesirable side effects caused by our drug candidates could cause either us or regulatory authorities to interrupt, delay or halt clinical trials and could result in a more restrictive label or the delay or denial of regulatory approval by the FDA, NMPA, TGA, Health Canada, EMA or other regulatory authorities. If the results of the ongoing clinical trials of our drug candidates reveal a high and unacceptable severity and prevalence of undesirable side effects, the clinical trials of our drug candidates could be suspended or terminated and the FDA, NMPA, TGA, Health Canada, EMA or comparable regulatory authorities could order us to cease further development of or deny approval of our drug candidates for any or all targeted indications. The drug-related side effects could affect patient recruitment or the ability of enrolled patients to complete the clinical trial or result in potential product liability claims. Any of these occurrences may harm our business, financial condition, and prospects significantly.
Clinical trials assess a sample of the potential patient population. With a limited number of patients and a limited duration of exposure, rare and severe side effects of our drug candidates may only be uncovered with a significantly larger number of patients exposed to the drug candidates. If our drug candidates receive regulatory approval and we or others discover undesirable side effects caused by such drugs (or any other similar drugs) or that such drug candidates are less effective than previously believed, a number of potentially significant negative consequences could result, including:
| ● |
the FDA, NMPA, TGA, Health Canada, EMA or other comparable regulatory authorities may withdraw or limit their approval of such drug candidates; |
| ● |
the FDA, NMPA, TGA, Health Canada, EMA or other comparable regulatory authorities may require the addition of labeling statements, such as a “boxed” warning or a contra-indication; |
| ● |
we may be required to create a medication guide outlining the risks of such side effects for distribution to patients; |
| ● |
we may be required to change the way such drug candidates are distributed or administered, conduct additional clinical trials or change the labeling of our drug candidates; |
| ● |
the FDA, NMPA, TGA, Health Canada, EMA or other comparable regulatory authorities may require the development of risk evaluation and mitigation strategies and plans to mitigate risks, which could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools; |
| ● |
we may be subject to regulatory investigations and government enforcement actions; |
| ● |
we may decide to, or be required to, remove such drug candidates from the marketplace; |
| ● |
we could be sued and held liable for injury caused to individuals exposed to or taking our drugs; and |
| ● |
our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the affected drug candidates and could substantially increase the costs of commercializing our drugs, if approved, and significantly impact our ability to successfully commercialize our drugs and generate revenue.
Adverse drug reactions and negative results from off-label use of our products could materially harm our business reputation, product brand name, commercial operations, financial condition, including the value of our Common Stock, and expose us to liability.
Products distributed or sold in the pharmaceutical market may be subject to off-label drug use. Off-label drug use is prescribing a product for an indication, patient population, dosage strength or frequency, or other condition of use that is not in accordance with regulatory approved usage and labeling. Even though the FDA, NMPA, TGA, Health Canada, EMA and other comparable regulatory authorities actively enforce the laws and regulations prohibiting the promotion of off-label use, there remains the risk that our products are subject to off-label drug use and are prescribed in a patient population or dosage that has not been approved by competent authorities. Off-label use of our products may be less effective or entirely ineffective and may cause adverse drug reactions. Any of these occurrences can create negative publicity and significantly harm our business reputation, product brand name, commercial operations, and financial condition, including the value of our Common Stock. In addition, this may negatively impact our ability to commercialize our products because it could influence third party payers reimbursement and formulary placement decisions about our products. These occurrences may also expose us to liability and cause, or lead to, a delay in the progress of our clinical trials and may also ultimately result in failure to obtain regulatory approval for our drug candidates.
Off-label use of our products could expose us to government investigation or prosecution.
Regulatory bodies that enforce laws and regulations to prohibit off-label use may investigate whether our products are being used off-label. Even though we take steps to prevent off-label promotion of our products, this would not necessarily prevent regulatory or prosecuting agencies from investigating and taking action against us as if we were engaged in off-label promotion.
As a company, we have no experience in launching and marketing drugs. If we are unable to develop sales, marketing and distribution capabilities or enter into sales, marketing and distribution agreements or arrangements with third parties, we may not be successful in commercializing any drugs, if approved, or generating drug candidate sales revenue.
We have not yet demonstrated an ability to launch and commercialize any of our drug candidates, if approved. As a result, our ability to successfully commercialize any approved drugs may involve more inherent risk, take longer, and cost more than it would if we were a company with prior experience launching and marketing drugs.
We will have to compete with other pharmaceutical and biopharmaceutical companies to recruit, hire, train and retain marketing and sales personnel. We must either develop internal sales, marketing, and commercial distribution capabilities for any or all of our approved drugs or pursue collaborative arrangements regarding the sales and marketing of our approved drugs. However, there can be no assurance that we will be able to develop such distribution capabilities or establish or maintain such collaborative arrangements, or if we are able to do so, that they will have effective sales forces. Any revenue we receive will depend upon the efforts of such third parties. We would have little or no control over the marketing and sales efforts of such third parties, and our revenue from product sales, if approved, may be lower than if we had commercialized any approved drugs by ourselves or we may fail to generate any product sales revenue in the future at all.
We face substantial competition from other pharmaceutical and biotechnology companies, and our operating results may suffer if we fail to compete effectively.
The development and commercialization of new drugs is highly competitive. We face competition from major pharmaceutical companies, specialty pharmaceutical companies, and biotechnology companies worldwide. There are a number of large pharmaceutical and biotechnology companies that currently market and sell drugs or are pursuing the development of drugs for the treatment of neurological diseases and other disorders for which we are commercializing our drugs or developing our drug candidates. Potential competitors also include academic institutions, government agencies, and other public and private research organizations that conduct research, seek patent protection and establish collaborative arrangements for research, development, manufacturing, and commercialization.
Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize drugs that are safer, more effective, have fewer or less severe side effects, are more convenient, or are less expensive than any drugs that we may commercialize or may develop. Our competitors may also obtain approval from the FDA, NMPA, TGA, Health Canada, EMA or other comparable regulatory authorities for their drugs more rapidly than we may obtain approval for our drugs, which could result in our competitors establishing a strong market position before we are able to enter the market and/or could slow our regulatory approval.
Many of our current or future competitors have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals, and marketing approved drugs than we do. Mergers and acquisitions in the pharmaceutical and biotechnology industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller and other early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These third parties compete with us in recruiting and retaining qualified scientific and management personnel, establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
We may be subject, directly or indirectly, to applicable anti-kickback, false claims laws, physician payment transparency laws, privacy and security laws, fraud and abuse laws or similar healthcare and security laws and regulations in the U.S. and other jurisdictions, which could expose us to criminal sanctions, civil penalties, contractual damages, reputational harm and diminished profits and future earnings.
Healthcare providers, physicians and others play a primary role in the recommendation and prescription of any products for which we obtain regulatory approval. If we obtain FDA approval for any of our drug candidates and begin commercializing those drugs in the U.S., our operations may be subject to various federal and state fraud and abuse laws, including, without limitation, the federal Anti-Kickback Statute, the federal False Claims Act, and physician payment sunshine laws and regulations. These laws may impact, among other things, our proposed sales, marketing, and education programs. In addition, we may be subject to patient privacy regulation by both the federal government and the states in which we conduct our business. Restrictions under applicable federal and state healthcare laws and regulations include the following:
| ● |
the federal Anti-Kickback Statute prohibits, among other things, persons and entities from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward, or in return for, either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under a federal healthcare program such as Medicare and Medicaid. A person or entity does not need to have actual knowledge of the federal Anti-Kickback Statute or specific intent to violate it in order to have committed a violation. In addition, the government may assert that a claim including items or services resulting from a violation of the U.S. federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the civil False Claims Act; |
| ● |
the federal false claims and civil monetary penalties laws, including the civil False Claims Act and the Civil Monetary Penalties Law, which can be enforced by private citizens through civil whistleblower or qui tam actions, prohibit individuals or entities from, among other things, knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government; |
| ● |
HIPAA prohibits, among other things, executing or attempting to execute a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation; |
| ● |
HIPAA, as amended by HITECH, and their implementing regulations, also imposes obligations, including mandatory contractual terms, certain covered healthcare providers, health plans, and healthcare clearinghouses and their respective business associates and covered subcontractors that perform services for them that involve the use, or disclosure of, individually identifiable health information with respect to safeguarding the privacy, security and transmission of individually identifiable health information; and |
| ● |
the federal Physician Payments Sunshine Act requires applicable manufacturers of covered drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program, with specific exceptions, to annually report to the CMS information regarding payments and other transfers of value to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, as well as information regarding ownership and investment interests held by physicians and their immediate family members. Beginning in 2022, applicable manufacturers also will be required to report such information regarding payments and transfers of value provided during the previous year to physician assistants, nurse practitioners, clinical nurse specialists, anesthesiologist assistants, certified nurse anesthetists and certified nurse-midwives. The information reported is publicly available on a searchable website, with disclosure required annually. |
Additionally, we are subject to state and non-U.S. equivalents of each of the healthcare laws described above, among others, some of which may be broader in scope and may apply to healthcare services reimbursed by any source, not just governmental payors, including private insurers. In addition, some states have passed laws that require pharmaceutical companies to comply with the April 2003 Office of Inspector General Compliance Program Guidance for Pharmaceutical Manufacturers and/or other voluntary industry codes of conduct. Several states also impose other marketing restrictions or require pharmaceutical companies to make marketing or price disclosures to the state. There are ambiguities as to what is required to comply with these state requirements, and if we fail to comply with applicable state law requirements, we could be subject to penalties.
Violations of fraud and abuse laws may be punishable by criminal and/or civil sanctions, including penalties, fines and/or exclusion or suspension from federal and state healthcare programs such as Medicare and Medicaid and debarment from contracting with the U.S. government.
Neither the U.S. government nor the U.S. courts have provided definitive guidance on limitations to potential liability under the fraud and abuse laws as they may apply to our business. Law enforcement authorities are increasingly focused on enforcing these laws, often using new and creative legal theories, and it is possible that some of our practices may be challenged under these laws. Efforts to ensure that our business arrangements with third parties will comply with applicable healthcare laws and regulations will involve substantial costs. Regardless of the compliance efforts, it is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. In addition, private individuals have the ability to bring actions on behalf of the U.S. government under the federal False Claims Act as well as under the false claims laws of several states. If any such actions are instituted against us, defending against such actions, even if successful, would distract us and our key personnel from our core mission and impose potentially significant costs. If we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business, including the imposition of civil, criminal and administrative penalties, damages, disgorgement, monetary fines, possible exclusion from participation in Medicare, Medicaid, and other federal healthcare programs, contractual damages, reputational harm, diminished profits and future earnings, and curtailment of our operations, any of which could adversely affect our ability to operate our business and our results of operations. In addition, the approval and commercialization of any of our approved drugs outside the U.S. will also likely subject us to non-U.S. equivalents of the healthcare laws mentioned above, among other non-U.S. laws, as well as the U.S. Foreign Corrupt Practices Act.
If any of the physicians or other providers or entities with whom we expect to do business are found to be not in compliance with applicable laws, they may be subject to criminal, civil or administrative sanctions, including exclusions from government funded healthcare programs, which may also adversely affect our business.
We may face difficulties from changes to current regulations and future legislation.
In the U.S. and some foreign jurisdictions, there have been, and continue to be, several legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval of drug candidates, restrict or regulate post-approval activities, and affect the ability to profitably sell drug candidates for which marketing approval is obtained. Among policy makers and payors in the U.S. and elsewhere, there is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality and/or expanding access. In the U.S., the pharmaceutical industry has been a particular focus of these efforts and has been significantly affected by major legislative initiatives.
For example, the Affordable Care Act has substantially changed healthcare financing and delivery by both governmental and private insurers. Among the Affordable Care Act provisions of importance to the pharmaceutical and biotechnology industries are the following: among other things, subjected biological products to potential competition by lower-cost biosimilars, created a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for drugs that are inhaled, infused, instilled, implanted or injected, increased the minimum Medicaid rebates owed by manufacturers under the Medicaid Drug Rebate Program and extended the rebate program to individuals enrolled in Medicaid managed care organizations, established annual fees and taxes on manufacturers of certain branded prescription drugs, and created a new Medicare Part D coverage gap discount program, in which manufacturers must agree to offer 70% point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period, as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D.
Some of the provisions of the Affordable Care Act have yet to be implemented, and there have been legal and political challenges to certain aspects of the Affordable Care Act. For example, on June 17, 2021 the U.S. Supreme Court dismissed a challenge on procedural grounds that argued the Affordable Care Act is unconstitutional in its entirety because the “individual mandate” was repealed by Congress. Thus, the Affordable Care Act will remain in effect in its current form. Further, prior to the U.S. Supreme Court ruling, on January 28, 2021, President Biden issued an executive order that initiated a special enrollment period for purposes of obtaining health insurance coverage through the Affordable Care Act marketplace, which began on February 15, 2021 and remained open through August 15, 2021. The executive order also instructed certain governmental agencies to review and reconsider their existing policies and rules that limit access to healthcare, including among others, reexamining Medicaid demonstration projects and waiver programs that include work requirements, and policies that create unnecessary barriers to obtaining access to health insurance coverage through Medicaid or the Affordable Care Act. It is possible that the Affordable Care Act will be subject to judicial or Congressional challenges in the future. It is unclear how any such challenges and the healthcare reform measures of the Biden administration will impact the Affordable Care Act and our business.
Further legislation or regulation could be passed that could harm our business, financial condition and results of operations. Other legislative changes have been proposed and adopted since the Affordable Care Act was enacted. For example, in August 2011, President Obama signed into law the Budget Control Act of 2011, which, among other things, included aggregate reductions to Medicare payments to providers of 2% per fiscal year, which went into effect beginning on April 1, 2013, with COVID-19 relief legislation suspending the 2% Medicare sequester from May 1, 2020 through December 31, 2021. In January 2013, the American Taxpayer Relief Act of 2012 was signed into law, which, among other things, further reduced Medicare payments to several types of providers, including hospitals, imaging centers and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. Additionally, on March 11, 2021, President Biden signed the American Rescue Plan Act of 2021 into law, which eliminates the statutory Medicaid drug rebate cap, currently set at 100% of a drug’s average manufacturer price, for single source and innovator multiple source drugs, beginning January 1, 2024. Moreover, the Inflation Reduction Act of 2022 may impact existing Medicare programs that cover prescription drugs. In addition to other relevant provisions, the Inflation Reduction Act of 2022 allows the Medicare program to directly negotiate the price of certain high-expenditure prescription drugs covered under Medicare Parts B and D, starting in the year 2028 and 2026, respectively, by setting certain “maximum fair prices.” Moreover, the Inflation Reduction Act of 2022 requires manufacturers to pay rebates to the federal government if prices of certain drugs covered under the Medicare program rise faster than the rate of inflation.
Additionally, there has been increasing legislative and enforcement interest in the U.S. with respect to specialty drug pricing practices. Specifically, there have been several recent U.S. Congressional inquiries and proposed federal legislation designed to, among other things, bring more transparency to drug pricing, reduce the cost of prescription drugs under Medicare, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for drugs. Congress has indicated that it will continue to seek new legislative and/or administrative measures to control drug costs. Additionally, based on a recent executive order, the Biden administration expressed its intent to pursue certain policy initiatives to reduce drug prices. In response to Biden’s executive order, on September 9, 2021, HHS released a Comprehensive Plan for Addressing High Drug Prices that outlines principles for drug pricing reform and sets out a variety of potential legislative policies that Congress could pursue as well as potential administrative actions HHS can take to advance these principles. No legislation or administrative actions have been finalized to implement these principles. In addition, Congress is considering drug pricing as part of the budget reconciliation process. Individual states in the U.S. have also become increasingly active in passing legislation and implementing regulations designed to control biopharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing.
We anticipate that the Affordable Care Act, if substantially maintained in its current form, will continue to result in additional downward pressure on coverage and the price that we receive for any approved product, and could seriously harm our business. Any reduction in reimbursement from Medicare and other government programs may result in a similar reduction in payments from private payors. Further, the implementation of cost containment measures or other healthcare reforms may prevent us from being able to generate revenue, attain profitability, or commercialize our products. Such reforms could have an adverse effect on anticipated revenue from drug candidates that we may successfully develop and for which we may obtain regulatory approval and may affect our overall financial condition and ability to develop drug candidates.
Any failure to perform proper quality control and quality assurance would have a material adverse effect on our business and financial results.
The manufacturing of our drug candidates and any drugs, if approved, is subject to applicable laws, regulations, and GMP. These regulations govern manufacturing processes and procedures, including record keeping and the implementation and operation of quality management systems to control and assure the quality of investigational products and products approved for sale. We apply stringent quality controls at each stage of our production process to comply with these requirements. We perform extensive tests throughout the manufacturing processes to ensure the safety and effectiveness of our drug candidates. We may, however, detect instances in which an unreleased product was produced without adherence to our manufacturing procedures or the raw material used in our production process was not collected to store in accordance with the GMP or other regulations, resulting in a determination that the implicated products should be destroyed.
In addition, if we fail to comply with relevant quality control requirements under laws, regulations, and GMP, we could experience a disruption in the supply of our products, which could delay or prevent further sales of such products, which could have a material adverse effect on our business and financial results.
In addition, quality issues may arise during scale-up activities. If we are unable to successfully ensure consistent and high quality of our products during large-volume production, the sales of our products may not be able to be promoted, which could have a material adverse effect on our business and financial results.
We may explore the licensing of commercialization rights or other forms of collaboration worldwide, which will expose us to additional risks.
Non-U.S. markets are an important component of our growth strategy. We initially intend to focus on opportunities in the U.S., the European Union, Canada, Australia, Japan, Korea and China, in particular. If we fail to obtain licenses or enter into collaboration arrangements with third parties in these or other markets, or if these arrangements are not successful, our revenue-generating growth potential will be adversely affected. Moreover, international business relationships subject us to additional risks that may materially adversely affect our ability to attain or sustain profitable operations, including:
| ● |
efforts to enter into collaboration or licensing arrangements with third parties in connection with our international sales, marketing, and distribution efforts may increase our expenses or divert our management’s attention from the development of our drug candidates; |
| ● |
difficulty of effective enforcement of contractual provisions in foreign jurisdictions; |
| ● |
differing regulatory requirements for drug approvals and marketing internationally, including differing product reimbursement regimes; |
| ● |
changes in a specific market’s political and cultural climate or economic condition; |
| ● |
potential third-party patent rights or potentially reduced protection for intellectual property rights; |
| ● |
unexpected changes in tariffs, trade barriers, and regulatory requirements; |
| ● |
economic weakness, including inflation; |
| ● |
compliance with tax, employment, immigration, and labor laws for employees traveling abroad; |
| ● |
the effects of applicable non-U.S. tax structures and potentially adverse tax consequences; |
| ● |
currency fluctuations, which could result in increased operating expenses and reduced revenue; |
| ● |
production shortages resulting from any events affecting raw material supply or manufacturing capabilities abroad; |
| ● |
workforce uncertainty and labor unrest; |
| ● |
failure of our employees and contracted third parties to comply with Office of Foreign Assets Control rules and regulations and the Foreign Corrupt Practices Act; and |
| ● |
business interruptions resulting from geo-political actions, including war and terrorism, or natural disasters, including earthquakes, volcanoes, typhoons, floods, hurricanes, and fires. |
These and other risks may materially and adversely affect our ability to attain or sustain revenue from international markets and could have a material adverse effect on our business, financial condition, results of operations, and prospects.
Illegal and/or parallel imports and counterfeit pharmaceutical products may reduce demand for our future approved drug candidates and could have a negative impact on our reputation and business.
The imports, whether authorized by governmental policy or illegal, of competing products from countries where government price controls or other market dynamics result in lower prices may adversely affect the demand for any of our future drugs, if approved, and, in turn, may adversely affect our sales and profitability if we commercialize our products. Unapproved foreign imports of prescription drugs are illegal under the current laws of the U.S., China, the European Union, Australia and other jurisdictions. However, illegal imports may continue to occur or even increase as the ability of patients to obtain these lower priced imports continues to grow. Furthermore, cross-border imports from lower-priced markets (parallel imports) into higher-priced markets could harm sales of our future drugs, if approved, and exert commercial pressure on pricing within one or more markets. In addition, competent government authorities may expand consumers’ ability to import lower-priced versions of our future drugs, if approved, or competing products from outside the countries where we operate. Any future legislation or regulations that increase consumer access to lower-priced medicines from outside the countries where we operate could have a material adverse effect on our business.
Certain products distributed or sold in the pharmaceutical market may be manufactured without proper licenses or approvals, or may be fraudulently mislabeled with respect to their content or manufacturers. These products are generally referred to as counterfeit pharmaceutical products. The counterfeit pharmaceutical product control and enforcement system, particularly in developing markets such as China, may be inadequate to discourage or eliminate the manufacturing and sale of counterfeit pharmaceutical products imitating our products. Since counterfeit pharmaceutical products in many cases have very similar appearances to the authentic pharmaceutical products but are generally sold at lower prices, counterfeits of our products can quickly erode the demand for our future drugs, if approved. Our reputation and business could suffer harm as a result of counterfeit pharmaceutical products sold under our or our collaborators’ brand names. In addition, theft of inventory at warehouses, plants or while in-transit, which are not properly stored and which are sold through unauthorized channels, could adversely impact patient safety, as well as our reputation and business.
We rely on third parties to conduct our preclinical studies and clinical trials and we must work effectively with collaborators to develop our drug candidates. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval for or commercialize our drug candidates and our business could be substantially harmed.
We rely on and plan to continue to rely on third-party CROs and third-party vendors to monitor, collect samples, analyze samples, report data, and manage data for our ongoing preclinical and clinical programs. We rely on these third parties for execution of our preclinical studies and clinical trials. While we control only certain aspects of their activities, we are responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol, legal and regulatory requirements, and scientific standards, and our reliance on the CROs does not relieve us of our regulatory responsibilities. We, our CROs, third-party vendors supporting our clinical programs, and our clinical investigators, are required to comply with GCPs, which are regulations and guidelines enforced by the FDA, NMPA, TGA, Health Canada, EMA, and other comparable regulatory authorities for all of our drugs in clinical development. If we, any of our CROs, third-party vendors, or clinical investigators fail to comply with applicable GCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA, NMPA, TGA, Health Canada, EMA or comparable regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. In addition, our pivotal clinical trials must be conducted with products produced under GMP. Our failure, or the failure of any third party, to comply with these regulations may result in our having to repeat clinical trials, which would delay the regulatory approval process.
If any of our relationships with these third parties terminates, we may not be able to enter into arrangements with alternative CROs, vendors or clinical investigators, or to do so on commercially reasonable terms. In addition, our CROs are not our employees, and except for remedies available to us under our agreements with such CROs, we cannot control whether or not they devote sufficient time and resources to our ongoing clinical and other programs. If CROs do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they or our clinical investigators obtain is compromised due to the failure to adhere to our clinical protocols, regulatory requirements, or for other reasons, our clinical trials may be extended, delayed or terminated and we may not be able to obtain regulatory approval for or successfully commercialize our drug candidates. As a result, our results of operations and any commercial prospects for our drugs would be harmed, our costs would increase and our ability to generate revenues would be delayed.
Switching or adding additional CROs or clinical investigators involves additional cost and delays, which can materially affect our ability to meet our desired clinical development timelines. There can be no assurance that we will not encounter these delays in the future or that these delays or challenges will not have a material adverse effect on our business, financial condition, results of operations, and prospects.
Our ability to generate future revenues is dependent on our ability to work effectively with collaborators to develop our drug candidates, including to obtain regulatory approval. Our arrangements with collaborators will be critical to successfully bringing products to market and commercializing them, if approved. We rely on collaborators in various respects, including to undertake research and development programs, to conduct clinical trials, to manage or assist with the regulatory filings and approval process, and to assist with our commercialization efforts. We do not control our collaborators and we cannot ensure that these third parties will adequately and timely perform all of their obligations to us. If they fail to complete the remaining studies successfully, or at all, it would delay, adversely affect or prevent regulatory approval. We cannot guarantee the satisfactory performance of any of our collaborators’ obligations and if any of our collaborators breach or terminate their agreements with us, we may not be able to successfully commercialize the drug candidates which could materially and adversely affect our business, financial condition, results of operations, and prospects.
We are also unable to predict how changing global economic or political conditions, such as the ongoing conflicts between Ukraine and Russia and Israel and Palestine and related global economic sanctions, or potential global health concerns, such as future health epidemics or pandemics, may impact our CROs, clinical investigators, third-party vendors, and other collaborators. Any negative impact could have a material adverse effect on our business, financial condition, results of operations, and prospects.
We have entered into research collaborations and may form or seek collaborations, joint ventures or strategic alliances or enter into licensing arrangements in the future, and we may not realize the benefits of such collaborations, alliances, or licensing arrangements.
We may form or seek strategic alliances, create joint ventures or collaborations, or enter into licensing arrangements with third parties that we believe will complement or augment our development and commercialization efforts with respect to our drug candidates and any future drug candidates that we may develop. Any of these relationships may require us to incur non-recurring and other costs, increase our near and long-term expenditures, disrupt our management and business, or issue securities that dilute our existing stockholders.
While we have entered into collaborative research arrangements with some of the world’s leading academic institutions and research centers and are working with key scientists in the field of central nervous system disorders, we face significant competition in seeking appropriate strategic partners and the negotiation process is time-consuming and complex. Moreover, we may not be successful in our efforts to establish a strategic partnership or other alternative arrangements for our drug candidates because they may be deemed to be at too early of a stage of development for collaborative effort and third parties may not view our drug candidates as having the requisite potential to demonstrate safety and efficacy or commercial viability. If and when we collaborate with a third party for development and commercialization of a drug candidate, if approved, we can expect to relinquish some or all of the control over the future success of that drug candidate to the third party. For any drug candidates that we may seek to in-license from third parties, we may face significant competition from other pharmaceutical or biotechnology companies with greater resources or capabilities than we have, and any agreement that we do enter into may not result in the anticipated benefits.
Further, collaborations involving our drug candidates are subject to numerous risks, which may include the following:
| ● |
collaborators have significant discretion in determining the efforts and resources that they will apply to a collaboration; |
| ● |
collaborators may not pursue development and commercialization of our drug candidates, if approved, or may elect not to continue or renew development or commercialization programs based on clinical trial results, changes in their strategic focus due to the acquisition of competitive drugs, availability of funding, or other external factors outside of our control, such as a business combination that diverts resources or creates competing priorities; |
| ● |
collaborators may delay clinical trials, provide insufficient funding for a clinical trial, stop a clinical trial, abandon a drug candidate, repeat or conduct new clinical trials, or require a new formulation of a drug candidate for clinical testing; |
| ● |
collaborators could independently develop, or develop with third parties, drugs that compete directly or indirectly with our drugs; |
| ● |
collaborators with marketing and distribution rights to one or more drugs may not commit sufficient resources to their marketing and distribution; |
| ● |
collaborators may not properly develop, maintain, or defend our intellectual property rights or may use our intellectual property or proprietary information in a way that gives rise to actual or threatened litigation that could jeopardize or invalidate our intellectual property or proprietary information or expose us to potential liability; |
| ● |
disputes may arise between us and a collaborator that cause the delay or termination of the research, development, or commercialization of our drug candidates, if approved, or that result in costly litigation or arbitration that diverts management attention and resources; |
| ● |
collaborations may be terminated and, if terminated, may result in a need for additional capital to pursue further development or commercialization of our drug candidates, if approved; and |
| ● |
collaborators may own or co-own intellectual property covering our drugs that results from our collaborating with them, and in such cases, we would not have the exclusive right to commercialize such intellectual property. |
As a result, we may not be able to realize the benefit of any current or future research collaborations, strategic partnerships, or the potential licensing of third-party drugs if we are unable to successfully integrate such products with our existing operations and company culture, which could delay our timelines or otherwise adversely affect our business. We also cannot be certain that, following a strategic transaction or license, we will achieve the revenue or net income that justifies such transaction. If we are unable to reach agreements with suitable collaborators on a timely basis, on acceptable terms, or at all, we may have to curtail the development of one of more of our drug candidates, reduce or delay our development program or one or more of our future development programs, delay our potential commercialization or reduce the scope of any sales or marketing activities, or increase our expenditures and undertake development or commercialization activities at our own expense. If we elect to fund and undertake development or commercialization activities on our own, we may need to obtain additional expertise and additional capital, which may not be available to us on acceptable terms or at all. If we fail to enter into collaborations and do not have sufficient funds or expertise to undertake the necessary development and commercialization activities, we may not be able to further develop our drug candidates or, if approved, bring them to market and generate product sales revenue, which would harm our business, financial condition, results of operations, and prospects.
Our business depends on the use of raw materials, and a decrease in the supply or an increase in the cost of these raw materials or any quality issues in such raw materials could materially and adversely affect our business, financial condition, results of operations, and prospects.
In order to manufacture our products, we must obtain sufficient quantities of high-quality raw materials at commercially acceptable prices and in a timely manner. Certain critical raw materials, such as wires made of high-purity gold and other transition elements, are available from a limited number of suppliers in the market. As a result, any disruption in production or inability of our suppliers to produce adequate quantities to meet our needs could impair our ability to operate our business on a day-to-day basis and to continue our research and development of future drug candidates. Moreover, we expect our demand for such materials to increase as we expand our business scale and commercialize our products, if approved, and we cannot guarantee that current suppliers have the capacity to meet our demand. We are also exposed to the risk of increased material costs, which we may not be able to pass on to customers and as a result, we could have lower profitability. In addition, although we have implemented quality inspection procedures on such materials before they are used in our manufacturing processes and also require our suppliers to maintain high quality standards, we cannot guarantee that we will be able to secure sufficient quantities of raw materials at high quality standards, nor detect all quality issues in the supplies we use. For example, should the highly purified water that we utilize be compromised in any way, it could render entire batches unusable or, depending on the nature of the impurity, could be dangerous to patients. Further, we cannot assure you that third parties will be able to maintain and renew all licenses, permits, and approvals necessary for their operations or comply with all applicable laws and regulations. Failure to do so by them may lead to interruption in their business operations, which in turn may result in shortages of the raw materials utilized by us. If we are unable to obtain adequate raw materials and the quality of our products suffers as a result, we may have to delay clinical trials and regulatory filings, recall our products, be subject to product liability claims, fail to comply with continuing regulatory requirements, and incur significant costs to rectify such issues, which may have a material and adverse effect on our business, financial condition, results of operations, and prospects.
If we are unable to obtain and maintain sufficient patent protection for our drug candidates through intellectual property rights, or if the scope of such intellectual property rights obtained is not sufficiently broad, third parties could develop and commercialize products similar or identical to our products, and our ability to commercialize our approved drugs successfully may be adversely affected.
Our success depends in large part on our ability to protect our proprietary technology, drug candidates in clinical trials, and approved drugs on market (if approved) from competition by obtaining, maintaining and enforcing our intellectual property rights, including patent rights. We seek to protect the drug candidates and technology that we consider commercially important by filing patent applications in most important commercial markets, including the U.S., China, Europe, Canada, Japan, Korea, and other countries, relying on trade secrets or pharmaceutical regulatory protection or employing a combination of these methods. However, the patent prosecution process is expensive, time-consuming and complex, and we may not be able to file, prosecute, maintain, enforce or license all necessary or desirable patent applications at a reasonable cost or in a timely manner. It is also possible that we will fail to identify patentable aspects of our research and development output before it is too late to obtain patent protection. As a result, we may not be able to prevent competitors from developing and commercializing competitive drugs in all such fields and territories.
Patents may be invalidated and patent applications may not be granted for a number of reasons, including known or unknown prior art, deficiencies in the patent application or the lack of novelty of the underlying invention or technology. Although we enter into non-disclosure and confidentiality agreements with parties who have access to confidential or patentable aspects of our research and development output, such as our employees, corporate collaborators, outside scientific collaborators, contract manufacturers, consultants, advisors and any other third parties, any of these parties may breach such agreements and disclose such output before a patent application is filed, thereby jeopardizing our ability to seek patent protection. In addition, publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in the U.S. and other jurisdictions are typically not published until 18 months after filing, or in some cases, not at all. Therefore, we cannot be certain that we were the first to make the inventions claimed in our patents or pending patent applications or that we were the first to file for patent protection of such inventions. Furthermore, China, EPO, and the U.S. have adopted the “first-to-file” system under which whoever first files a patent application will be awarded the patent if all other patentability requirements are met. Under the first-to-file system, third parties may be granted a patent relating to a technology which we invented.
The coverage sought by the claims in a patent application can be significantly reduced before the patent is issued, and the scope of the claims can be reinterpreted after issuance. Even if patent applications we license or own currently or in the future issue as patents, they may not issue in a form that will provide us with any meaningful protection, prevent competitors or other third parties from competing with us, or otherwise provide us with any competitive advantage. In addition, the patent position of biotechnology and pharmaceutical companies generally is highly uncertain, involves complex legal and factual questions, and has been the subject of much litigation in recent years. As a result, the issuance, scope, validity, enforceability and commercial value of our patent rights are highly uncertain.
The issuance of a patent is not conclusive as to our inventorship, scope, validity, or enforceability, and our patents may be challenged in the courts or patent offices in any country. We may be subject to a third-party preissuance submission of prior art to the U.S. Patent and Trademark Office (“USPTO”), or become involved in opposition, derivation, revocation, re-examination, post-grant and inter partes review, or interference proceedings or similar proceedings in foreign jurisdictions challenging our patent rights or the patent rights of others. An adverse determination in any such submission, proceeding or litigation could reduce the scope of, or invalidate, our patent rights, allow third parties to commercialize our technology or approved drugs and compete directly with us without payment, or result in our inability to manufacture or commercialize drug candidates and approved drugs without infringing, misappropriating or otherwise violating third-party patent rights. Moreover, we may have to participate in interference proceedings declared by the USPTO to determine priority of invention or in post-grant challenge proceedings, such as oppositions in a foreign patent office, that challenge the priority of our invention or other features of patentability of our patents and patent applications. Such challenges may result in loss of patent rights, loss of exclusivity, or in patent claims being narrowed, invalidated, or held unenforceable, which could limit our ability to stop others from using or commercializing similar or identical technology and products, or limit the duration of the patent protection of our technology and drug candidates. Such proceedings also may result in substantial costs and require significant time from our scientists and management, even if the eventual outcome is favorable to us. Consequently, we do not know whether any of our technology or drug candidates will be protectable or remain protected by valid and enforceable patents. Our competitors or other third parties may be able to circumvent our patents by developing similar or alternative technologies or products in a non-infringing manner.
Furthermore, although various extensions may be available, the life of a patent and the protection it affords, are limited. For example, approved therapies may face competition from generic medications after the related patents have expired, or if they are challenged and invalidated even before their expiry. Manufacturers of generic drugs may challenge the scope, validity or enforceability of our patents in court, and we may not be successful in enforcing or defending those intellectual property rights and, as a result, may not be able to develop or market the relevant product exclusively, which would have a material adverse effect on any potential sales of that product. The issued patents and pending patent applications, if issued, for our drug candidates are expected to expire on various dates as described in “Business—Intellectual Property” of this Annual Report. Upon the expiration of our issued patents or patents that may issue from our pending patent applications, we will not be able to assert such patent rights against potential competitors and our business and results of operations may be adversely affected.
Given the amount of time required for the development, testing and regulatory review of new drug candidates, patents protecting such drug candidates might expire before or shortly after such drugs are commercialized. As a result, our patents and patent applications may not provide us with sufficient rights to exclude others from commercializing products similar or identical to our products. Moreover, some of our patents and patent applications may in the future be co-owned with third parties. If we are unable to obtain an exclusive license to any such third-party co-owners’ interest in such patents or patent applications, such co-owners may be able to license their rights to other third parties, including our competitors, and our competitors could market competing products and technology. In addition, we may need the cooperation of any such co-owners of our patents in order to enforce such patents against third parties, and such cooperation may not be provided to us. Any of the foregoing could have a material adverse effect on our competitive position, business, financial conditions, results of operations, and prospects.
Intellectual property discovered through government funded programs may be subject to federal regulations such as “march-in” rights, certain reporting requirements and a preference for U.S.-based companies. Compliance with such regulations may limit our exclusive rights and limit our ability to contract with non-U.S. manufacturers.
Although we do not currently own issued patents or pending patent applications that have been generated through the use of U.S. government funding, we may acquire or license in the future intellectual property rights that have been generated through the use of U.S. government funding or grants. Pursuant to the Bayh-Dole Act of 1980, the U.S. government may have certain rights in inventions developed with government funding. These U.S. government rights include a non-exclusive, non-transferable, irrevocable worldwide license to use inventions for any governmental purpose. In addition, the U.S. government has the right, under certain limited circumstances, to require us to grant exclusive, partially exclusive, or non-exclusive licenses to any of these inventions to a third party if it determines that: (1) adequate steps have not been taken to commercialize the invention; (2) government action is necessary to meet public health or safety needs; or (3) government action is necessary to meet requirements for public use under federal regulations (also referred to as “march-in rights”). Such “march-in” rights can apply to new subject matter arising from the use of such government funding or grants and should not extend to pre-existing subject matter or subject matter arising from funds unrelated to the government funding or grants If the U.S. government exercised its march-in rights in our future intellectual property rights that are generated through the use of U.S. government funding or grants, we could be forced to license or sublicense intellectual property developed by us or that we license on terms unfavorable to us, and there can be no assurance that we would receive compensation from the U.S. government for the exercise of such rights. The U.S. government also has the right to take title to these inventions if we fail to disclose the invention to the government or fail to file an application to register the intellectual property within specified time limits. Intellectual property generated under a government funded program is also subject to certain reporting requirements, compliance with which may require us to expend substantial resources. In addition, the U.S. government requires that any products embodying any of these inventions or produced through the use of any of these inventions be manufactured substantially in the United States. This preference for U.S. industry may be waived by the federal agency that provided the funding if the owner or assignee of the intellectual property can show that reasonable but unsuccessful efforts have been made to grant licenses on similar terms to potential licensees that would be likely to manufacture substantially in the United States or that under the circumstances domestic manufacture is not commercially feasible. This preference for U.S. industry may limit our ability to contract with non-U.S. product manufacturers for products covered by such intellectual property.
We may not be able to protect our intellectual property rights throughout the world or prevent unfair competition by third parties.
Filing, prosecuting, maintaining, and defending patents on drug candidates in all countries throughout the world could be prohibitively expensive for us, and our intellectual property rights in some non-U.S. countries can have a different scope and strength than do those in the U.S. In addition, the laws of certain non-U.S. countries do not protect intellectual property rights to the same extent as the laws of the U.S. Consequently, we may not be able to prevent third parties from practicing our inventions in all countries outside the U.S., or from selling or importing drugs made using our inventions in and into the U.S. or non-U.S. jurisdictions. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own drugs and further, may export otherwise infringing drugs to non-U.S. jurisdictions where we have patent protection, but where enforcement rights are not as strong as those in the U.S. These drugs may compete with our future approved drugs and our patent rights or other intellectual property rights may not be effective or adequate to prevent them from competing.
Geo-political actions in the U.S. and in foreign countries could also increase the uncertainties and costs surrounding the prosecution, maintenance, and defense of our patents. For example, the U.S. and foreign government actions related to Russia’s invasion of Ukraine may limit or prevent prosecution, maintenance, and defense of patents in Russia. These actions could result in abandonment or lapse of our patents, resulting in partial or complete loss of patent rights in Russia. If such an event were to occur, it could have a material adverse effect on our business. In addition, a decree was adopted by the Russian government in March 2022, allowing Russian companies and individuals to exploit inventions owned by patentees that have citizenship or nationality in, are registered in, or have predominately primary place of business or profit-making activities in the United States and other countries that Russia has deemed unfriendly without consent or compensation. Consequently, we would not be able to prevent third parties from practicing our inventions in Russia or from selling or importing drugs made using our inventions in and into Russia. Accordingly, our competitive position may be impaired, and our business, financial condition, results of operations, and prospects may be adversely affected.
We may become involved in lawsuits to protect or enforce our intellectual property, which could be expensive, time consuming and unsuccessful. Our patent rights relating to our drugs could be found invalid or unenforceable if challenged in court or before the U.S. Patent and Trademark Office or comparable non-U.S. authority.
Competitors may infringe our patent rights or misappropriate or otherwise violate our intellectual property rights. To counter infringement or unauthorized use, litigation may be necessary in the future to enforce or defend our intellectual property rights, protect our trade secrets or determine the validity and scope of our own intellectual property rights or the proprietary rights of others. Enforcement or defense of intellectual property rights can be expensive and time consuming. Any claims that we assert against perceived infringers could also provoke these parties to assert counterclaims against us alleging that we infringe their intellectual property rights. Many of our current and potential competitors have the ability to dedicate substantially greater resources to enforce and/or defend their intellectual property rights than we can. Accordingly, despite our efforts, we may not be able to prevent third parties from infringing upon or misappropriating our intellectual property. An adverse result in any litigation proceeding could put our patents, as well as any patents that may issue in the future from our pending patent applications, at risk of being invalidated, held unenforceable or interpreted narrowly. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation.
In patent litigation in the U.S., defendant counterclaims in district courts or in the Patent Trademark and Appeal Board alleging invalidity or unenforceability are commonplace, and there are numerous grounds upon which a third party can assert invalidity or unenforceability of a patent. Third parties may also raise similar claims before administrative bodies in the U.S. or abroad, even outside the context of litigation. Such mechanisms include ex parte re-examination, inter partes review, post-grant review, derivation and equivalent proceedings in non-U.S. jurisdictions, such as opposition proceedings. Such proceedings could result in revocation or amendment to our patents in such a way that they no longer cover and protect our drug candidates. The outcome following legal assertions of invalidity and unenforceability is unpredictable. With respect to the validity of our patents, for example, we cannot be certain that there is no invalidating prior art of which we, our patent counsel, and the patent examiner were unaware during prosecution. If a defendant were to prevail on a legal assertion of invalidity and/or unenforceability, we would lose at least part, and perhaps all, of the patent protection on our drug candidates. Such a loss of patent protection could have a material adverse impact on our business.
We may not be able to prevent misappropriation of our trade secrets or confidential information, particularly in countries where the laws may not protect those rights as fully as in the U.S. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation.
If we are sued for infringing the intellectual property rights of third parties, such litigation could be costly and time consuming and could prevent or delay us from developing or commercializing our drug candidates.
Our commercial success depends in part on our avoiding infringement of the patents and other intellectual property rights of third parties. We are aware of other issued patents belonging to third parties that exist in fields in which we are developing our drug candidates. There may also be third-party patents or patent applications of which we are currently unaware, and given the dynamic area in which we operate, additional patents are likely to be issued that relate to some aspects of our business. There is a substantial amount of litigation and other claims and proceedings involving patent and other intellectual property rights in the biotechnology and pharmaceutical industries generally. As the biotechnology and pharmaceutical industries expand and more patents are issued, the risk increases that our drug candidates may give rise to claims of infringement of the patent rights of others.
Third parties may assert that we are using technology in violation of their patent or other proprietary rights. Defense of these claims, regardless of their merit, could involve substantial litigation expense and divert our technical personnel, management personnel, or both from their normal responsibilities. If third parties bring successful claims against us for infringement of their intellectual property rights, we may be subject to injunctive or other equitable relief, which could prevent us from developing and commercializing one or more of our drug candidates. We may also have to pay substantial damages, including treble damages and attorneys’ fees in the case of willful infringement, or redesign our infringing drug candidates, which may be impossible or require substantial time and cost. In the event of an adverse result in any such litigation, or even in the absence of litigation, we may need to obtain licenses from third parties to advance our research or allow commercialization of our drug candidates. Any such license might not be available on reasonable terms or at all. In the event that we are unable to obtain such a license, we would be unable to further develop and commercialize one or more of our drug candidates, which could harm our business significantly. We may also elect to enter into license agreements in order to settle patent infringement claims or to resolve disputes prior to litigation, and any such license agreements may require us to pay royalties and other fees that could significantly harm our business.
Intellectual property litigation may lead to unfavorable publicity that harms our reputation and increases our operating losses, causing the market price of our Common Stock to decline.
During the course of any intellectual property litigation, there could be public announcements of the results of hearings, motions or other interim proceedings or developments, and if securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the market price of our Common Stock. Such litigation or proceedings could substantially increase our operating losses and reduce the resources available for development activities or any future sales, marketing, or distribution activities. We may not have sufficient financial or other resources to adequately conduct such litigation or proceedings. Some of our competitors may be able to sustain the costs of such litigation or proceedings more effectively than we can because of their greater financial resources. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could have a material adverse effect on our ability to compete in the marketplace.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for noncompliance with these requirements.
Periodic maintenance fees on any issued patent are due to be paid to the USPTO and most foreign jurisdictions either annually or in several stages over the lifetime of the patent. The USPTO and various non-U.S. governmental patent agencies require compliance with a number of procedural, documentary, fee payment, and other similar provisions during the patent application process. Although an inadvertent lapse can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. Noncompliance events that could result in abandonment or lapse of a patent or patent application include failure to respond to official actions within prescribed time limits, non-payment of fees, and failure to properly legalize and submit formal documents. In any such event, our competitors might be able to enter the market, which would have a material adverse effect on our business.
If we do not obtain patent term extension and data exclusivity for any drug candidates we may develop, our business may be materially harmed.
Depending upon the timing, duration, and specifics of any FDA marketing approval of any drug candidates we may develop, one or more of our U.S. patents may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Action of 1984, or Hatch Waxman Amendments. The Hatch Waxman Amendments permit a patent extension term of up to five years as compensation for patent term lost during clinical trials and the FDA regulatory review process. A comparable extension right may exist in other foreign jurisdictions as well. A patent term extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of drug approval, only one patent may be extended and only those claims covering the approved drug, a method for using it, or a method for manufacturing it may be extended. However, we may not be granted an extension because of, for example, failing to exercise due diligence during the testing phase or regulatory review process, failing to apply within applicable deadlines, failing to apply prior to expiration of relevant patents, or otherwise failing to satisfy applicable requirements. Moreover, the applicable time period or the scope of patent protection afforded could be less than we request.
In addition, no patent term extension system has been established in China beyond the new pilot program, and implementation of the pilot program may not occur quickly. As a result, the patents we have in China are not yet eligible to be extended for patent term lost during clinical trials and the regulatory review process. If we are unable to obtain patent term extension or if the term of any such extension is less than we request, our competitors may obtain approval of competing products following our patent expiration, and our business, financial condition, results of operations, and prospects could be materially harmed.
Changes in patent law could diminish the value of patents in general, thereby impairing our ability to protect our drug candidates.
The U.S. has recently enacted and is currently implementing wide-ranging patent reform legislation. Recent U.S. Supreme Court rulings have narrowed the scope of patent protection available in certain circumstances and weakened the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents once obtained, if any. Depending on decisions by the U.S. Congress, the federal courts and the USPTO, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce our existing patents and patents that we might obtain in the future. There could be similar changes in the laws of foreign jurisdictions that may impact the value of our patent rights or other intellectual property rights.
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position would be harmed.
In addition to our issued patents and pending patent applications, we rely on trade secrets, including unpatented know-how, technology, and other proprietary information, to maintain our competitive position and to protect our drug candidates. We seek to protect these trade secrets, in part, by entering into non-disclosure and confidentiality agreements with parties that have access to them, such as our employees, corporate collaborators, outside scientific collaborators, sponsored researchers, consultants, advisors and other third parties. We also enter into confidentiality and invention or patent assignment agreements with our employees and consultants. However, any of these parties may breach such agreements and disclose our proprietary information, and we may not be able to obtain adequate remedies for such breaches. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret can be difficult, expensive, time-consuming, and the outcome is unpredictable. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent the competitor from using that technology or information to compete with us and our competitive position would be harmed.
We may be subject to claims that our employees have wrongfully used or disclosed the alleged trade secrets of their former employers.
Many of our employees, including our senior management, were previously employed at other biotechnology or pharmaceutical companies, including our competitors or potential competitors. Some of these employees, including each member of our senior management, executed proprietary rights, non-disclosure and non-competition agreements in connection with such previous employment. Although we try to ensure that our employees do not use the proprietary information or know-how of others in their work for us, we may be subject to claims that we or these employees have used or disclosed intellectual property, including trade secrets or other proprietary information, of any such employee’s former employer. We are not aware of any threatened or pending claims related to these matters or concerning the agreements with our senior management, but in the future litigation may be necessary to defend against such claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, or personnel. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management.
Intellectual property rights do not necessarily protect us from all potential threats to our competitive advantages.
The degree of future protection afforded by our intellectual property rights is uncertain because intellectual property rights have limitations, and may not adequately protect our business, or permit us to maintain our competitive advantage. The following examples are illustrative:
| ● |
others may be able to make compounds that are similar to our drug candidates but that are not covered by the claims of the patents that we own or may in the future exclusively license; |
| ● |
we might not have been the first to make the inventions covered by the issued patents or pending patent applications that we own or may in the future exclusively license, which could result in the patent applications not issuing or being invalidated after issuing; |
| ● |
we might not have been the first to file patent applications covering certain of our inventions, which could prevent the issuance of the patent applications or cause them to be invalidated after issuance; |
| ● |
others may independently develop similar or alternative technologies or duplicate any of our technologies without infringing our intellectual property rights; |
| ● |
it is possible that our pending patent applications will not lead to issued patents; |
| ● |
issued patents that we own or have exclusively licensed may not provide us with any competitive advantages, or may be held invalid or unenforceable, as a result of legal challenges by our competitors; |
| ● |
we may obtain patents for certain drug candidates many years before we receive NDA approval for these drugs, and because patents have a limited life, which may begin to run prior to the commercial sale of the related drugs, limiting the commercial value of our patents; |
| ● |
our competitors might conduct research and development activities in countries where we do not have patent rights and then use the information learned from such activities to develop competitive drugs for commercialization in our major markets; |
| ● |
we may fail to develop additional proprietary technologies that are patentable; |
| ● |
we may fail to apply for or obtain adequate intellectual property protection in all the jurisdictions in which we operate; |
| ● |
the patents of others may have an adverse effect on our business, for example by preventing us from commercializing one or more of our drug candidates for one or more indications; and |
| ● |
any of the aforementioned threats to our competitive advantage could have a material adverse effect on our business. |
Risks Related to the Reverse Recapitalization and Integration of Businesses
We have incurred significant increased expenses and administrative burdens as a public company, which could have an adverse effect on our business, financial condition and results of operations.
As a public company, and particularly after we are no longer a smaller reporting company, we have faced and will continue to face increased legal, accounting, administrative and other costs and expenses as a public company that we did not incur as a private company. The Sarbanes-Oxley Act, including the requirements of Section 404, as well as rules and regulations subsequently implemented by the U.S. Securities and Exchange Commission (“SEC”), the Dodd-Frank Wall Street Reform and Consumer Protection Act of 2010 and the rules and regulations promulgated and to be promulgated thereunder, the Public Company Accounting Oversight Board and the securities exchanges, impose additional reporting and other obligations on public companies. Compliance with public company requirements has increased costs and made certain activities more time-consuming. A number of those requirements has required us to carry out activities we have not done previously. Our management and other personnel also have devoted and will continue to devote a substantial amount of time to these compliance initiatives. In addition, additional expenses associated with SEC reporting requirements have been incurred. Furthermore, if any issues in complying with those requirements are identified (for example, if the auditors identify a material weakness or significant deficiency in the internal control over financial reporting), we could incur additional costs rectifying those issues, and the existence of those issues could adversely affect our reputation or investor perceptions of it. It is also more expensive to obtain director and officer liability insurance. Risks associated with our status as a public company may make it more difficult to attract and retain qualified persons to serve on the board of directors or as executive officers. The additional reporting and other obligations imposed by these rules and regulations has increased legal and financial compliance costs and the costs of related legal, accounting and administrative activities. These increased costs require us to divert a significant amount of money that could otherwise be used to expand our business and achieve strategic objectives. Advocacy efforts by stockholders and third parties may also prompt additional changes in governance and reporting requirements, which could further increase costs.
We qualify as a smaller reporting company within the meaning of the Securities Act, and if we take advantage of certain exemptions from disclosure requirements available to smaller reporting companies, it could make our Common Stock less attractive to investors and may make it more difficult to compare our performance to the performance of other public companies.
We are a “smaller reporting company” because the market value of our stock held by non-affiliates was less than $250 million as of June 30, 2023. We may continue to be a smaller reporting company in any given year if either (i) the market value of our stock held by non-affiliates is less than $250 million as of June 30 in the most recently completed fiscal year or (ii) our annual revenue is less than $100 million during the most recently completed fiscal year and the market value of our stock held by non-affiliates is less than $700 million as of June 30 in the most recently completed fiscal year. As a smaller reporting company, we are eligible for and may take advantage of certain exemptions from various reporting requirements applicable to other public companies for as long as we continue to be a smaller reporting company, including: (i) the choice of presenting only the two most recent fiscal years of audited financial statements in our Annual Report on Form 10-K, (ii) the exemption from the auditor attestation requirements with respect to internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act, and (iii) reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements.
We cannot predict if investors will find our Common Stock less attractive because we rely on these exemptions. If some investors find our Common Stock less attractive as a result, there may be a less active trading market for our Common Stock and our stock price may be more volatile.
Risks Related to Our Common Stock
Provisions in our amended and restated certificate of incorporation and amended and restated bylaws could make a merger, tender offer or proxy contest difficult, thereby depressing the trading price of our Common Stock.
Provisions in our amended and restated certificate of incorporation and amended and restated bylaws may discourage, delay or prevent a merger, acquisition or other change in control that stockholders may consider favorable, including transactions in which stockholders might otherwise receive a premium for their shares of our Common Stock. These provisions could also limit the price that investors might be willing to pay in the future for shares of our Common Stock, thereby depressing the market price of our Common Stock. Such provisions include the following:
| ● |
a classified board of directors with three-year staggered terms, which could delay the ability of stockholders to change the membership of a majority of our Board; |
| ● |
the ability of our Board to approve the issuance shares of preferred stock and to determine the price and other terms of those shares, including preferences and voting rights, without stockholder approval, which could be used to significantly dilute the ownership of a hostile acquiror and/or existing stockholders; |
| ● |
the requirement for the affirmative vote of holders of at least 66⅔% of the voting power of all of the then-outstanding shares of the Common Stock, voting together as a single class, to amend certain provisions of our amended and restated certificate of incorporation or our amended and restated bylaws, which may inhibit the ability of an acquiror to effect such amendments to facilitate an unsolicited takeover attempt; |
| ● |
the exclusive right of our Board to elect a director to fill a vacancy created by the expansion of our Board or the resignation, retirement death, disqualification or removal of a director, which prevents stockholders from being able to fill vacancies on our Board for a period of time; and |
| ● |
the requirement that a special meeting of stockholders may be called only by our Board, the chairman of our Board or our Chief Executive Officer, which could delay the ability of our stockholders to force consideration of a proposal or to take action, including the removal of directors. |
These and other provisions in our amended and restated certificate of incorporation and amended and restated bylaws could make it more difficult for stockholders or potential acquirors to obtain control of our Board or initiate actions that are opposed by our then-current Board, including the ability to delay or impede a merger, tender offer or proxy contest. The existence of these provisions could negatively affect the price of our Common Stock and limit opportunities for stockholders to realize value in a corporate transaction.
Future offerings of debt or equity securities by us may adversely affect the market price of our Common Stock.
In the future, we may attempt to obtain financing or to further increase our capital resources by issuing additional shares of our Common Stock or offering debt or other equity securities, including commercial paper, medium-term notes, senior or subordinated notes, debt securities convertible into equity or shares of preferred stock. Future clinical trials, commercialization efforts, and acquisitions could require substantial additional capital in excess of cash from operations. We would expect to obtain the capital required for acquisitions through a combination of additional issuances of equity, corporate indebtedness and/or cash from operations.
Issuing additional shares of our Common Stock or other equity securities or securities convertible into equity may dilute the economic and voting rights of our existing stockholders or reduce the market price of our Common Stock or both. Upon liquidation, holders of such debt securities and preferred shares, if issued, and lenders with respect to other borrowings would receive a distribution of our available assets prior to the holders of our Common Stock. Debt securities convertible into equity could be subject to adjustments in the conversion ratio pursuant to which certain events may increase the number of equity securities issuable upon conversion. Preferred shares, if issued, could have a preference with respect to liquidating distributions or a preference with respect to dividend payments that could limit our ability to pay dividends to the holders of our Common Stock. Our decision to issue securities in any future offering will depend on market conditions and other factors beyond our control, which may adversely affect the amount, timing and nature of our future offerings.
General Risk Factors
We do not satisfy all continued listing requirements of Nasdaq. There can be no assurance that we will be able to comply with the continued listing requirements of Nasdaq.
As previously disclosed, on August 1, 2023, we received a written notice from Nasdaq that for the last 30 consecutive business days, the bid price for our Common Stock had closed below the minimum $1.00 per share requirement for continued listing on Nasdaq pursuant to Nasdaq Listing Rule 5550(a)(2) (the “Minimum Bid Price Requirement”). In accordance with Nasdaq Listing Rule 5810(c)(3)(A), the Company had a period of 180 calendar days, or until January 29, 2024, to regain compliance with the Minimum Bid Price Requirement. On January 30, 2024, the Company received a notice from Nasdaq that, while the Company has not regained compliance with the Minimum Bid Price Requirement, in accordance with Nasdaq Listing Rule 5810(c)(3)(A), it is eligible for an additional 180 calendar day period, or until July 29, 2024, to regain compliance with the Minimum Bid Price Requirement (the “January Notice”). The January Notice has no immediate effect on the listing of our Common Stock and our Common Stock will continue to be listed on Nasdaq under the symbol “CLNN.”
Nasdaq’s determination to grant us an additional 180 calendar day period to regain compliance is based on us meeting the continued listing requirement for market value of publicly held shares and all other applicable requirements for initial listing on Nasdaq, with the exception of the Minimum Bid Price Requirement, and on our written notice to Nasdaq on January 16, 2024 of our intention to cure the deficiency during the additional 180-day compliance period, including by effecting a reverse stock split, if necessary. If at any time during this additional 180-day compliance period, the bid price of our Common Stock closes at $1.00 per share or more for a minimum of 10 consecutive business days, Nasdaq will provide us with a written confirmation of compliance with the Minimum Bid Price Requirement. If we do not regain compliance with the Minimum Bid Price Requirement by July 29, 2024, Nasdaq will provide us written notification that our Common Stock will be delisted. At that time, we may appeal the delisting determination to a Nasdaq hearings panel.
We intend to actively monitor the bid price for our Common Stock between now and July 29, 2024, and will consider our available options to regain compliance with the Minimum Bid Price Requirement. There can be no assurance that we will regain compliance with the Minimum Bid Price Requirement or maintain compliance with any of the other Nasdaq continued listing requirements.
If Nasdaq delists our shares of Common Stock or warrants from trading on its exchange for failure to meet Nasdaq’s listing requirements, we and our stockholders could face significant material adverse consequences including:
| ● |
a limited availability of market quotations for our securities; |
| ● |
reduced liquidity for our securities; |
| ● |
a determination that our Common Stock is a “penny stock” which will require brokers trading in our Common Stock to adhere to more stringent rules and possibly result in a reduced level of trading activity in the secondary trading market for our securities; |
| ● |
a limited amount of news and analyst coverage; and |
| ● |
a decreased ability to issue additional securities or obtain additional financing in the future. |
The price of our Common Stock may be volatile.
The stock markets in general and the markets for biotechnology stocks have experienced extreme volatility. The market for the common stock of smaller companies such as ours is characterized by significant price volatility when compared to the shares of larger, more established companies that trade on a national securities exchange and have large public floats, and the share price of our Common Stock is more volatile than the price of the shares of such larger, more established companies and will continue to be for the indefinite future.
The price of our Common Stock may fluctuate due to a variety of factors, including:
| ● |
changes in the industries in which we operate; |
| ● |
variations in our operating performance and the performance of our competitors in general; |
| ● |
material and adverse impact of health epidemics or pandemics on the markets and the broader global economy; |
| ● |
actual or anticipated fluctuations in our quarterly or annual operating results; |
| ● |
publication of research reports by securities analysts about us or our competitors or our industry; |
| ● |
the public’s reaction to our press releases, our other public announcements and our filings with the SEC; |
| ● |
our failure or the failure of our competitors to meet analysts’ projections or guidance that we or our competitors may give to the market; |
| ● |
additions and departures of key personnel; |
| ● |
changes in laws and regulations affecting our business; |
| ● |
commencement of, or involvement in, litigation involving us; |
| ● |
changes in our capital structure, such as future issuances of securities or the incurrence of additional debt; |
| ● |
the volume of shares of our Common Stock available for public sale; and |
| ● |
general economic, political, industry, and market conditions such as recessions, interest rates, fuel prices, foreign currency fluctuations, international tariffs, social, political and economic risks, epidemics and pandemics, and acts of terrorism or war (such as the ongoing conflicts between Ukraine and Russia and Israel and Palestine). |
These market and industry factors may materially reduce the market price of our Common Stock regardless of our operating performance.
SEC regulations limit the amount of funds we can raise during any 12-month period pursuant to our shelf registration statement on Form S-3.
SEC regulations limit the amount that companies with a public float of less than $75 million may raise during any 12-month period pursuant to a shelf registration statement on Form S-3. Under General Instruction I.B.6 to Form S-3 (the “Baby Shelf Rule”), the amount of funds a company can raise through primary public offerings of securities in any 12-month period using a registration statement on Form S-3 pursuant to the Baby Shelf Rule is limited to one-third of the aggregate market value of its shares of common stock held by non-affiliates of the company. Currently, we are constrained by the Baby Shelf Rule. Even if sufficient funding is available, there can be no assurance that it will be available on terms acceptable to us or our stockholders. Furthermore, if we are required or choose to file a new registration statement on a form other than Form S-3, we may incur additional costs and be subject to delays due to review by the SEC staff.
Item 1B. Unresolved Staff Comments
Not applicable.
Overview
Information, unlike other assets such as cash, facilities, equipment, and products, is highly volatile in terms of its value and many people can use it simultaneously. It leaves no obvious indicators when it is stolen, and it is in constant motion across our internet, intranet, extranet, and computer systems. It is often stored in many locations in different formats at the same time. These characteristics make it much more difficult to manage, control, and protect than other types of assets and therefore a risk management process is required. Our cybersecurity policies and procedures have been developed to ensure an adequate and consistent approach to the management, control, and protection of our information (“Information Assets”). Our Information Assets include business information, customer information and external business partner information, including, without limitation, classified information, information relating to research, intellectual property, personally identifiable information, business and product development, clinical test and evaluation data, and business plans, customer and supplier information, supply chain, manufacturing, distribution, finance, human resources, consulting, partnerships, contracts, and corporate transactions, maintained in any form or format or location, including audio, video, paper, magnetic, electronic and optical. Information Assets may be classified as Low, Medium, or High Risk based on the potential impact of its unauthorized disclosure.
Device and Network Security
Our device and network security policies and procedures are designed to mitigate risk by ensuring our network and computing devices (“Computer Equipment”), electronic systems, and resources used in our business (“Information Systems”), whether owned or leased by us, our employees, or third parties, and the Information Assets contained therein, are protected from security threats.
To mitigate risk, we utilize (i) firewalls to protect our network perimeter and additional perimeters within the network as required, (ii) anti-malware software to protect all Computer Equipment, including but not limited to desktops, laptops, workstations, and servers, (iii) device scanning, alerts, and reporting, (iv) physical security, (v) security and application lifecycle security, (vi) security updates and backups, and (vii) vulnerability and risk assessments.
Firewalls. Our network and Computer Equipment is protected by one or more authorized firewalls, with any changes to firewall hardware, operating system, or rules requiring approval from authorized personnel including the review and approval of an IT change control document. Administration of firewalls is restricted to a minimum number of authorized personnel as necessary. We also employ intrusion detection at critical points of our network. All external access to our network, or to any computing resource on our network connected to a non-Clene network (including, but not limited to the internet) must pass through a hardware firewall, appliance, or equivalent device, where all traffic between our network and external networks can be continuously controlled, monitored, and examined for any access violations.
Anti-Malware Software. Our Computer Equipment is protected by anti-malware software. The management and administration of anti-malware software is restricted to a minimum number of authorized personnel as necessary.
Real-Time Monitoring. We engage a third-party security operations center that actively monitors our environment and detects and remediates security threats in real-time.
Device Scanning, Alerts, and Reporting. We reserve the right to monitor, scan, screen, and quarantine/confiscate all Computer Equipment that accesses our network, in compliance with applicable laws and government regulations. We also reserve the right to scan information systems, monitor or screen content and traffic patterns, block e-mail, quarantine and/or confiscate any Information Systems that may post a threat to us, and if such activities reveal possible evidence of criminal activity, to take any appropriate action which may include providing evidence to law enforcement officials.
Physical Security. We control physical access to our facilities, areas within our facilities, data centers, server rooms, and equipment. Manufacturing and research and development is conducted out of our Maryland facility that employs badging, visitor registries, escorts for visitors, exit/removal procedures, and physical locks/access controls as appropriate and necessary. Our corporate office in Utah is equipped with physical security including locks/access controls to the facility and to secure all IT-related equipment and personnel files. Installation, maintenance, and repair of equipment is restricted to authorized personnel. We protect our Computer Equipment from power failure, surges, and other electrical anomalies, and cabling is protected from unauthorized access or damage. Access to our network services is restricted to authorized individuals and granted only following individual identification and authentication. Local wireless access is limited to authorized entry points, with various forms of authentication required before access is granted to authorized individuals.
Security and Application Lifecycle Security. We perform analysis of security requirements for all systems and applications throughout their lifecycle, including for new systems and applications and significant upgrades to existing systems and applications. All new or upgraded systems and applications are tested for stability, compatibility, and security integrity in a separate environment prior to introduction into our production environment.
Security Updates and Backups. We monitor security bulletins, software updates/patches, and functional software updates/patches and apply them in accordance with the timeline prescribed in our policies and based upon recommendations from third-party vendors, as applicable. Systems that no longer provide security updates/patches are discontinued. We research, test, and verify functional software updates/patches before installation. We perform data backups periodically based on business requirements to maximize data availability and prevent information loss, including before any system upgrade or maintenance. Encrypted data remains encrypted throughout our backup processes. We review backup schedules at least annually, and changes may only be made by authorized personnel after formal documentation and approval. Data backups are stored in geographically separate facilities.
Vulnerability Assessments. We conduct assessments over potential vulnerabilities for all new and existing network-connected assets on an annual basis. Any potential vulnerabilities that we identify are remediated. We rate vulnerabilities based on the following criteria: (i) High: A vulnerability exists that could potentially allow an attacker to gain elevated access of the host, divulge system information, and/or lead to system or network compromise; (ii) Medium: A vulnerability exists that could potentially allow an attacker limited access to file contents, security settings or ability to conduct a denial-of-service attack; (iii) Low: A vulnerability exists that could potentially allow an attacker limited access to sensitive host system data, such as installed software version giving the ability to exploit application vulnerabilities; and (iv) Info: An attacker could collect basic host information such as open ports and services.
Security Incident Reporting
Our security incident reporting policy and procedures enable the identification, monitoring, reporting, and response capabilities to known or suspected security incidents in our network and all IT-managed services and Information Systems. Security identification begins with a broad range of potential risks, including, but not limited to, theft or unauthorized disclosure of Information Assets, unexpected modification of Company Information Assets, disruptions of service that can result in Information Assets being unavailable for an unacceptable amount of time, and suspicious behavior and/or unauthorized activity by any individual or organization that can potentially compromise Information Assets or Information Systems.
Our process to monitor, report, and respond to identified or suspected security incidents includes (i) collection of relevant information about an incident, including (a) impacted systems, (b) impacted entities, (c) protection mechanisms that were in place and active at the time of the security incident, (d) audit logs, and (e) the risk classification of the Information Assets that were potentially impacted; (ii) reporting to a centralized ticketing system; (iii) reporting to management and other authorities, such as legal, human resources, IT, and local and/or state law enforcement, etc.; (iv) escalation, if the incident is considered to be critical based upon our assessment of its potential impact, to appropriate management and directors and other authorities; and (v) documentation of the incident and our response actions taken.
Change and Configuration Management
Our change and configuration management policy and procedures enable the effective management of changes to Information Systems (“Changes”) to ensure the confidentiality and integrity of Information Assets and the continued availability of both the Information Systems and information technology (“IT”) services. The policies and procedures apply to all changes to Information Systems managed by the Company or its IT external business partners.
Changes must be approved by authorized personnel prior to (i) performance of any work related to a Change, (ii) migration of any Change-related work from the quality environment to the production environment, to ensure the Change was adequately tested and performs properly, and (iii) closing of the Change, to ensure the Change was implemented in the production environment and correctly solves the issue that prompted the Change request.
Changes are tracked and documented in a change tracking system, and we retain past versions of source components and supporting documentation. Testing is performed in an environment other than the production environment, and user acceptance testing is performed by an independent person not responsible for development, modification, or configuration of applications, programs, or system code. Errors are identified, logged, and resolved.
Additionally, for Changes that may impact our manufacturing process, we perform impact assessments prior to performing a Change to understand the (i) level of financial, technical, and compliance risk, (ii) impact on business operations, (iii) impact of configuration and user access security, (iv) impact on connected Information Systems and interfaces, and (v) need for user training. The extent and documentation of impact assessments are commensurate with the level of risk associated with the Change, and the level of testing performed shall be determined by the results of the impact assessment.
Identity and Access Management
Our identity and access management policies and procedures define the access control measures to our Information Systems to protect the privacy, security, and confidentiality of Computer Equipment, Information Systems, and Information Assets.
Unique identification is assigned to all individuals with a defined relationship (e.g., employees, vendors, suppliers, etc.), and if a relationship changes, a new identifier is created to reflect the new relationship. Passwords must be changed upon first logon and all privileged account passwords (e.g., root, super user, and administrator passwords) must follow our password guidelines. Identification and authentication are required every time Medium or High Risk Information Assets are accessed or elevated privileges are exercised, and use of elevated privileges is temporary and is revoked upon implementation of a change.
Our data access procedures require completion and authorization of access request forms to request, change, or delete access privileges to Information Systems containing Medium or High Risk Information Assets. We perform checks for segregation of duties conflicts and only grant the minimum necessary and least privilege access to users based upon their role. When users are reassigned, promoted, or separated, their access privileges are reviewed and, if necessary, updated in a timely manner. We also perform periodic reviews of user privileges and require training for users with access to Medium or High Risk Information Assets.
Information Asset Protection
Our Information Asset protection policy and procedures enables the management, control, and protection of Information Assets from unauthorized disclosure, theft, loss, destruction, unauthorized alteration, unauthorized access, and the denial of availability, all of which could have a direct and significant impact on the future success of the Company. Protection of Information Asset supports the efficient and effective management, control, and protection of our business information and the business information entrusted to us by our customers and external business partners. All Information Asset protection policies and procedures must also be viewed in the context of our obligations to comply with government requirements, such as those related to the protection of personal data, and compliance with our contractual obligations.
We use the following approach to manage risks related to Information Asset protection: (i) identification and classification of Information Assets, (ii) identification and assessment of the threats to those Information Assets and the associated risk based upon impact to the business and the likelihood of their occurrence, (iii) assessment and analysis of risk, and determination of the actions required to lower risks to an acceptable level, (iv) implementation of appropriate controls or management acknowledgment or risk where controls cannot be implemented, (v) continuous monitoring and measuring of risk, (vi) ongoing communication of risks and mitigating actions, and (vii) auditing for compliance.
Once a risk is identified, we analyze the risk and assign a risk classification based upon a combination of factors, including data volume, legal and regulatory requirements, privacy considerations, and intellectual property considerations. Risks are classified as (i) Low Risk, where unauthorized disclosure could be expected to have a limited adverse effect on operations, assets, or individuals; (2) Medium Risk, where unauthorized disclosure could be expected to have a serious adverse effect on operations, assets, or individuals; or (3) High Risk, where unauthorized disclosure could be expected to have a severe or catastrophic adverse effect on operations, assets, or individuals.
Prior to the close of 2024, we intend to implement automated system restrictions over Information Assets that will permit general use of Low Risk Information Assets both internally and by our external business partners, and will restrict access to Medium and High Risk Information Assets to limited audiences with legitimate business purposes or specific job responsibilities. Additionally, we currently use confidentiality agreements before granting access as determined by relationship of the user and the associated risks of the Information Asset, and we periodically review access rights to ensure compliance and prevent unauthorized access.
Governance
Assessing, identifying, and managing cybersecurity related risks are integrated into our overall risk management program. Our Chief Executive Officer, General Counsel, and Vice President of Quality and Technical Operations directly oversee the development, implementation, operation, and revision of our cybersecurity policies and procedures, and are primarily responsible for the oversight of risks from cybersecurity threats and any security incidents that may occur. These officers have more than 21 years of combined experience in managing IT, operations, and information risk and security. Our Vice President of Quality and Technical Operations has experience developing comprehensive information security programs for organizations, and brings extensive experience in the private sector and is a specialist in IT governance strategies, risk management protocols, and compliance frameworks. All security incidents are managed by our Vice President of Quality and Technical Operations and reported to management, including our Chief Executive Officer, General Counsel, and other personnel based upon the specifics of the incident and its impact. Additionally, if a known or suspected security incident occurs at the Company, based upon its risk classification and if we assess the impact to be critical, the incident is escalated in a timely manner to the Audit Committee of the Board of Directors for oversight of the monitoring, reporting, and response process. The Audit Committee also oversees the implementation of our policies and procedures to prevent or reduce cybersecurity risks on an ongoing basis during the performance of its general committee duties.
We face a number of cybersecurity risks in connection with our business and have from time-to-time experienced cybersecurity incidents, which to date have not had a material impact on our financial condition or results of operations. For more information about the cybersecurity risks we face, see Item 1A—Risk Factors “Our internal computer systems, or those used by any CROs or other third-party contractors or consultants we may engage, may fail or suffer security breaches.”
To date, we do not have any owned properties. We have leased a number of properties from independent third parties in the U.S. Our leased Salt Lake City headquarters is utilized for finance, clinical development, clinical operations, translational medicine, and business operations. Our leased North East, Maryland facility is utilized for manufacturing and research and development activities. Our leased Elkton, Maryland facility will be utilized to increase our manufacturing capability. We believe that our facilities are suitable and adequate for present purposes and that our productive capacity is substantially being utilized.
The following summary sets forth the details of our leased properties:
| ● |
EOS at Millrock Park, LLC (Salt Lake City, Utah)—approximately 5,028 square feet, expiring April 2027 with an option to extend thereafter. |
| ● |
Upper Chesapeake Flex One, LLC (North East, Maryland)—approximately 32,603 square feet, expiring January 2029 with an option to extend thereafter. |
| ● |
100 Chesapeake Blvd LLC (Elkton, Maryland)—approximately 74,210 square feet, expiring August 2031 with an option to extend thereafter and a purchase option at the expiration of the seventh year. |
We are not currently a party to any material legal proceedings. From time to time, we may, however, be involved in legal proceedings in the ordinary course of business. We cannot predict the outcome of any such legal proceedings, and despite the potential outcomes, the existence thereof may have an adverse impact on us because of defense and settlement costs, diversion of management resources and other factors. As of the date of this Annual Report, we are not aware of any pending or threatened litigation or administrative proceedings against us, our officers or our directors which may have a material and adverse impact on our business, financial condition or results of operations.
Item 4. Mine Safety Disclosures
Not Applicable.
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
Market Information
Our Common Stock and publicly-traded warrants are traded on Nasdaq under the symbols “CLNN” and “CLNNW,” respectively.
Holders
As of March 8, 2024, there were 128,430,098 issued and outstanding shares of our Common Stock held by 65 stockholders of record. The number of stockholders of record was determined from the records of our transfer agent and does not include beneficial owners whose shares are held in the names of various security brokers, dealers, and registered clearing agencies.
Dividends
We intend to retain all available funds and any future earnings to finance the growth and development of our business. We have never declared or paid cash dividends on our Common Stock, and we do not intend to pay cash dividends in the foreseeable future. Our ability to declare dividends is limited by the terms of financing or other agreements that we have entered into. Future debt or other financing arrangements also may contain terms prohibiting or limiting the amount of dividends that may be declared or paid on our Common Stock. Investors should not purchase our Common Stock with the expectation of receiving cash dividends.
Any future determination to declare dividends will be made at the discretion of our Board and will depend on our financial condition, results of operations, capital requirements, general business conditions, and other factors that our Board may deem relevant.
Recent Sales of Unregistered Securities
None.
Purchases of Equity Securities by the Issuer and Affiliated Purchasers
None.
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The following discussion and analysis of our financial condition and results of operations should be read in conjunction with our consolidated financial statements and related notes included elsewhere in this Annual Report on Form 10-K. This discussion contains forward-looking statements reflecting our or our management team's expectations, hopes, beliefs, intentions, strategies, estimates, and assumptions concerning events and financial trends that may affect our future financial condition or results of operations. Actual results and the timing of events may differ materially from those contained in these forward-looking statements due to a number of factors, including those discussed in the sections titled “Cautionary Note Regarding Forward-Looking Statements” and “Risk Factors” appearing elsewhere in this Annual Report on Form 10-K. Unless the context otherwise requires, for purposes of this section, the terms “we,” “us,” the “Company” or “our” are intended to mean the business and operations of Clene Inc. and its consolidated subsidiaries.
Business Overview
We are a clinical-stage pharmaceutical company pioneering the discovery, development, and commercialization of novel clean-surfaced nanotechnology (“CSN®”) therapeutics. CSN® therapeutics are comprised of atoms of transition elements that, when assembled in nanocrystal form, possess unusually high, unique catalytic activities not present in those same elements in bulk form. These catalytic activities drive, support, and maintain beneficial metabolic and energetic cellular reactions within diseased, stressed, and damaged cells.
Our patent-protected, proprietary position affords us the potential to develop a broad and deep pipeline of novel CSN therapeutics to address a range of diseases with high impact on human health. We innovated an electro-crystal-chemistry drug development platform that draws from advances in nanotechnology, plasma and quantum physics, material science, and biochemistry. Our platform process results in nanocrystals with faceted structures and surfaces that are free of the chemical surface modifications that accompany other production methods. Many traditional methods of nanoparticle synthesis involve the unavoidable deposition of potentially toxic organic residues and stabilizing surfactants on the particle surfaces. Synthesizing stable nanocrystals that are both nontoxic and highly catalytic has overcome this significant hurdle in harnessing transition metal catalytic activity for therapeutic use. Our clean-surfaced nanocrystals exhibit catalytic activities many-fold higher than multiple other commercially available nanoparticles, produced using various techniques, that we have comparatively evaluated.
We have multiple drug assets currently in development and/or clinical trials for applications primarily in neurology. Our development and clinical efforts are currently focused on addressing the high unmet medical needs in central nervous system disorders including amyotrophic lateral sclerosis (“ALS”), multiple sclerosis (“MS”), and Parkinson’s disease (“PD”). We currently have no drugs approved for commercial sale and have not generated any revenue from drug sales. We have never been profitable and have incurred operating losses in each year since inception. We generate revenue from sales of dietary supplements through our wholly owned subsidiary, dOrbital, Inc., or through an exclusive license with 4Life Research LLC (“4Life”), an international supplier of health supplements, stockholder, and related party. We anticipate these revenues to be small compared to our operating expenses and to the revenue we expect to generate from potential future sales of our drug candidates, for which we are currently conducting clinical trials.
Reverse Recapitalization
Clene Nanomedicine, Inc. (“Clene Nanomedicine”) became a public company on December 30, 2020 (the “Closing Date”) when it completed a reverse recapitalization (the “Reverse Recapitalization”) with Tottenham Acquisition I Limited (“Tottenham”), and with Tottenham’s wholly-owned subsidiary and our predecessor, Chelsea Worldwide Inc., and Creative Worldwide Inc., a wholly-owned subsidiary of Chelsea Worldwide Inc. On the Closing Date, Chelsea Worldwide Inc. changed its name to Clene Inc. and listed its shares of common stock, par value $0.0001 per share (“Common Stock”) on the Nasdaq Capital Market (“Nasdaq”) under the symbol “CLNN.”
In connection with the Reverse Recapitalization, certain of Clene Nanomedicine’s common stockholders are entitled to receive earn-out payments (the “Clene Nanomedicine Contingent Earn-out”), and Tottenham’s former officers and directors and Norwich Investment Limited (collectively, the “Initial Stockholders”) are entitled to receive earn-out payments (the “Initial Stockholders Contingent Earn-out,” and both collectively the “Contingent Earn-outs”) based on achieving certain milestones.
Recent Developments of Our Clinical Programs
Amyotrophic Lateral Sclerosis
In December 2023, we announced a statistically significant reduction of plasma neurofilament light chain (“NfL”) levels in the Phase 2 HEALEY ALS Platform Trial from baseline to 76 weeks in patients randomized to CNM-Au8 30 mg compared to patients treated with placebo for 24 weeks prior to crossing over to CNM-Au8 treatment. CNM-Au8 30 mg treatment reduced plasma NfL levels compared to baseline using a mixed model with repeat measures (“MMRM”), least squares (“LS”) mean change of the natural logarithm (“Ln”) of the plasma NfL values with the standard error (“SE”) for the 76-week change from baseline of plasma NfL: CNM-Au8 = -0.075 (SE: 0.053); placebo = +0.098 (SE: 0.056); CNM-Au8 30 mg versus original placebo difference = -0.173 (SE: 0.076), p=0.023. Combined analyses of both CNM-Au8 doses (30 mg and 60 mg) also demonstrated nominally significant reductions in plasma NfL, CNM-Au8 versus placebo difference = -0.144 (SE: 0.066), p=0.029. We also announced the results of long-term survival analyses under the prespecified rank-preserving structural failure time model (“RPSFTM”) to account for the effects of CNM-Au8 in participants randomized to placebo who crossed-over to treatment with CNM-Au8. Under an assumption of a constant common treatment effect from CNM-Au8, treatment with CNM-Au8 demonstrated a 60% decreased risk of long-term all-cause mortality in participants originally randomized to treatment with CNM-Au8 compared to those originally randomized to placebo, after adjusting for the estimated benefit received after switching to CNM-Au8 (Cox hazard ratio=0.40, 95% CI: 0.19 to 0.85; p=0.017). CNM-Au8 was well-tolerated, and no drug-related serious adverse events or significant safety findings were reported. We also continue to support two Expanded Access Programs (“EAPs”) with the Sean M. Healey & AMG Center for ALS.
In February 2024, we announced results from two independent analyses of the pooled EAP data for CNM-Au8 30 mg compared to two independent datasets derived from PRO-ACT and the ALS/MND Natural History Consortium. The EAP dataset as of the date of the analyses was comprised of 256 participants with ALS of which 220 EAP participants had all baseline values available for matching. These participants were matched for similar baseline characteristics compared to each non-CNM-Au8 treated control. The results in the EAP participants versus the matched controls demonstrated a significant survival benefit for each comparison:
| ● |
CNM-Au8 EAP vs. PRO-ACT matched controls: the baseline risk-adjusted hazard ratio demonstrated a 68% decreased risk of all-cause mortality with CNM-Au8 treatment (hazard ratio=0.320, 95% CI: 0.178 to 0.575, p=0.0001). |
| ● |
CNM-Au8 EAP vs. ALS/MND Natural History Consortium matched controls: the baseline risk-adjusted hazard ratio demonstrated a 57% decreased risk of all-cause mortality with CNM-Au8 treatment (hazard ratio=0.433, 95% CI: 0.282 to 0.663, p=0.0001). |
Analyses of the full dataset of 256 participants compared to the 220 matched controls also showed statistically significant survival benefits with log-rank p-values of p<0.0001 and p=0.006 for the PRO-ACT and ALS/MND Natural History Consortium matched controls, respectively.
We are presently planning the design of an international Phase 3 study of CNM-Au8 30 mg, RESTORE-ALS, with expert ALS clinical advisors and expect to initiate the trial in the second half of 2024, contingent upon funding. We plan to work closely with regulatory health authorities from the U.S. Food and Drug Administration (“FDA”), European Medicines Agency (“EMA”), ALS experts, and patient representatives to determine the proper path to support potential approval.
Additionally, we met with the FDA in the fourth quarter of 2023 and presented initial clinical and NfL biomarker results from our completed Phase 2 trials. We also presented the evidence of long-term survival data from these studies as well as the supportive safety data of more than 500 years of participant exposure to date without any identified safety signals (across ALS, MS, and PD). The FDA determined that the initial findings on biomarker NfL reduction from the Phase 2 trials were insufficient to support accelerated approval at that time. We are planning to provide supplemental data for further engagement with the FDA in the first half of 2024, including additional long-term clinical evidence and biomarker results of CNM-Au8’s treatment benefit in people living with ALS. We plan to demonstrate how CNM-Au8’s mechanism of action is linked to the reduction in NfL, and the association between observed NfL reductions and improved clinical outcomes in ALS patients, including increased survival time. We do not know when or if we will be able to file a New Drug Application (“NDA”) with the FDA which would be based on the outcome of our future meetings with the FDA and our accumulation of clinical evidence.
Multiple Sclerosis
In January 2024, we announced results from the open-label long-term extension (“LTE”) for the mITT population of our Phase 2 VISIONARY-MS clinical trial. The LS mean difference (SE) at week 144 for low contrast letter acuity (“LCLA”) change across both eyes versus the original randomization baseline of participants assigned to CNM-Au8 was: +8.70 letters (1.88), 95% CI: 5.0 to 12.4, p<0.0001; the LCLA LS squared mean difference (SE) versus the end of the double-blind period was: +4.0 letters (1.67), 95% CI: 0.72 to 7.30, p=0.017. Low contrast vision demonstrated sustained improvement by up to 38 letters across both eyes in individual participants, which represents multiple row gains on a greyed-out MS eye chart. The LS mean difference (SE) at week 144 for Symbol Digit Modalities Test (“SDMT”) change versus the original randomization baseline of participants assigned to CNM-Au8 was: +8.03 (1.52), 95% CI: 5.01 to 11.0, p<0.0001; the SDMT LS mean difference (SE) versus the end of the double-blind period was: +3.11 (1.3), 95% CI: 0.55 to 5.68, p=0.018. Cognitive improvement, particularly working memory and information processing speed, was improved by up to 35 points in individual participants, where a three-point change in cognitive processing speed has been deemed notable in other MS studies. Additionally, improvements demonstrated during the 48-week double-blind period were maintained in the LTE for the Timed 25-foot Walk (“T25FWT,” gait) and 9-Hole Peg Test (“9HPT,” upper extremity function). Placebo participants who transitioned to CNM-Au8 during the LTE showed significant improvements versus original baseline in LCLA and SDMT that were generally consistent with the increases observed in participants originally randomized to CNM-Au8.
We have initiated a second dosing cohort of REPAIR-MS, an open-label, investigator blinded Phase 2 clinical trial in non-active progressive MS patients. We anticipate enrollment concluding in the first half of 2024 with topline results available by the end of 2024. We plan to work closely with regulatory health authorities from the FDA and EMA, MS experts, and patient representatives to determine the proper path to advance CNM-Au8 into Phase 3 and potential future approval. We expect to meet with the FDA in an end of Phase 2 meeting in the second half of 2024.
The chart below reflects the growing body of evidence for CSN therapeutics from our completed and ongoing clinical programs.
Recent Competition Update
Despite the great need for an effective disease-modifying treatment for ALS and significant research efforts by the pharmaceutical industry to meet this need, there have been limited clinical successes and no curative therapies approved to date. Recently, in April 2023, the FDA granted accelerated approval to tofersen, branded as Qalsody, a drug from Biogen Inc. for the treatment of SOD1-ALS. A marketing authorization application for tofersen is currently under review by the EMA. Additionally, sodium phenylbutyrate and taurursodiol, a drug from Amylyx Pharmaceuticals, Inc. (“Amylyx”) for the treatment of ALS, previously received approval from the FDA and conditional approval from Health Canada based on the results of a Phase 2 trial. In January 2024, the European Commission refused the marketing authorization for sodium phenylbutyrate and taurursodiol, and in March 2024 Amylyx announced the results of a Phase 3 trial which did not demonstrate a statistically significant treatment benefit as measured by the ALSFRS-R score and quality of life patient-reported outcome assessments, including overall survival and respiratory function. Amylyx has voluntarily paused promotion of sodium phenylbutyrate and taurursodiol, with anticipated future engagement with regulatory authorities and the potential voluntarily withdrawal of the drug from the market.
Financial Overview
Our financial condition, results of operations, and the period-to-period comparability of our financial results are principally affected by the following factors:
Research and Development Expense
The discovery and development of novel drug candidates require a significant investment of resources over a prolonged period of time, and a core part of our strategy is to continue making sustained investments in this area. As a result of this commitment, our pipeline of drug candidates has been advancing, with substantially all our research and development expenses relating to CNM-Au8, our lead asset, with the remainder spent on our CNM-ZnAg asset.
Our research and development expenses are affected by the scope and advancement of our existing product pipeline and the commencement of new drug programs. Drug candidates in later stages of clinical development generally have higher development costs than those in earlier stages, primarily due to costs and fees for per patient clinical trial sites for larger clinical trials, opening and monitoring clinical sites, contract research organization (“CRO”) activity, and manufacturing. We anticipate that our research and development expenses will decrease in early 2024 due to the completion of many of our ongoing clinical trials but will increase throughout 2024 and into future years as we advance our assets into Phase 3. Additionally, if we are able to file an NDA under an accelerated pathway with the FDA, contingent upon our discussions with the FDA regarding our accumulation of clinical evidence which is expected in the first half of 2024, we anticipate that our research and development expenses related to regulatory activities would increase in advance of receiving regulatory approval. If we are unable to file an NDA under an accelerated pathway, we would need to continue investing in clinical research activities and we anticipate that our research and development expenses would increase in future periods as we advance our assets in Phase 3.
Research and development costs consist primarily of payroll and personnel expenses for salaries, benefits, and stock-based compensation; supplies and materials expenses to support our clinical trials; payments to CROs, principal investigators, and clinical trial sites; costs of preclinical activities; consulting costs; and allocated overhead costs, including rent, equipment, utilities, depreciation, insurance, and facilities maintenance. Research and development costs are charged to operations as incurred, and nonrefundable advance payments related to future research and development activities are initially recorded as assets and are expensed when we receive the related goods or services.
Our clinical trial accrual process seeks to account for expenses resulting from obligations under contracts with CROs, consultants, and clinical sites in connection with conducting clinical trials. The financial terms of these contracts vary and may result in payment flows that do not match the periods over which materials or services are provided to us under such contracts. We reflect the appropriate clinical trial expenses in the consolidated financial statements by matching the appropriate expenses with the period in which services are performed. In the event advance payments are made to CROs, the payments are recorded as prepaid assets and expensed over the period in which services are performed.
General and Administrative Expense
General and administrative expenses consist primarily of payroll and personnel expenses for salaries, benefits, and stock-based compensation; fees for legal, accounting, tax, and information technology services; fees for directors’ and officers’ insurance; expenses for business development activities and investor and public relations; rent, utilities, and facility costs; travel costs; and consulting fees.
We anticipate that our general and administrative expenses in future periods will be contingent upon our discussions with the FDA, expected in the first half of 2024. If we are able to file an NDA with the FDA based on our accumulation of clinical evidence, we anticipate our general and administrative expenses would increase in future periods to support increases in our drug development activities and as we build our commercial capabilities in advance of receiving regulatory approval. This potential increase will likely include increased headcount, increased stock compensation expenses, expanded infrastructure including certain sales and marketing activities performed ahead of regulatory approval, and increased insurance expenses. If we are unable to file an NDA based on our FDA interaction, we would need to continue investing in clinical research activities and we anticipate our general and administrative expenses would decrease in future periods as we decrease commercial expansion projects, including at our Elkton, Maryland facility, and as we implement cost-saving initiatives, such as a reduction in compensation, a hiring freeze, and elimination of certain staff positions.
Total Other Income (Expense), Net
Total other income (expense), net, consists primarily of (i) interest income and interest expense, (ii) gains and losses on termination of leases, (iii) commitment share expense from shares of Common Stock issued as a commitment fee, (iv) issuance costs allocated to liability-classified warrants, (v) a loss on initial issuance of equity from the fair value in excess of proceeds from a public equity offering, (vi) changes in the fair value of our (a) common stock warrant liabilities and (b) Contingent Earn-outs, (vii) research and development tax credits, unconditional grants, and conditional grants for which applicable conditions have been met, and (viii) realized gains and losses on foreign currency transactions and other miscellaneous income and expense items.
Results of Operations
Our results of operations for the years ended December 31, 2023 and 2022 were as follows:
| Year Ended December 31, |
||||||||||||
| (in thousands) |
2023 |
2022 |
Change |
|||||||||
| Revenue: |
||||||||||||
| Product revenue |
$ | 498 | $ | 329 | 51 | % | ||||||
| Royalty revenue |
156 | 144 | 8 | % | ||||||||
| Total revenue |
654 | 473 | 38 | % | ||||||||
| Operating expenses: |
||||||||||||
| Cost of revenue |
121 | 26 | 365 | % | ||||||||
| Research and development |
26,655 | 31,920 | (16 | )% | ||||||||
| General and administrative |
14,418 | 16,936 | (15 | )% | ||||||||
| Total operating expenses |
41,194 | 48,882 | (16 | )% | ||||||||
| Loss from operations |
(40,540 | ) | (48,409 | ) | (16 | )% | ||||||
| Total other income (expense), net |
(8,964 | ) | 18,491 | * | ||||||||
| Net loss |
$ | (49,504 | ) | $ | (29,918 | ) | 65 | % | ||||
Revenue
Product revenue relates to our dietary supplement products and consists of (i) sales of an aqueous zinc-silver ion dietary (mineral) supplement sold by our wholly-owned subsidiary, dOrbital, Inc., under the trade name “rMetx™ ZnAg Immune Boost,” or under a supply agreement with 4Life under the trade name “Zinc Factor™,” and (ii) sales of KHC46, an aqueous gold dietary (mineral) supplement of very low-concentration, sold under a supply agreement with 4Life under the trade name “Gold Factor™.” Royalty revenue relates to our dietary supplement products and consists of proceeds under an exclusive and royalty-bearing license agreement with 4Life relating to the sale of Gold Factor. During the years ended December 31, 2023 and 2022, changes in product and royalty revenues were due to the timing of purchases of Zinc Factor and Gold Factor by 4Life under the supply and license agreements.
Cost of Revenue
Cost of revenue related to production and distribution costs for the sales of Gold Factor, Zinc Factor, and rMetx dietary supplements.
Research and Development Expense
Research and development expense for the years ended December 31, 2023 and 2022 was as follows:
| Year Ended December 31, |
||||||||||||
| (in thousands) |
2023 |
2022 |
Change |
|||||||||
| CNM-Au8 |
$ | 6,795 | $ | 10,439 | (35 | )% | ||||||
| CNM-ZnAg |
682 | 2,662 | (74 | )% | ||||||||
| Unallocated |
5,572 | 5,698 | (2 | )% | ||||||||
| Personnel |
9,545 | 9,856 | (3 | )% | ||||||||
| Stock-based compensation |
4,061 | 3,265 | 24 | % | ||||||||
| Total research and development |
$ | 26,655 | $ | 31,920 | (16 | )% | ||||||
The change in research and development expenses was primarily due to the following:
| (i) | a decrease in expenses related to our lead drug candidate, CNM-Au8, primarily due to a decrease in expenses in the HEALEY ALS Platform Trial and our RESCUE-ALS, REPAIR-MS, REPAIR-PD, and VISIONARY-MS clinical trials due to completion of the blinded period of each trial and decreased CRO and clinical operations expenses; and a decrease in expenses related to non-clinical and pre-clinical activities; partially offset by an increase in expenses related to our two ongoing EAPs due to increased enrollment and expansion of one EAP; increased expenses related to the LTE for VISIONARY-MS; and an increase in expenses related to regulatory activities; |
| (ii) | a decrease in expenses related to CNM-ZnAg, primarily due to completion of the clinical trial for treatment of COVID-19 in 2022, and the renegotiation of our CRO fees during the year ended December 31, 2023; |
| (iii) | a decrease in unallocated expenses, primarily due to decreased research, manufacturing, equipment, and materials expenses; partially offset by increased rent, utility, and depreciation expenses due to our leased facility in Elkton, Maryland and our expanded facility in North East, Maryland; |
| (iv) | a decrease in personnel expenses, primarily due to a reduction in headcount during the fourth quarter of 2022, partially offset by increased employee compensation during the second half of 2023; and |
| (v) | an increase in stock-based compensation expense, primarily due to the timing of award grants, vesting, and forfeitures for research and development personnel, partially offset by our decreased headcount and corresponding stock-based compensation expense during 2023. |
General and Administrative Expenses
General and administrative expense for the years ended December 31, 2023 and 2022 was as follows:
| Year Ended December 31, |
||||||||||||
| (in thousands) |
2023 |
2022 |
Change |
|||||||||
| Directors’ and officersʼ insurance |
$ | 1,593 | $ | 3,395 | (53 | )% | ||||||
| Legal |
404 | 557 | (27 | )% | ||||||||
| Finance and accounting |
1,317 | 773 | 70 | % | ||||||||
| Public and investor relations |
614 | 927 | (34 | )% | ||||||||
| Personnel |
4,239 | 4,649 | (9 | )% | ||||||||
| Stock-based compensation |
5,056 | 5,248 | (4 | )% | ||||||||
| Other |
1,195 | 1,387 | (14 | )% | ||||||||
| Total general and administrative |
$ | 14,418 | $ | 16,936 | (15 | )% | ||||||
The change in general and administrative expense was primarily due to the following:
| (i) | a decrease in directors’ and officers’ insurance fees; |
| (ii) | a decrease in legal fees, primarily due to a decrease in general corporate legal fees, intellectual property fees, and legal fees related to financing and fundraising; |
| (iii) | an increase in finance and accounting fees, primarily due to increased fees from auditors, consultants, advisors, and other financial vendors, partially offset by decreased tax fees; |
| (iv) | a decrease in fees related to our public and investor relations efforts; |
| (v) | a decrease in personnel expenses, primarily due to a reduction in headcount during the fourth quarter of 2022, partially offset by increased employee compensation during the second half of 2023; |
| (vi) | a decrease in stock-based compensation expense, primarily due to the timing of award grants, vesting, and forfeitures for general and administrative personnel, and our decreased headcount during 2023; and |
| (vii) | a decrease in other expenses, primarily due to a decrease in expenses related to supplies and equipment, facilities, corporate and liability insurance, information technology, travel, business development, and office and professional expenses; partially offset by increased depreciation expense. |
Total Other Income (Expense), Net
Total other income (expense), net, for the years ended December 31, 2023 and 2022 was as follows:
| Year Ended December 31, |
||||||||||||
| (in thousands) |
2023 |
2022 |
Change |
|||||||||
| Interest income |
$ | 1,389 | $ | 225 | 517 | % | ||||||
| Interest expense |
(4,558 | ) | (3,296 | ) | 38 | % | ||||||
| Gain on termination of lease |
— | 420 | * | |||||||||
| Commitment share expense |
(402 | ) | — | * | ||||||||
| Issuance costs for common stock warrant liabilities |
(333 | ) | — | * | ||||||||
| Loss on initial issuance of equity |
(14,840 | ) | — | * | ||||||||
| Change in fair value of common stock warrant liabilities |
6,337 | 169 | 3,650 | % | ||||||||
| Change in fair value of Clene Nanomedicine contingent earn-out liability |
2,189 | 15,836 | (86 | )% | ||||||||
| Change in fair value of Initial Stockholders contingent earn-out liability |
281 | 2,026 | (86 | )% | ||||||||
| Research and development tax credits and unrestricted grants |
963 | 3,079 | (69 | )% | ||||||||
| Other income, net |
10 | 32 | (69 | )% | ||||||||
| Total other income (expense), net |
$ | (8,964 | ) | $ | 18,491 | * | ||||||
| * | Not meaningful. |
The change in total other income (expense), net, was primarily due to the following:
| (i) | an increase in interest income primarily due to increased balances of cash and cash equivalents and increasing interest rates on cash and cash equivalents; and an increase in interest expense primarily due to increasing interest rates and increased amortization of debt discount and debt issuance costs on notes payable; |
| (ii) | a gain on termination of lease due to the termination of an operating lease for office space during the year ended December 31, 2022; |
| (iii) | commitment share expense, due to the shares of Common Stock issued to Lincoln Park Capital Fund, LLC (“Lincoln Park”), as an initial fee for Lincoln Park’s commitment to purchase shares of Common Stock under a purchase agreement with the Company during the year ended December 31, 2023; |
| (iv) | issuance costs from a public equity offering allocated to liability-classified warrants during the year ended December 31, 2023; |
| (v) | a loss on initial issuance of equity from the fair value in excess of proceeds from a public equity offering during the year ended December 31, 2023; |
| (vi) | a gain from a change in fair value of the common stock warrant liability due to the Original Avenue Warrant during the year ended December 31, 2022 and the New Avenue Warrant and Tranche A Warrants during the year ended December 31, 2023. The changes in fair value were due to the change in price of our Common Stock on Nasdaq and updates in the valuation model assumptions (see “Critical Accounting Estimates”). As of March 31, 2022, we reclassified Tranche 1 of the Original Avenue Warrant to additional paid-in capital. As of December 31, 2022, Tranche 2 of the Original Avenue Warrant expired, we recognized income of $0.2 million, and the warrant liability was extinguished; |
| (vii) | a gain from a change in fair value of the Clene Nanomedicine Contingent Earn-out liability and Initial Stockholders Contingent Earn-out liability during the years ended December 31, 2023 and 2022. The changes were due to the price of our Common Stock on Nasdaq and updates in the valuation model assumptions at the end of each respective period (see “Critical Accounting Estimates”); |
| (viii) | a decrease in research and development tax credits and unrestricted grants due to changes in the amount of qualifying research and development expenses incurred and changes in the reimbursement percentage; and |
| (vii) | other income during the years ended December 31, 2023 and 2022, primarily due to realized gains and losses on foreign currency transactions and other miscellaneous income and expense items. |
Taxation
United States
We are incorporated in the state of Delaware and subject to statutory U.S. federal corporate income tax at a rate of 21.00% for the years ended December 31, 2023 and 2022. We are also subject to state income tax in Utah at a rate of 4.65% and 4.85% for the years ended December 31, 2023 and 2022, respectively; and in Maryland at a rate of 8.25% for the years ended December 31, 2023 and 2022. As of December 31, 2023 and 2022, we recorded a full valuation allowance against our net deferred tax assets due to the uncertainty as to whether such assets will be realized resulting from our three-year cumulative loss position and the uncertainty surrounding our ability to generate pre-tax income in the foreseeable future.
Australia
Our wholly-owned subsidiary, Clene Australia Pty Ltd (“Clene Australia”), was established in Australia in March 2018 and is subject to corporate income tax at a rate of 30.00% for the years ended December 31, 2023 and 2022. Clene Australia had no taxable income or provision for income taxes for the years ended December 31, 2023 and 2022. We recorded other income of $1.0 million and $3.1 million for the years ended December 31, 2023 and 2022, respectively, for research and development tax credits pertaining to Clene Australia for the 2023 and 2022 tax years, respectively.
Netherlands
Our wholly-owned subsidiary, Clene Netherlands B.V. (“Clene Netherlands”), was established in the Netherlands in April 2021 and is subject to corporate income tax at a rate of 19.00% up to €200,000 of taxable income and 25.80% for taxable income in excess of €200,000 for the year ended December 31, 2023; and 15.00% up to €395,000 of taxable income and 25.80% for taxable income in excess of €395,000 for the year ended December 31, 2022. Clene Netherlands had no taxable income or provision for income taxes for the years ended December 31, 2023 and 2022.
Liquidity and Capital Resources
Sources of Capital
We have incurred significant losses and negative cash flows from operations since our inception. We expect to incur additional losses in the future to fund our operations and conduct research and development of our drug candidates. We recognize the need to raise additional capital to fully implement our business plan. The long-term continuation of our business plan is dependent upon the generation of sufficient revenues from our products to offset expenses and capital expenditures. In the event that we do not generate sufficient revenues and are unable to obtain funding, we will be forced to delay, reduce, or eliminate some or all of our research and development programs, product portfolio expansion, commercialization efforts, or capital expenditures, which could adversely affect our business prospects, ability to meet long-term liquidity needs, or we may be unable to continue operations.
Since our inception, we have dedicated substantially all our resources to the development of our drug candidates. We have financed our operations principally through the following sources:
| ● |
gross proceeds of $175.1 million from equity financing, including sales of common stock, preferred stock, and warrants to purchase common stock; |
| ● |
gross proceeds of $32.3 million from borrowings under convertible promissory notes; |
| ● |
gross proceeds of $27.3 million from borrowings under notes payable and convertible notes payable; |
| ● |
gross proceeds of $9.4 million from the Reverse Recapitalization; |
| ● |
gross proceeds of $8.9 million from refundable research and development tax credits; |
| ● |
gross proceeds of $2.9 million from grants from various organizations; and |
| ● |
gross proceeds of $1.0 million from stock option and warrant exercises. |
We also received indirect financial support for the HEALEY ALS Platform Trial, administered by Massachusetts General Hospital, which conducted a platform trial for the treatment of ALS with certain drug candidates, including CNM-Au8, at significantly lower costs than we would have otherwise incurred if we had conducted a comparably designed clinical trial at reasonable market rates.
Going Concern
We incurred a loss from operations of $40.5 million and $48.4 million for the years ended December 31, 2023 and 2022, respectively. Our accumulated deficit was $242.7 million and $193.2 million as of December 31, 2023 and 2022. Our cash, cash equivalents, and marketable securities totaled $35.0 million and $23.3 million as of December 31, 2023 and 2022, respectively, and net cash used in operating activities was $30.2 million and $39.0 million for the years ended December 31, 2023 and 2022, respectively.
We have incurred significant losses and negative cash flows from operations since our inception. We have not generated significant revenues since our inception, and we do not anticipate generating significant revenues unless we successfully complete development and obtain regulatory approval for commercialization of a drug candidate. We expect to incur additional losses in the future, particularly as we advance the development of our clinical-stage drug candidates, continue research and development of our preclinical drug candidates, and initiate additional clinical trials of, and seek regulatory approval for, these and other future drug candidates. We expect that within the next twelve months, we will not have sufficient cash and other resources on hand to sustain our current operations or meet our obligations as they become due unless we obtain additional financing. Additionally, pursuant to our term loan with Avenue Venture Opportunities Fund, L.P. (“Avenue”), we are required to maintain unrestricted cash and cash equivalents of at least $5.0 million to avoid acceleration of the full balance of the loan (see Note 8 to the consolidated financial statements). These conditions raise substantial doubt about the Company’s ability to continue as a going concern.
To mitigate our funding needs, we plan to raise additional funding, including exploring equity financing and offerings, debt financing, licensing or collaboration arrangements with third parties, as well as utilizing our existing at-the-market facility and equity purchase agreement and potential proceeds from the exercise of outstanding warrants and stock options. These plans are subject to market conditions and reliance on third parties, and there is no assurance that effective implementation of our plans will result in the necessary funding to continue current operations. We have implemented cost-saving initiatives, including delaying and reducing certain research and development programs and commercialization efforts and elimination of certain staff positions. We have concluded that our plans do not alleviate the substantial doubt about our ability to continue as a going concern beyond one year from the date the consolidated financial statements are issued.
The accompanying consolidated financial statements have been prepared assuming we will continue as a going concern, which contemplates the realization of assets and satisfaction of liabilities in the normal course of business. As a result, the accompanying consolidated financial statements do not include any adjustments relating to the recoverability and classification of assets and their carrying amounts, or the amounts and classification of liabilities that may result should we be unable to continue as a going concern.
Short-Term Material Cash Requirements
For at least the next twelve months, our primary capital requirements are to fund our operations, including research and development, personnel, regulatory, and other clinical trial costs related to development of our lead drug candidate, CNM-Au8; and general and administrative costs to support our drug development and pre-commercial activities in advance of receiving regulatory approval for our drug candidates. Firm commitments for funds include approximately $27,000 and $1.1 million of payments under finance and operating lease obligations, respectively; payment of principal and interest on notes payable totaling $22.5 million; and commitments under various agreements for capital expenditures totaling $0.4 million related to the construction of our manufacturing facilities. We expect to meet our short-term liquidity requirements primarily through cash on hand. Additional sources of funds include equity financing, debt financing, or other capital sources.
We enter into agreements in the normal course of business with CROs for clinical trials and with vendors for preclinical studies and other services and products for operating purposes, which are cancelable at any time by us, subject to payment of our remaining obligations under binding purchase orders and, in certain cases, nominal early termination fees. These commitments are not deemed significant.
Long-Term Material Cash Requirements
Beyond the next twelve months, our primary capital requirements are to fund our operations, including research and development, personnel, regulatory, and other clinical trial costs related to development of our lead drug candidate, CNM-Au8; and general and administrative costs to support our drug development activities in advance of receiving regulatory approval for our drug candidates. Additional funds may be spent to initiate new clinical trials, at our discretion. Known obligations beyond the next twelve months include $6.4 million of payments under operating lease obligations, and interest and principal repayment of notes payable of $9.1 million. We expect to meet our long-term liquidity requirements primarily through equity financing, debt financing, or other capital sources.
Use of Funds
Our cash flows for the years ended December 31, 2023 and 2022 were as follows:
| Year Ended December 31, |
||||||||
| (in thousands) |
2023 |
2022 |
||||||
| Net cash used in operating activities |
$ | (30,171 | ) | $ | (39,011 | ) | ||
| Net cash used in investing activities |
(1,499 | ) | (10,164 | ) | ||||
| Net cash provided by financing activities |
42,163 | 17,249 | ||||||
| Effect of foreign exchange rate changes on cash |
(4 | ) | (30 | ) | ||||
| Net increase (decrease) in cash, cash equivalents and restricted cash |
$ | 10,489 | $ | (31,956 | ) | |||
Our primary use of cash in all periods presented was to fund our research and development, regulatory and other clinical trial costs, and general corporate expenditures.
Operating Activities
Net cash used in operating activities was $30.2 million for the year ended December 31, 2023, which resulted from a net loss of $49.5 million, adjusted for non-cash items totaling $19.5 million and a net change in operating assets and liabilities of $0.2 million. Significant non-cash items included (i) depreciation expense of $1.7 million relating to laboratory and office equipment and leasehold improvements; (ii) non-cash lease expense of $0.4 million; (iii) commitment share expense of $0.4 million related to the shares of Common Stock issued to Lincoln Park as an initial fee for Lincoln Park’s commitment to purchase Common Stock under a purchase agreement with the Company; (iv) issuance costs of $0.3 million from a public equity offering allocated to liability-classified warrants; (v) a loss on initial issuance of equity of $14.8 million from the fair value in excess of proceeds from a public equity offering; (vi) stock-based compensation expense of $9.1 million; (vii) accretion of debt discount of $1.2 million; (viii) non-cash interest expense of $0.4 million; and (ix) changes in fair value of the Clene Nanomedicine and Initial Stockholders Contingent Earn-outs of $2.2 million and $0.3 million, respectively, primarily driven by the decrease in price of our Common Stock on Nasdaq; and (x) a change in fair value of our common stock warrant liabilities of $6.3 million, primarily driven by the decrease in price of our Common Stock on Nasdaq and changes in valuation model inputs. The net change in operating assets and liabilities was primarily attributable to the following: (a) a decrease in accounts receivable of $46,000 and a decrease in accounts payable of $1.5 million due to the timing of vendor invoicing and payments; (b) a decrease in prepaid expenses and other current assets of $2.0 million due to the timing of vendor invoicing and payments, the timing of receipt of metals to be used in research and development, and a decrease in research and development tax credits receivable; (c) a decrease in accrued liabilities of $0.1 million primarily due to a decrease in accrued CRO and clinical fees, partially offset by an increase in accrued compensation and benefits and other accrued liabilities; and (d) a decrease in operating lease obligations of $0.6 million.
Net cash used in operating activities was $39.0 million for the year ended December 31, 2022, which resulted from a net loss of $29.9 million, adjusted for non-cash items totaling $7.6 million and a net change in operating assets and liabilities of $1.5 million. Significant non-cash items included (i) depreciation expense of $1.0 million relating to laboratory and office equipment and leasehold improvements; (ii) non-cash lease expense of $0.4 million; (iii) stock-based compensation expense of $8.5 million; (iv) gain on termination of lease of $0.4 million; (v) accretion of debt discount of $0.9 million; (vi) non-cash interest expense of $0.1 million; and (vii) the changes in fair value of the Clene Nanomedicine and Initial Stockholders Contingent Earn-outs of $15.8 million and $2.0 million, respectively, and the change in fair value of common stock warrant liability of $0.2 million. The changes in fair value of these instruments were primarily driven by the decrease of the closing price of our Common Stock on Nasdaq. The net change in operating assets and liabilities was primarily attributable to the following: (a) an increase in accounts receivable of $0.1 million and an increase in accounts payable of $0.3 million due to the timing of vendor invoicing and payments; (b) an increase in prepaid expenses and other current assets of $1.4 million due to the timing of vendor invoicing and payments, the timing of receipt of metals to be used in research and development, and an increase in research and development tax credits receivable; (c) an increase in accrued liabilities of $0.3 million primarily due to decreased accrued compensation and benefits; and (d) a decrease in operating lease obligations of $0.5 million.
Investing Activities
Net cash used in investing activities was $1.5 million for the year ended December 31, 2023, which consisted of (i) purchases of marketable securities of $6.2 million and (ii) purchases of property and equipment of $0.3 million, offset primarily by (iii) proceeds from maturities of marketable securities of $5.0 million. Net cash used in investing activities was $10.2 million for year ended December 31, 2022, which consisted of (i) purchases of marketable securities of $24.6 million and (ii) purchases of property and equipment of $5.2 million, partially offset by (iii) proceeds from maturities of marketable securities of $12.0 million and (iv) proceeds from sale of marketable securities of $7.6 million.
Financing Activities
Net cash provided by financing activities was $42.2 million for the year ended December 31, 2023, which consisted of (i) proceeds from issuance of common stock and warrants, net of offering costs, of $42.1 million, and (ii) proceeds from the issuance of notes payable of $0.4 million; partially offset by (iii) payments of finance lease obligations of $0.1 million and (iv) payments of notes payable modification fees of $0.2 million. Net cash provided by financing activities was $17.3 million for the year ended December 31, 2022, which consisted of (i) proceeds from exercise of stock options of $0.3 million, (ii) proceeds from issuance of common stock, net of offering costs, of $11.5 million, and (iii) proceeds from the issuance of notes payable of $5.7 million; partially offset by (iv) payments of finance lease obligations of $0.1 million and (v) payments of notes payable issuance costs of $0.1 million.
Public Offering
In June 2023, we sold 50,000,000 units at a sale price of $0.80 per unit pursuant to an underwriting agreement with Canaccord Genuity LLC (“Canaccord”) as underwriter. Each unit consisted of (i) one share of Common Stock, (ii) one warrant to purchase one share of Common Stock at an exercise price of $1.10 per share (the “Tranche A Warrants”), and (iii) one warrant to purchase one share of Common Stock at an exercise price of $1.50 per share (the “Tranche B Warrants”). The aggregate gross proceeds were $40.0 million, excluding the proceeds, if any, from the exercise of the Tranche A Warrants and Tranche B Warrants. We cannot predict when or if the Tranche A Warrants or Tranche B Warrants will be exercised, and it is possible they may expire and/or never be exercised. We paid underwriting discounts and commissions of $2.4 million and offering expenses of $0.2 million. The offering was made pursuant to our registration statement on Form S-3 (file number 333-264299), which was declared effective by the SEC on April 26, 2022, a related registration statement pursuant to Rule 462(b) (file number 333-272692), filed with the SEC and effective on June 16, 2023, and our prospectus supplement relating to the offering.
Common Stock Sales Agreement
During the year ended December 31, 2023, we sold 2,895,090 shares of Common Stock under our Equity Distribution Agreement (the “ATM Agreement”) with Canaccord, generated gross proceeds of $4.5 million, and paid commissions of $0.1 million. During the year ended December 31, 2022, we sold 358,769 shares of Common Stock and generated gross proceeds of $0.8 million, and commissions paid to Canaccord were insignificant. The issuance and sale of Common Stock by us under the ATM Agreement was made pursuant to our registration statement on Form S-3 (file number 333-264299), which was declared effective by the Securities and Exchange Commission on April 26, 2022, and our prospectus supplement relating to the offering. On June 16, 2023, we suspended and terminated the prospectus supplement related to the offering, and on November 7, 2023, we filed a prospectus supplement for future sales pursuant to the ATM Agreement having an aggregate offering price of up to $15.0 million.
Common Stock Purchase Agreement
During the year ended December 31, 2023, we sold 400,000 shares of Common Stock under the purchase agreement (the “Purchase Agreement”) with Lincoln Park, issued 2,893 Additional Commitment Shares, and generated proceeds of $0.4 million. The issuance and sale of Common Stock under the Purchase Agreement is made pursuant to our registration statement on Form S-3 (file number 333-264299), which was declared effective by the SEC on April 26, 2022. On June 16, 2023, we suspended and terminated the prospectus supplement (the “Purchase Agreement Prospectus Supplement”) related to the offering with respect to the unsold shares of Common Stock issuable pursuant to the Purchase Agreement. We will not make any further sales of our securities pursuant to the Purchase Agreement, unless and until a new prospectus supplement is filed. Other than the termination of the Purchase Agreement Prospectus Supplement and offering with respect to future sales by us, the Purchase Agreement remains in full force and effect.
Critical Accounting Estimates
Our discussion and analysis of our financial condition and results of operations is based on our consolidated financial statements, which have been prepared in accordance with U.S. Generally Accepted Accounting Principles. The preparation of these consolidated financial statements requires us to make estimates, assumptions, and judgments that affect the reported amounts of assets, liabilities, revenues, costs, and expenses. We evaluate our estimates and judgments on an ongoing basis, and our actual results may differ from these estimates. We base our estimates on historical experience, known trends and events, contractual milestones, and other various factors that are believed to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources.
We consider the following estimates to be critical as they involve a significant level of estimation uncertainty and have had or are reasonably likely to have a material impact on our financial condition and results of operations.
Contingent Earn-Out Liabilities
In connection with the Reverse Recapitalization, certain stockholders are entitled to the Contingent Earn-out payments based on achievement of certain milestones. In accordance with ASC 815, we classified the Contingent Earn-outs as liabilities and measured them at fair value on the date of the Reverse Recapitalization. We remeasure the liabilities at each reporting date and record the change in fair value as a component of other income (expense), net, in the consolidated statements of operations and comprehensive loss. The change in fair value of the Clene Nanomedicine Contingent Earn-out resulted in a gain of $2.2 million and $15.8 million for the years ended December 31, 2023 and 2022, respectively. The change in fair value of the Initial Stockholders Contingent Earn-out resulted in a gain of $0.3 million and $2.0 million for the years ended December 31, 2023 and 2022, respectively. We estimate the fair value using a Monte Carlo valuation model, which requires significant judgment. The unobservable inputs include the expected stock price volatility, the risk-free interest rate, and the expected term. As of December 31, 2023 and 2022, the unobservable inputs were as follows:
| December 31, |
December 31, |
|||||||
| 2023 |
2022 |
|||||||
| Expected stock price volatility |
115.00 | % | 115.00 | % | ||||
| Risk-free interest rate |
4.20 | % | 4.20 | % | ||||
| Expected dividend yield |
0.00 | % | 0.00 | % | ||||
| Expected term (in years) |
2.00 | 3.00 | ||||||
Convertible Notes
Pursuant to the 2021 Avenue Loan, $5.0 million of the outstanding principal is subject to a conversion option. In accordance with ASU 2020-06, Debt—Debt with Conversion and Other Options (Subtopic 470-20) and Derivatives and Hedging—Contracts in Entity’s Own Equity (Subtopic 815-40): Accounting for Convertible Instruments and Contracts in an Entity’s Own Equity, we classified this portion as convertible notes payable in the consolidated balance sheets and did not separate the conversion option from the host contract as it did not meet the requirements for accounting as a derivative instrument. We account for the convertible note as a single liability measured at its amortized cost. As of December 31, 2023 and 2022, the convertible note was carried at $4.9 million and $4.8 million, respectively.
We classified the 2022 DHCD Loan as convertible notes payable in the consolidated balance sheets and did not separate the conversion option from the host contract as it did not meet the requirements for accounting as a derivative instrument. We account for the convertible note as a single liability measured at its amortized cost. As of December 31, 2023 and 2022, the convertible note was carried at $5.3 million and $5.0 million, respectively.
Common Stock Warrant Liabilities
Pursuant to a June 2023 amendment to the 2021 Avenue Loan, we issued a warrant to purchase 3,000,000 shares of Common Stock at $0.80 per share (the “New Avenue Warrant”). In accordance with ASC 815, we recognized the New Avenue Warrant as a derivative liability measured at fair value and remeasure the New Avenue Warrant at each reporting date and record the change in fair value as a component of other income (expense), net, in the consolidated statements of operations and comprehensive loss. The change in fair value of the New Avenue Warrant resulted in a gain of $0.5 million for the year ended December 31, 2023. We estimate the fair value using a Black-Scholes option-pricing model with probability weights for the occurrence of the following events: (i) settlement of the instrument upon a change of control transaction, (ii) dissolution of the Company, or (iii) another outcome outside of (i)-(ii). These estimates require significant judgment. As of December 31, 2023, the unobservable inputs were as follows:
| December 31, |
||||
| 2023 |
||||
| Expected stock price volatility |
105.00% –110.00 | % | ||
| Risk-free interest rate |
3.88% –5.03 | % | ||
| Expected dividend yield |
0.00 | % | ||
| Expected term (in years) |
0.75 –4.5 | |||
| Probability of change of control |
25.00 | % | ||
| Probability of dissolution |
50.00 | % | ||
| Probability of other outcome |
25.00 | % | ||
Pursuant to an underwritten public offering in June 2023, we issued the Tranche A Warrants to purchase 50,000,000 shares of Common Stock at $1.10 per share and the Tranche B Warrants to purchase 50,000,000 shares of Common Stock at $1.50 per share. In accordance with ASC 815, we recognized the Tranche A Warrants as derivative liabilities measured at fair value and will remeasure the Tranche A Warrants at each reporting date and record the change in fair value as a component of other income (expense), net, in the consolidated statements of operations and comprehensive loss (the Tranche B Warrants qualified for equity classification at issuance). The change in fair value of the Tranche A Warrants out resulted in a gain of $5.8 million for the year ended December 31, 2023. We estimate the fair value using a Black-Scholes option-pricing model with probability weights for the occurrence of the following events: (i) FDA acceptance of an NDA for CNM-Au8, (ii) settlement upon a fundamental transaction, (iii) dissolution of the Company, and (iv) another outcome outside of (i)-(iii). These estimates require significant judgment. As of December 31, 2023, the unobservable inputs were as follows:
| December 31, |
||||
| 2023 |
||||
| Expected stock price volatility |
100.00% –110.00 | % | ||
| Risk-free interest rate |
4.13% –4.74 | % | ||
| Expected dividend yield |
0.00 | % | ||
| Expected term (in years) |
1.08 –2.46 | |||
| Probability of NDA acceptance |
20.00 | % | ||
| Probability of fundamental transaction |
25.00 | % | ||
| Probability of dissolution |
50.00 | % | ||
| Probability of other outcome |
5.00 | % | ||
Income Taxes
We account for uncertainty in income taxes by applying a two-step process to determine the amount of tax benefit to be recognized in the consolidated financial statements. First, the tax position is evaluated to determine the likelihood that it will be sustained upon external examination by the taxing authorities. If the tax position is deemed more-likely-than-not to be sustained, the tax position is then assessed to determine the amount of benefit to recognize. The amount of the benefit that may be recognized is the largest amount that has a greater than 50% likelihood of being realized upon ultimate settlement. Additionally, we assess the likelihood that our deferred tax assets will be recovered from future taxable income and, to the extent we believe, based upon the weight of available evidence, that it is more likely than not that all or a portion of the deferred tax assets will not be realized, a valuation allowance is established through a charge to income tax expense. Potential for recovery of deferred tax assets is evaluated by estimating the future taxable profits expected and considering prudent and feasible tax planning strategies. The estimation of these factors requires significant judgment. Based on our evaluation of these factors, we have not recorded income tax benefits for the net operating losses or for research and development tax credits or other deferred tax assets due to uncertainty of realizing benefits from these items.
Stock-Based Compensation
We account for stock-based compensation arrangements using a fair value-based method for costs related to all share-based payments including stock options and stock awards. The fair value is recognized over the period during which a grantee was required to provide services in exchange for the option award and service-based stock awards, known as the requisite service period (usually the vesting period), on a straight-line basis. For stock awards with market conditions, the fair value is recognized over the period based on the expected milestone achievement dates as the derived service period (usually the vesting period), on a straight-line basis. For stock awards with performance conditions, the grant-date fair value of these awards is the market price on the applicable grant date, and compensation expense will be recognized when the conditions become probable of being satisfied. We will recognize a cumulative true-up adjustment once the conditions become probable of being satisfied as the related service period had been completed in a prior period. We elect to account for forfeitures as they occur, rather than estimating expected forfeitures.
We estimate the fair value of stock options using a Black-Scholes option-pricing model, which requires significant judgment. The unobservable inputs include the expected price volatility, risk-free interest rate, expected dividend yield, and expected term. For the years ended December 31, 2023 and 2022, the unobservable inputs were as follows:
| Year Ended December 31, |
||||||||
| 2023 |
2022 |
|||||||
| Expected stock price volatility |
96.22% –103.31 | % | 89.57% –99.77 | % | ||||
| Risk-free interest rate |
3.26% –4.66 | % | 1.65% –4.31 | % | ||||
| Expected dividend yield |
0.00 | % | 0.00 | % | ||||
| Expected term of options (in years) |
5.00 –6.43 | 5.00 –6.98 | ||||||
We estimate the fair value of restricted stock awards using a Monte Carlo valuation model to simulate the achievement of certain stock price milestones. The unobservable inputs include the expected stock price volatility, risk-free interest rate, and expected term. No restricted stock awards were granted during the years ended December 31, 2023 and 2022.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
As a smaller reporting company, we are not required to provide information required by this Item.
Item 8. Financial Statements and Supplementary Data
Index to Consolidated Financial Statements
| Report of Independent Registered Public Accounting Firm (PCAOB ID: | F-1 |
| F-2 | |
| Consolidated Statements of Operations and Comprehensive Loss | F-3 |
| F-4 | |
| F-5 | |
| F-6 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the stockholders and the Board of Directors of Clene Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Clene Inc. and subsidiaries (the “Company”) as of December 31, 2023 and 2022, the related consolidated statements of operations and comprehensive loss, stockholders’ equity, and cash flows, for each of the two years in the period ended December 31, 2023, and the related notes (collectively referred to as the “financial statements”). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2023 and 2022, and the results of its operations and its cash flows for each of the two years in the period ended December 31, 2023, in conformity with accounting principles generally accepted in the United States of America.
Going Concern
The accompanying financial statements have been prepared assuming that the Company will continue as a going concern. As discussed in Note 1 to the financial statements, the Company has incurred significant losses and negative cash flows from operations since inception and will not have sufficient cash and other resources on hand to sustain current operations or meet obligations as they become due, that raise substantial doubt about the Company’s ability to continue as a going concern. Management’s plans in regard to these matters are also described in Note 1. The financial statements do not include any adjustments that might result from the outcome of this uncertainty.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (“PCAOB”) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/
March 13, 2024
We have served as the Company’s auditor since 2021.
CONSOLIDATED BALANCE SHEETS
(In thousands, except share and per share amounts)
| December 31, | December 31, | |||||||
| 2023 | 2022 | |||||||
| ASSETS | ||||||||
| Current assets: | ||||||||
| Cash and cash equivalents | $ | $ | ||||||
| Marketable securities | ||||||||
| Accounts receivable | ||||||||
| Inventory | ||||||||
| Prepaid expenses and other current assets | ||||||||
| Total current assets | ||||||||
| Restricted cash | ||||||||
| Operating lease right-of-use assets | ||||||||
| Property and equipment, net | ||||||||
| TOTAL ASSETS | $ | $ | ||||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY | ||||||||
| Current liabilities: | ||||||||
| Accounts payable | $ | $ | ||||||
| Accrued liabilities | ||||||||
| Operating lease obligations, current portion | ||||||||
| Finance lease obligations, current portion | ||||||||
| Notes payable, current portion | ||||||||
| Convertible notes payable, current portion | ||||||||
| Total current liabilities | ||||||||
| Operating lease obligations, net of current portion | ||||||||
| Finance lease obligations, net of current portion | ||||||||
| Notes payable, net of current portion | ||||||||
| Convertible notes payable, net of current portion | ||||||||
| Common stock warrant liabilities | ||||||||
| Clene Nanomedicine contingent earn-out liability | ||||||||
| Initial Stockholders contingent earn-out liability | ||||||||
| TOTAL LIABILITIES | ||||||||
| Commitments and contingencies (Note 9) | ||||||||
| Stockholders’ equity: | ||||||||
| Common stock, $ par value: and shares authorized at December 31, 2023 and December 31, 2022, respectively; and shares issued and outstanding at December 31, 2023 and December 31, 2022, respectively | ||||||||
| Additional paid-in capital | ||||||||
| Accumulated deficit | ( | ) | ( | ) | ||||
| Accumulated other comprehensive income | ||||||||
| TOTAL STOCKHOLDERS’ EQUITY | ||||||||
| TOTAL LIABILITIES AND STOCKHOLDERS’ EQUITY | $ | $ | ||||||
See accompanying notes to the consolidated financial statements.
CONSOLIDATED STATEMENTS OF OPERATIONS AND COMPREHENSIVE LOSS
(In thousands, except share and per share amounts)
| Year Ended December 31, |
||||||||
| 2023 |
2022 |
|||||||
| Revenue: |
||||||||
| Product revenue |
$ | $ | ||||||
| Royalty revenue |
||||||||
| Total revenue |
||||||||
| Operating expenses: |
||||||||
| Cost of revenue |
||||||||
| Research and development |
||||||||
| General and administrative |
||||||||
| Total operating expenses |
||||||||
| Loss from operations |
( |
) | ( |
) | ||||
| Other income (expense), net: |
||||||||
| Interest income |
||||||||
| Interest expense |
( |
) | ( |
) | ||||
| Gain on termination of lease |
||||||||
| Commitment share expense |
( |
) | ||||||
| Issuance costs for common stock warrant liabilities |
( |
) | ||||||
| Loss on initial issuance of equity |
( |
) | ||||||
| Change in fair value of common stock warrant liabilities |
||||||||
| Change in fair value of Clene Nanomedicine contingent earn-out liability |
||||||||
| Change in fair value of Initial Stockholders contingent earn-out liability |
||||||||
| Research and development tax credits and unrestricted grants |
||||||||
| Other income, net |
||||||||
| Total other income (expense), net |
( |
) | ||||||
| Net loss before income taxes |
( |
) | ( |
) | ||||
| Income tax benefit |
— |
— |
||||||
| Net loss |
( |
) | ( |
) | ||||
| Other comprehensive loss: |
||||||||
| Unrealized gain (loss) on available-for-sale securities |
( |
) | ||||||
| Foreign currency translation adjustments |
( |
) | ( |
) | ||||
| Total other comprehensive loss |
( |
) | ( |
) | ||||
| Comprehensive loss |
$ | ( |
) | $ | ( |
) | ||
| Net loss per share – basic and diluted |
$ | ( |
) | $ | ( |
) | ||
| Weighted average common shares used to compute basic and diluted net loss per share |
||||||||
See accompanying notes to the consolidated financial statements.
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY
(In thousands, except share amounts)
| Common Stock |
Additional Paid-In | Accumulated |
Accumulated Other Comprehensive | Total Stockholders’ | ||||||||||||||||||||
| Shares |
Amount |
Capital |
Deficit |
Income (Loss) |
Equity |
|||||||||||||||||||
| Balances at December 31, 2021 |
$ | $ | $ | ( |
) | $ | $ | |||||||||||||||||
| Issuance of common stock |
||||||||||||||||||||||||
| Reclassification of common stock warrant liability to equity |
— | |||||||||||||||||||||||
| Exercise of stock options |
||||||||||||||||||||||||
| Stock-based compensation expense |
— | |||||||||||||||||||||||
| Issuance of common stock upon vesting of restricted stock awards |
||||||||||||||||||||||||
| Unrealized loss on available-for-sale securities |
— | ( |
) | ( |
) | |||||||||||||||||||
| Foreign currency translation adjustment |
— | ( |
) | ( |
) | |||||||||||||||||||
| Net loss |
— | ( |
) | ( |
) | |||||||||||||||||||
| Balances at December 31, 2022 |
$ | $ | $ | ( |
) | $ | $ | |||||||||||||||||
| Issuance of common stock |
||||||||||||||||||||||||
| Issuance of equity-classified warrants |
— | |||||||||||||||||||||||
| Stock-based compensation expense |
— | |||||||||||||||||||||||
| Issuance of common stock upon vesting of restricted stock awards |
||||||||||||||||||||||||
| Unrealized gain on available-for-sale securities |
— | |||||||||||||||||||||||
| Foreign currency translation adjustment |
— | ( |
) | ( |
) | |||||||||||||||||||
| Net loss |
— | ( |
) | ( |
) | |||||||||||||||||||
| Balances at December 31, 2023 |
$ | $ | $ | ( |
) | $ | $ | |||||||||||||||||
See accompanying notes to the consolidated financial statements.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
| Year Ended December 31, |
||||||||
| 2023 |
2022 |
|||||||
| Cash flows from operating activities: |
||||||||
| Net loss |
$ | ( |
) | $ | ( |
) | ||
| Adjustments to reconcile net loss to net cash used in operating activities: |
||||||||
| Depreciation |
||||||||
| Non-cash lease expense |
||||||||
| Commitment share expense |
||||||||
| Issuance costs for common stock warrant liabilities |
||||||||
| Loss on initial issuance of equity |
||||||||
| Change in fair value of common stock warrant liabilities |
( |
) | ( |
) | ||||
| Change in fair value of Clene Nanomedicine contingent earn-out liability |
( |
) | ( |
) | ||||
| Change in fair value of Initial Stockholders contingent earn-out liability |
( |
) | ( |
) | ||||
| Stock-based compensation expense |
||||||||
| Gain on termination of lease |
( |
) | ||||||
| Loss on sale of marketable securities |
||||||||
| Accretion of debt discount |
||||||||
| Non-cash interest expense |
||||||||
| Changes in operating assets and liabilities: |
||||||||
| Accounts receivable |
( |
) | ||||||
| Inventory |
( |
) | ||||||
| Prepaid expenses and other current assets |
( |
) | ||||||
| Accounts payable |
( |
) | ||||||
| Accrued liabilities |
( |
) | ||||||
| Operating lease obligations |
( |
) | ( |
) | ||||
| Net cash used in operating activities |
( |
) | ( |
) | ||||
| Cash flows from investing activities: |
||||||||
| Purchases of marketable securities |
( |
) | ( |
) | ||||
| Proceeds from maturities of marketable securities |
||||||||
| Proceeds from sales of marketable securities |
||||||||
| Purchases of property and equipment |
( |
) | ( |
) | ||||
| Net cash used in investing activities |
( |
) | ( |
) | ||||
| Cash flows from financing activities: |
||||||||
| Proceeds from exercise of stock options |
||||||||
| Proceeds from issuance of common stock and warrants, net of offering costs |
||||||||
| Payments of finance lease obligations |
( |
) | ( |
) | ||||
| Proceeds from the issuance of notes payable |
||||||||
| Payments of notes payable issuance costs |
( |
) | ||||||
| Payments of notes payable modification fees |
( |
) | ||||||
| Net cash provided by financing activities |
||||||||
| Effect of foreign exchange rate changes on cash and restricted cash |
( |
) | ( |
) | ||||
| Net increase (decrease) in cash, cash equivalents and restricted cash |
( |
) | ||||||
| Cash, cash equivalents and restricted cash – beginning of period |
||||||||
| Cash, cash equivalents and restricted cash – end of period |
$ | $ | ||||||
| Reconciliation of cash, cash equivalents and restricted cash to the consolidated balance sheets |
||||||||
| Cash and cash equivalents |
$ | $ | ||||||
| Restricted cash |
||||||||
| Cash, cash equivalents and restricted cash |
$ | $ | ||||||
| Supplemental disclosure of non-cash investing and financing activities: |
||||||||
| Common stock warrant liability recorded upon debt modification |
$ | $ | ||||||
| Common stock warrant liability recorded upon public stock offering |
$ | $ | ||||||
| Lease liability arising from obtaining right-of-use assets, leasehold improvements, and lease incentives |
$ | $ | ||||||
| Lease incentive realized |
$ | $ | ||||||
| Lease liability settled through termination of lease |
$ | $ | ||||||
| Reclassification of common stock warrant liability to permanent equity |
$ | $ | ||||||
| Purchases of property and equipment in accounts payable |
$ | $ | ||||||
| Supplemental cash flow information: |
||||||||
| Cash paid for interest expense |
$ | $ | ||||||
See accompanying notes to the consolidated financial statements.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Note 1. Nature of the Business
Clene Inc. (the “Company,” “we,” “us,” or similar such references) is a clinical-stage pharmaceutical company pioneering the discovery, development, and commercialization of novel clean-surfaced nanotechnology therapeutics. We have developed an electro-crystal-chemistry drug development platform which enables production of concentrated, stable, highly active, clean-surfaced nanocrystal suspensions. We have multiple drug assets currently in development for applications primarily in neurology. Our efforts are currently focused on addressing the high unmet medical needs in central nervous system disorders including amyotrophic lateral sclerosis (“ALS”), multiple sclerosis (“MS”), and Parkinson’s disease (“PD”). Our patented electro-crystal-chemistry manufacturing platform further enables us to develop very low concentration dietary supplements to advance the health and well-being of broad populations. These dietary supplements can vary greatly and include nanocrystals of varying composition, shapes and sizes as well as ionic solutions with diverse metallic constituents. Dietary supplements are marketed and distributed through our wholly owned subsidiary, dOrbital, Inc., or through an exclusive license with 4Life Research LLC (“4Life”), an international supplier of health supplements, stockholder, and related party (see Note 15).
Clene Nanomedicine, Inc. (“Clene Nanomedicine”) became a public company on December 30, 2020 (the “Closing Date”) when it completed a reverse recapitalization (the “Reverse Recapitalization”) with Tottenham Acquisition I Limited (“Tottenham”), Tottenham’s wholly-owned subsidiary and our predecessor, Chelsea Worldwide Inc., and Creative Worldwide Inc., a wholly-owned subsidiary of Chelsea Worldwide Inc. On the Closing Date, Chelsea Worldwide Inc. changed its name to Clene Inc. and listed its shares of common stock, par value $
Going Concern
We incurred a loss from operations of $
We have incurred significant losses and negative cash flows from operations since our inception. We have not generated significant revenues since our inception, and we do not anticipate generating significant revenues unless we successfully complete development and obtain regulatory approval for commercialization of a drug candidate. We expect to incur additional losses in the future, particularly as we advance the development of our clinical-stage drug candidates, continue research and development of our preclinical drug candidates, and initiate additional clinical trials of, and seek regulatory approval for, these and other future drug candidates. We expect that within the next twelve months, we will not have sufficient cash and other resources on hand to sustain our current operations or meet our obligations as they become due unless we obtain additional financing. Additionally, pursuant to our term loan with Avenue Venture Opportunities Fund, L.P. (“Avenue”), we are required to maintain unrestricted cash and cash equivalents of at least $
To mitigate our funding needs, we plan to raise additional funding, including exploring equity financing and offerings, debt financing, licensing or collaboration arrangements with third parties, as well as utilizing our existing at-the-market facility, equity purchase agreement, and potential proceeds from the exercise of outstanding warrants and stock options. These plans are subject to market conditions and reliance on third parties, and there is no assurance that effective implementation of our plans will result in the necessary funding to continue current operations. We have implemented cost-saving initiatives, including delaying and reducing certain research and development programs and commercialization efforts and elimination of certain staff positions. We have concluded that our plans do not alleviate the substantial doubt about our ability to continue as a going concern beyond one year from the date the consolidated financial statements are issued.
The accompanying consolidated financial statements have been prepared assuming we will continue as a going concern, which contemplates the realization of assets and satisfaction of liabilities in the normal course of business. As a result, the accompanying consolidated financial statements do not include any adjustments relating to the recoverability and classification of assets and their carrying amounts, or the amounts and classification of liabilities that may result should we be unable to continue as a going concern.
Note 2. Summary of Significant Accounting Policies
Basis of Presentation
The accompanying consolidated financial statements include the accounts of Clene Inc. and our wholly-owned subsidiaries, Clene Nanomedicine, Inc., a subsidiary incorporated in Delaware, Clene Australia Pty Ltd (“Clene Australia”), a subsidiary incorporated in Australia, Clene Netherlands B.V. (“Clene Netherlands”), a subsidiary incorporated in the Netherlands, and dOrbital, Inc., a subsidiary incorporated in Delaware, after elimination of all intercompany accounts and transactions. We have prepared the accompanying consolidated financial statements in accordance with United States (“U.S.”) Generally Accepted Accounting Principles (“GAAP”) In the opinion of management, the consolidated financial statements reflect all adjustments, which are normal and recurring in nature, necessary for fair financial statement presentation.
Use of Estimates
The preparation of consolidated financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets, liabilities, and disclosure of contingent assets and liabilities, and the reported amounts of expenses. We base our estimates on historical experience and various other assumptions that we believe to be reasonable. Actual results may differ from those estimates or assumptions. Estimates are periodically reviewed in light of changes in circumstances, facts, and experience, and any changes in estimates will be recorded in future periods as they develop.
Risks and Uncertainties
We are subject to certain risks and uncertainties and believe that changes in any of the following areas could have a material adverse effect on future financial condition, results of operations, or cash flows: ability to obtain additional financing; regulatory approval and market acceptance of, and reimbursement for, product candidates; performance of third-party contract research organizations (“CROs”) and manufacturers upon which we rely; protection of our intellectual property; litigation or claims against us based on intellectual property, patent, product, regulatory, or other factors; and our ability to attract and retain employees necessary to support our growth. The product candidates we develop require approvals from regulatory agencies prior to commercial sales. There can be no assurance that our current and future product candidates will receive the necessary approvals or be commercially successful. If we are denied approval or approval is delayed, it will have a material adverse impact on our business and our consolidated financial statements.
Concentrations of Credit Risk
Financial instruments which potentially subject us to significant concentrations of credit risk consist primarily of cash. Our cash is held in financial institutions and amounts on deposit may at times exceed federally insured limits. We have not experienced any losses on our deposits of cash and do not believe that we are subject to unusual credit risk beyond the normal credit risk associated with commercial banking relationships.
Cash and Cash Equivalents
We consider all short-term investments with original maturities of 90 days or less when purchased to be cash equivalents.
Restricted Cash
We classify cash as restricted when it is unavailable for withdrawal or use in our general operating activities. Restricted cash is classified as current and noncurrent on the consolidated balance sheets based on the nature of the restriction. Our restricted cash balance includes contractually restricted deposits related to our corporate credit card.
Marketable Securities
Marketable securities are investments with original maturities of more than 90 days when purchased. We do not invest in securities with original maturities of more than one year. Marketable debt securities are considered available-for-sale and are recorded at fair value, with unrealized gains and losses included as a component of accumulated other comprehensive income until realized. Realized gains and losses are included in other income (expense), net, on the basis of specific identification. The cost of marketable securities is adjusted for amortization of premiums or accretion of discounts to maturity, and such amortization or accretion is included in other income (expense), net.
Accounts Receivable
Accounts receivable are stated at invoice value less estimated allowances for sales returns and doubtful accounts. We estimate the allowance for sales returns based on historical percentage of returns over a 12-month trailing average of sales. We continually monitor customer payments and maintain a reserve for expected losses resulting from our customers’ inability to make required payments. We consider factors when estimating the allowance for doubtful accounts such as historical experience, age of the accounts receivable balances, geographic related risks, and economic conditions that may affect a customer’s ability to pay. In cases where there are circumstances that may impair a specific customer’s ability to meet its financial obligations, a specific allowance is recorded against amounts due, thereby reducing the net recognized receivable to the amount reasonably believed to be collectible. Accounts receivable are written off when deemed uncollectible. Recoveries of accounts receivable previously written off are recorded when received. Historically, there have been no sales returns, no written-off accounts receivable, and no allowance for doubtful accounts reducing the balance of the accounts receivable.
Inventory
Inventory is stated at historic cost on a first-in first-out basis. Our inventory consisted of $
Property and Equipment
Property and equipment are stated at cost less accumulated depreciation. Property and equipment consist of laboratory and office equipment, computer software, and leasehold improvements. Depreciation is calculated using the straight-line method over the estimated economic useful lives of the assets, which are
We capitalize costs to obtain or develop computer software for internal use, including development costs incurred during the software development stage and costs to obtain software for access and conversion of historical data. We also capitalize costs to modify, upgrade, or enhance existing internal-use software that result in additional functionality. We expense costs incurred during the preliminary project stage, training costs, data conversion costs, and maintenance costs.
Impairment of Long-Lived Assets
Long-lived assets are tested for recoverability whenever events or changes in business circumstances indicate that the carrying amount of the assets may not be fully recoverable. Factors we consider in deciding when to perform an impairment review include significant underperformance of the business in relation to expectations, significant negative industry or economic trends, and significant changes or planned changes in the use of assets. If an impairment review is performed to evaluate an asset group for recoverability, we compare the forecasted undiscounted cash flows expected to result from the use and eventual disposition of the asset group to its carrying value. An impairment loss would be recognized when estimated undiscounted future cash flows expected to result from the use and eventual disposition of an asset group are less than its carrying amount. The impairment loss would be based on the excess of the carrying value of the impaired asset group over its fair value, determined based on discounted cash flows using market participant assumptions. We did record any impairment losses on long-lived assets during the years ended December 31, 2023 and 2022.
Debt
When debt is issued and a derivative is required to be separated (e.g., bifurcated conversion option) or another separate freestanding financial instrument (e.g., warrant) is issued, costs and fees incurred are allocated to the instruments issued (or bifurcated) in proportion to the allocation of proceeds. When some portions of the costs and fees relate to a bifurcated derivative or freestanding financial instrument that is being subsequently measured at fair value, those allocated costs are expensed immediately. Debt discounts, debt premiums, and debt issuance costs related to debt are recorded as deductions that net against the principal value of the debt and are amortized to interest expense over the contractual term of the debt using the effective interest method.
In accordance with ASC 470-20, Debt with Conversion and Other Options, when we issue debt with warrants, we treat the warrants as a debt discount, recorded as a contra-liability against the debt, and amortize the balance over the life of the underlying debt as interest expense in the consolidated statements of operations and comprehensive loss. The offset to the contra-liability is recorded as additional paid-in capital in the consolidated balance sheets if the warrants are not treated as a derivative or liability under ASC 480, Distinguishing Liabilities from Equity (“ASC 480”). Otherwise, the offset to the contra-liability is recorded as a warrant liability in the consolidated balance sheets and is subject to re-measurement to fair value at each balance sheet date, with any changes in fair value recognized in the consolidated statements of operations and comprehensive loss. If the debt is retired early, the associated debt discount is then recognized immediately as interest expense in the consolidated statements of operations and comprehensive loss.
Convertible Debt
In accordance with ASU 2020-06, Debt—Debt with Conversion and Other Options (Subtopic 470-20) and Derivatives and Hedging—Contracts in Entity’s Own Equity (Subtopic 815-40): Accounting for Convertible Instruments and Contracts in an Entity’s Own Equity, when we issue notes with conversion features, we evaluate if the conversion feature is freestanding or embedded. If the conversion feature is embedded, we do not separate the conversion feature from the host contract for convertible notes that are not required to be accounted for as derivatives, or that do not result in substantial premiums accounted for as paid-in-capital. Consequently, we account for a convertible note as a single liability measured at its amortized cost as long as no other features require separation and recognition as derivatives. If the conversion feature is freestanding, or is embedded and meets the requirements to be separated, we account for the conversion feature as a derivative under ASC 815, Derivatives and Hedging (“ASC 815”). We record the derivative instrument at fair value at inception, and subsequently re-measure to fair value at each reporting period and immediately prior to the extinguishment of the derivative instrument, with any changes recorded in the consolidated statements of operations and comprehensive loss.
Deferred Offering Costs
We capitalize certain third-party legal, accounting, and other fees that are directly associated with in-process equity financings until such financings are completed. After completion of the equity financing, these costs are recorded in stockholders’ equity as a reduction of proceeds generated as a result of the offering. Should any in-process equity financing be abandoned, the deferred offering costs will be expensed immediately as a charge to operating expenses in the consolidated statements of operations and comprehensive loss. As of December 31, 2023 and 2022, we did have any deferred offering costs.
Leases
At inception of a contract, we determine if a contract meets the definition of a lease. We determine if the contract conveys the right to control the use of an identified asset for a period of time. We assess throughout the period of use whether we have both of the following: (i) the right to obtain substantially all the economic benefits from use of the identified asset, and (ii) the right to direct the use of the identified asset. This determination is reassessed if the terms of the contract are changed. Leases are classified as operating or finance leases based on the terms of the lease agreement and certain characteristics of the identified asset. Right-of-use assets and lease liabilities are recognized at the lease commencement date based on the present value of the future lease payments less any lease incentives received. At the lease commencement date, the discount rate implicit in the lease is used to discount the lease liability if readily determinable. If not readily determinable or leases do not contain an implicit rate, our incremental borrowing rate is used as the discount rate. Our policy is to not record leases with an original term of twelve months or less within the consolidated balance sheets and we recognize lease expense for these short-term leases on a straight-line basis over the lease term.
Certain lease agreements may require us to pay additional amounts for taxes, insurance, maintenance, and other expenses, which are generally referred to as non-lease components. Such variable non-lease components are treated as variable lease payments and recognized in the period in which the obligation for these payments is incurred. Variable lease components and variable non-lease components are not measured as part of the right-of-use asset and liability. Only when lease components and their associated non-lease components are fixed are they accounted for as a single lease component and are recognized as part of a right-of-use asset and liability. Total contract consideration is allocated to the fixed lease and non-lease component. This policy election applies consistently to all asset classes under lease agreements.
Leases may contain clauses for renewal at our option. Payments to be made in option periods are recognized as part of the right-of-use lease assets and lease liabilities when it is reasonably certain that the option to extend the lease will be exercised, or is not at our option. We determine whether the reasonably certain threshold is met by considering contract-, asset-, market-, and entity-based factors. Operating lease expense, which is recognized on a straight-line basis over the lease term, and the amortization of finance lease right-of-use assets, which are included in property and equipment and depreciated, are included in research and development or general and administrative expenses consistent with the leased assets’ primary use. Accretion on the liabilities for finance leases is included in interest expense.
Contingent Earn-Out Liabilities
In connection with the Reverse Recapitalization, certain Clene Nanomedicine stockholders are entitled to receive additional shares of Common Stock (the “Clene Nanomedicine Contingent Earn-out”) as follows: (i)
In accordance with ASC 815, the Contingent Earn-outs are not indexed to our own stock and therefore were accounted for as a liability at the Reverse Recapitalization date and are subsequently remeasured to fair value at each reporting date with changes recorded as a component of other income (expense), net.
Common Stock Warrants
We account for common stock warrants as either equity-classified instruments or liability-classified instruments based on an assessment of the warrant terms. The assessment considers whether the warrants are freestanding financial instruments pursuant to ASC 480, meet the definition of a liability pursuant to ASC 480, and whether the warrants meet all the requirements for equity classification under ASC 815, including whether the warrants are indexed to our Common Stock, among other conditions for equity classification. This assessment, which requires the use of professional judgment, is conducted at the time of warrant issuance, and, for liability-classified warrants, at each reporting period end date while the warrants are outstanding.
Revenue Recognition
Under ASC 606, Revenue from Contracts with Customers (“ASC 606”), an entity recognizes revenue when its customer obtains control of promised goods or services, in an amount that reflects the consideration that the entity expects to receive in exchange for those goods or services. To determine revenue recognition for arrangements that an entity determines are within the scope of ASC 606, the entity performs the following five steps: (i) identify the contract(s) with a customer; (ii) identify the performance obligations in the contract; (iii) determine the transaction price, including variable consideration, if any; (iv) allocate the transaction price to the performance obligations in the contract; and (v) recognize revenue when (or as) the entity satisfies a performance obligation. We only apply the five-step model to contracts when it is probable that we will collect the consideration to which we are entitled in exchange for the goods or services we transfer to the customer.
Once a contract is determined to be within the scope of ASC 606 at contract inception, we review the contract to determine which performance obligations we must deliver, and which performance obligations are distinct. We recognize as revenue the amount of the transaction price that is allocated to each performance obligation when that performance obligation is satisfied or as it is satisfied. We typically satisfy our performance obligations via delivery of dietary supplements to the customer. Payments are due upon receipt for commercial transactions, or a prepayment is collected for online retail sales. Our revenue during the years ended December 31, 2023 and 2022 was comprised of sales of dietary supplements and royalties from sales of dietary supplements.
Grant Funding
We may submit applications to receive grant funding from governmental and non-governmental entities. We account for grants by analogizing to the grant accounting model under IAS 20, Accounting for Government Grants and Disclosure of Government Assistance (“IAS 20”). We recognize grant funding without conditions or continuing performance obligations, including certain research and development tax credits, as other income in the consolidated statements of operations and comprehensive loss. We accrue certain research and development tax credits receivable in other current assets (see Note 4) in an amount equal to the qualifying expenses incurred in each period multiplied by the applicable reimbursement percentage and we recognize other income in the consolidated statements of operations and comprehensive loss. After submission of our tax returns, we receive a cash refund of certain research and development tax credits and relieve the receivable.
We recognize grant funding with conditions or continuing performance obligations as a reduction in research and development expenses in the period during which the related qualifying expenses are incurred and as the conditions or performance obligations are fulfilled. Any amount received in advance of fulfilling such conditions or performance obligations is recorded in accrued liabilities (see Note 6) if the conditions or performance obligations are expected to be met within the next twelve months. We recognized grant funding of $
Fair Value of Financial Instruments
Certain assets and liabilities are carried at fair value under GAAP. Fair value is defined as the price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. Valuation techniques used to measure fair value must maximize the use of observable inputs and minimize the use of unobservable inputs. Financial assets and liabilities carried at fair value are to be classified and disclosed in one of the following three levels of the fair value hierarchy:
| ● | Level 1—Inputs based upon quoted market prices for identical assets or liabilities in active markets at the measurement date. |
| ● | Level 2—Observable inputs other than quoted market prices included in Level 1, such as quoted prices for similar assets and liabilities in active markets; quoted prices for identical or similar assets and liabilities in markets that are not active; or other inputs that are observable or can be corroborated by observable market data. |
| ● | Level 3—Inputs that are management’s best estimate of what market participants would use in pricing the asset or liability at the measurement date. The inputs are unobservable in the market and significant to the instrument’s valuation. |
We review the fair value hierarchy classification of our applicable assets and liabilities on a quarterly basis. Changes in the observability of valuation inputs may result in a reclassification for certain financial assets or liabilities. Reclassifications impacting all levels of the fair value hierarchy are reported as transfers in or out of the Level 1, 2, or 3 categories as of the beginning of the period during which the reclassifications occur.
Foreign Currency Translation and Transactions
Our functional currency is the U.S. dollar. Clene Australia determined its functional currency to be the Australian dollar and Clene Netherlands determined its functional currency to be the Euro. We use the U.S. dollar as our reporting currency for the consolidated financial statements. The results of our non-U.S. dollar based functional currency operations are translated to U.S. dollars at the average exchange rates during the period. Our assets and liabilities are translated using the current exchange rate as of the balance sheet date and stockholders’ equity is translated using historical rates. Adjustments resulting from the translation of the consolidated financial statements of our foreign functional currency subsidiaries into U.S. dollars are excluded from the determination of net loss and are accumulated in a separate component of stockholders’ equity. We also incur foreign exchange transaction gains and losses for purchases denominated in foreign currencies. Foreign exchange transaction gains and losses are included in other income (expense), net, as incurred.
Comprehensive Loss
Comprehensive loss includes net loss as well as other changes in stockholders’ equity that result from transactions and economic events other than those with stockholders. The only elements of other comprehensive loss in any periods presented were translation of foreign currency denominated balances of Clene Australia and Clene Netherlands to U.S. dollars for consolidation and unrealized gain (loss) on available-for-sale securities.
Net Loss Per Share Attributable to Common Stockholders
Basic net loss per share attributable to common stockholders is calculated using our weighted-average outstanding common shares. Diluted net loss per share attributable to common stockholders is calculated using our weighted-average outstanding common shares including the dilutive effect of securities as determined under the treasury stock method, except for the dilutive effect of convertible notes payable, which is calculated under the if-converted method, even if the embedded conversion option is out-of-the-money. In periods in which we report a net loss attributable to common stockholders, diluted net loss per share attributable to common stockholders is the same as basic net loss per share attributable to common stockholders, since dilutive common shares are not assumed to have been issued if their effect is anti-dilutive.
Segment Information
We report segment information based on ASC 280 Segment Reporting (“ASC 280”), which defines operating segments as components of a company that engage in activities from which it may recognize revenues and incur expenses, and for which operating results are regularly reviewed by the entity’s chief operating decision maker (“CODM”) to make decisions regarding resource allocation and assess performance, and for which discrete financial information is available. Effective in the fourth quarter of 2023, we have revised our internal reporting processes to better align with our strategic priorities due to the immateriality of our dietary supplement operations. As a result and in accordance with ASC 280, we have determined that the Company is a single operating and reportable segment. Our chief executive officer is the CODM and allocates resources and assesses performance at a consolidated level. Previously, we operated as two operating and reportable segments related to our development and commercialization of drugs and dietary supplements. The change did not require any prior period information to be recast.
Income Taxes
We account for income taxes using the asset and liability method, which requires the recognition of deferred tax assets and liabilities for the expected future tax consequences of events that have been recognized in the consolidated financial statements or in our tax returns. Deferred tax assets and liabilities are determined based on the differences between the financial statement basis and tax basis of assets and liabilities using enacted tax rates in effect for the year in which the differences are expected to reverse. Changes in deferred tax assets and liabilities are recorded in the provision for income taxes. We assess the likelihood that our deferred tax assets will be recovered from future taxable income and, to the extent we believe, based upon the weight of available evidence, that it is more likely than not that all or a portion of the deferred tax assets will not be realized, a valuation allowance is established through a charge to income tax expense. Potential for recovery of deferred tax assets is evaluated by estimating the future taxable profits expected and considering prudent and feasible tax planning strategies.
We account for uncertainty in income taxes recognized in the consolidated financial statements by applying a two-step process to determine the amount of tax benefit to be recognized. First, the tax position must be evaluated to determine the likelihood that it will be sustained upon external examination by the taxing authorities. If the tax position is deemed more-likely-than-not to be sustained, the tax position is then assessed to determine the amount of benefit to recognize in the consolidated financial statements. The amount of the benefit that may be recognized is the largest amount that has a greater than 50% likelihood of being realized upon ultimate settlement. The provision for income taxes includes the effects of any resulting tax reserves, or unrecognized tax benefits, which are considered appropriate as well as the related net interest and penalties.
Stock-Based Compensation
We account for stock-based compensation arrangements using a fair value-based method for costs related to all share-based payments including stock options and stock awards. Stock-based compensation expense is recorded in research and development and general and administrative expenses based on the classification of the work performed by the grantees. The fair value is recognized over the period during which a grantee is required to provide services in exchange for the option award and service-based stock awards, known as the requisite service period (usually the vesting period), on a straight-line basis. For stock awards with market conditions, the fair value is recognized over the period based on the expected milestone achievement dates as the derived service period (usually the vesting period), on a straight-line basis. For stock awards with performance conditions, the grant-date fair value of these awards is the market price on the applicable grant date, and compensation expense will be recognized when the conditions become probable of being satisfied. We recognize a cumulative true-up adjustment once the conditions become probable of being satisfied as the related service period had been completed in a prior period. We elect to account for forfeitures as they occur, rather than estimating expected forfeitures. We determine the fair value of each share of Common Stock underlying stock-based awards using a Black-Scholes option pricing model based on the closing price of our Common Stock as reported by Nasdaq on the date of grant. The fair value of stock awards with market conditions are determined using a Monte Carlo valuation model.
Research and Development
Research and development costs are expensed as incurred. We account for nonrefundable advance payments for goods and services that will be used in future research and development activities as expenses when the goods have been received or when the service has been performed. Research and development expenses consist of costs incurred for the discovery and development of our product candidates. Research and development costs include, but are not limited to, payroll and personnel expenses including stock-based compensation, clinical trial supplies, fees for clinical trial services, consulting costs, and allocated overhead, including rent, equipment, and utilities.
Clinical Trial Accrual
Our clinical trial accrual process accounts for expenses resulting from obligations under contracts with CROs, consultants, and under clinical site agreements in connection with conducting clinical trials. The financial terms of these contracts are subject to negotiations, which vary from contract to contract and may result in payment flows that do not match the periods over which materials or services are provided to us under such contracts. We estimate accruals for the progress of contract completion at each reporting date based upon the facts and circumstances known to us at that time and through discussion and reporting from applicable personnel and service providers. Clinical trial costs are charged to research and development expense in the period in which services and efforts are expended. In the event advance payments are made to a CRO, the payments will be recorded as a prepaid asset which will be amortized to research and development expense over the period the contracted services are performed. CRO contracts generally include pass-through costs including, but not limited to, regulatory expenses, investigator fees, travel costs, shipping costs, printing fees, and other miscellaneous costs. In addition to pass-through costs, we generally incur costs in clinical trials in four distinct groups as follows:
| ● | CRO Start-Up—Start-up costs usually occur within a few months after the contract has been executed and include the initial study initiation, setup of the clinical trial, site recruitment, regulatory applications, investigator meetings, screening, preparation, pre-study visits, and training. These costs are expensed ratably over the start-up period when such period is identifiable or expensed as incurred when no such period is identifiable. |
| ● | CRO Site and Study Management—Site and study management costs include medical and safety monitoring, patient administration and data management. These costs are usually calculated on a per-patient basis and expensed ratably over the treatment period beginning on the date the patient enrolls. |
| ● | CRO Close-Down and Reporting—Close-down and reporting costs include analyzing data and reporting results from the study, which occurs after patients have ceased treatment and the clinical database is locked. These costs are expensed as incurred over the course of the close-down and reporting period when such period is identifiable or expensed as incurred when no such period is identifiable. |
| ● | Third-Party Contracts—Third-party contract costs include fees charged by third parties for various support services which are not provided by CROs, such as fees for laboratories, data quality review, inventory control, and investigational product monitoring. These costs are expensed ratably over the service period with the engaged third-parties when such period is identifiable or expensed as incurred when no such period is identifiable. |
Recently Adopted Accounting Pronouncements
In June 2016, the FASB issued ASU 2016-13, Financial Instruments—Credit Losses (Topic 326): Measurement of Credit Losses on Financial Instruments. The amendments in this update, among other things, require the measurement of all expected credit losses for financial assets held at the reporting date based on historical experience, current conditions, and reasonable and supportable forecasts. Financial institutions and other organizations will now use forward-looking information to better inform their credit loss estimates. As a smaller reporting company, the guidance was effective for our fiscal years beginning after December 15, 2022. The adoption of this guidance did not have an impact on our consolidated financial statements.
Recent Accounting Pronouncements Not Yet Adopted
In November 2023, the FASB issued ASU 2023-07, Segment Reporting (Topic 280): Improvements to Reportable Segment Disclosures (“ASU 2023-07”). ASU 2023-07 requires, among other things, that public entities with a single reportable segment provide all the disclosures required by ASC 280 and ASU 2023-07, and that public entities provide all annual disclosures about a reportable segment’s profit or loss and assets currently required in interim periods. The guidance is effective for fiscal years beginning after December 15, 2023, and interim periods within fiscal years beginning after December 15, 2024. We are currently evaluating the impact of ASU 2023-07.
In December 2023, the FASB issued ASU 2023-09, Income Taxes (Topic 740): Improvements to Income Tax Disclosures (“ASU 2023-09”). ASU 2023-09 requires, among other things, that public entities on an annual basis disclose specific categories of the tax rate reconciliation, provide additional information for reconciling items that meet a quantitative threshold, and disclose income taxes paid disaggregated by jurisdiction. The guidance is effective for annual periods beginning after December 15, 2024. We are currently evaluating the impact of ASU 2023-09.
Note 3. Cash, Cash Equivalents, and Marketable Securities
Available-for-Sale Securities
Available-for-sale securities as of December 31, 2023 were as follows:
| December 31, 2023 | ||||||||||||||||
| (in thousands) | Amortized Cost | Gross Unrealized Gains | Gross Unrealized Losses | Fair Value | ||||||||||||
| Cash equivalents (contractual maturity within 90 days): | ||||||||||||||||
| U.S. Treasury securities | $ | $ | $ | $ | ||||||||||||
| Money market funds | ||||||||||||||||
| Total cash equivalents | ||||||||||||||||
| Cash | ||||||||||||||||
| Total cash and cash equivalents | $ | $ | $ | $ | ||||||||||||
| Marketable securities (contractual maturity greater than 90 days but less than 1 year): | ||||||||||||||||
| U.S. Treasury securities | ||||||||||||||||
| Total marketable securities | $ | $ | $ | $ | ||||||||||||
Available-for-sale securities as of December 31, 2022 were as follows:
| December 31, 2022 | ||||||||||||||||
| (in thousands) | Amortized Cost | Gross Unrealized Gains | Gross Unrealized Losses | Fair Value | ||||||||||||
| Cash equivalents (contractual maturity within 90 days): | ||||||||||||||||
| Money market funds | $ | $ | $ | $ | ||||||||||||
| Total cash equivalents | ||||||||||||||||
| Cash | ||||||||||||||||
| Total cash and cash equivalents | $ | $ | $ | $ | ||||||||||||
| Marketable securities (contractual maturity greater than 90 days but less than 1 year): | ||||||||||||||||
| Commercial paper | $ | $ | $ | ( | ) | $ | ||||||||||
| Corporate debt securities | ||||||||||||||||
| Total marketable securities | $ | $ | $ | ( | ) | $ | ||||||||||
Proceeds from the sale and maturity of marketable securities held as available-for-sale were as follows:
| Year Ended December 31, | ||||||||
| (in thousands) | 2023 | 2022 | ||||||
| Proceeds from maturities of marketable securities | $ | $ | ||||||
| Proceeds from sales of marketable securities | ||||||||
| Total | $ | $ | ||||||
Realized gains and losses included in earnings from the sale of available-for-sale securities were insignificant. As of December 31, 2023 and 2022, we did have any allowance for credit losses or impairments of available-for-sale securities.
Note 4. Prepaid Expenses and Other Current Assets
Prepaid expenses and other current assets as of December 31, 2023 and 2022 were as follows:
| December 31, |
December 31, |
|||||||
| (in thousands) |
2023 |
2022 |
||||||
| Research and development tax credits receivable |
$ | $ | ||||||
| Metals to be used in research and development |
||||||||
| Other |
||||||||
| Total prepaid expenses and other current assets |
$ | $ | ||||||
Note 5. Property and Equipment, Net
Property and equipment, net, as of December 31, 2023 and 2022 were as follows:
| December 31, |
December 31, |
|||||||
| (in thousands) |
2023 |
2022 |
||||||
| Lab equipment |
$ | $ | ||||||
| Office equipment |
||||||||
| Computer software |
||||||||
| Leasehold improvements |
||||||||
| Construction in progress |
||||||||
| Less accumulated depreciation |
( |
) | ( |
) | ||||
| Total property and equipment, net |
$ | $ | ||||||
Depreciation expense recorded in research and development expense and general and administrative expense for the years ended December 31, 2023 and 2022 was as follows:
| Year Ended December 31, |
||||||||
| (in thousands) |
2023 |
2022 |
||||||
| General and administrative |
$ | $ | ||||||
| Research and development |
||||||||
| Total depreciation expense |
$ | $ | ||||||
Note 6. Accrued Liabilities
Accrued liabilities as of December 31, 2023 and 2022 were as follows:
| December 31, |
December 31, |
|||||||
| (in thousands) |
2023 |
2022 |
||||||
| Accrued compensation and benefits |
$ | $ | ||||||
| Accrued CRO and clinical fees |
||||||||
| Other |
||||||||
| Total accrued liabilities |
$ | $ | ||||||
Note 7. Leases
We lease laboratory and office space and certain laboratory equipment under non-cancellable operating and finance leases. The carrying value of our right-of-use lease assets is substantially concentrated in our real estate leases, while the volume of lease agreements is primarily concentrated in equipment leases. We expect that, in the normal course of business, the existing leases will be renewed or replaced by similar leases.
Operating Leases
Operating leases primarily consist of real estate leases for office and laboratory space. We have
As of December 31, 2023 and 2022, our operating lease obligations had a weighted-average discount rate of
Finance Leases
Assets recorded under finance lease obligations and included within property and equipment as of December 31, 2023 and 2022 were as follows:
| December 31, |
December 31, |
|||||||
| (in thousands) |
2023 |
2022 |
||||||
| Lab equipment |
$ | $ | ||||||
| Work in process |
||||||||
| Total |
||||||||
| Less accumulated depreciation |
( |
) | ( |
) | ||||
| Net |
$ | $ | ||||||
As of December 31, 2023 and 2022, our finance lease obligations had a weighted-average interest rate of
Maturity Analysis of Lease Obligations
The maturity analysis of our finance and operating lease obligations as of December 31, 2023 was as follows:
| (in thousands) |
Finance Leases |
Operating Leases |
||||||
| 2024 |
||||||||
| 2025 |
||||||||
| 2026 |
||||||||
| 2027 |
||||||||
| 2028 |
||||||||
| Thereafter |
||||||||
| Total minimum lease payments |
||||||||
| Less amount representing interest/discounting |
( |
) | ||||||
| Present value of minimum lease payments |
||||||||
| Less lease obligations, current portion |
( |
) | ( |
) | ||||
| Lease obligations, net of current portion |
$ | $ | ||||||
Components of Lease Cost
The components of finance and operating lease costs for the years ended December 31, 2023 and 2022 were as follows:
| Year Ended December 31, | ||||||||
| (in thousands) |
2023 |
2022 |
||||||
| Finance lease costs: |
||||||||
| Amortization |
$ | $ | ||||||
| Interest on lease liabilities |
||||||||
| Operating lease costs |
||||||||
| Short-term lease costs |
||||||||
| Variable lease costs |
||||||||
| Total lease costs |
$ | $ | ||||||
Supplemental Cash Flow Information
| Year Ended December 31, | ||||||||
| (in thousands) |
2023 |
2022 |
||||||
| Operating cash flows from operating leases |
$ | ( |
) | $ | ( |
) | ||
| Operating cash flows from finance leases |
$ | ( |
) | $ | ( |
) | ||
| Financing cash flows from finance leases |
$ | ( |
) | $ | ( |
) | ||
Note 8. Notes Payable and Convertible Notes Payable
Our notes payable and convertible notes payable as of December 31, 2023 and 2022 was as follows:
| Stated |
December 31, |
December 31, |
||||||||||
| (in thousands, except interest rates) |
Interest Rate |
2023 |
2022 |
|||||||||
| Notes payable |
||||||||||||
| Advance Cecil, Inc. (commenced April 2019) |
% | $ | $ | |||||||||
| Maryland DHCD (commenced February 2019) |
% | |||||||||||
| Maryland DHCD (commenced May 2022) |
% | |||||||||||
| Avenue Venture Opportunities Fund, L.P. (commenced May 2021) |
% | |||||||||||
| Less unamortized discount and debt issuance costs |
( |
) | ( |
) | ||||||||
| Less notes payable, current portion, net of unamortized discount and debt issuance costs |
( |
) | ( |
) | ||||||||
| Total notes payable, net of current portion |
$ | $ | ||||||||||
| Convertible notes payable |
||||||||||||
| Avenue Venture Opportunities Fund, L.P. (commenced May 2021) |
% | $ | $ | |||||||||
| Maryland DHCD (commenced December 2022) |
% | |||||||||||
| 10,308 | 10,007 | |||||||||||
| Less unamortized discount and debt issuance costs |
( |
) | ( |
) | ||||||||
| Less convertible notes payable, current portion, net of unamortized discount and debt issuance costs |
( |
) | ||||||||||
| Total convertible notes payable, net of current portion |
$ | $ | ||||||||||
Maryland Loans
In February 2019, we entered into a term loan agreement (the “2019 MD Loan”) with the Department of Housing and Community Development (“DHCD”), a principal department of the State of Maryland, for $
In April 2019, we entered into a term loan agreement (the “2019 Cecil Loan”) with Advance Cecil Inc., a non-stock corporation formed under the laws of the State of Maryland, for $
In May 2022, we entered into a term loan agreement (the “2022 MD Loan”) with DHCD for up to $
In December 2022, we entered into a term loan agreement (the “2022 DHCD Loan”) with DHCD for $
Avenue Loan
In May 2021, we entered into a term loan agreement (the “2021 Avenue Loan”) with Avenue for up to $
At any time between May 21, 2022, and May 21, 2024, Avenue may, in its sole discretion, convert up to $
We are subject to covenants until maturity, including limitations on our ability to retire, repurchase, or redeem our stock, options, and warrants other than per the terms of the securities; limitations on our ability to pay dividends; and we are required to maintain unrestricted cash and cash equivalents of at least $
At the inception of the 2021 Avenue Loan, we issued a warrant to Avenue to purchase
Debt Maturities
Future debt payments, net of unamortized discounts and debt issuance costs, and without giving effect to any potential future exercise of conversion features, are as follows:
| (in thousands) |
2019 MD Loan |
2019 Cecil Loan |
2021 Avenue Loan |
2022 MD Loan |
2022 DHCD Loan |
|||||||||||||||
| 2024 |
$ | $ | $ | $ | $ | |||||||||||||||
| 2025 |
||||||||||||||||||||
| 2026 |
||||||||||||||||||||
| 2027 |
||||||||||||||||||||
| 2028 |
||||||||||||||||||||
| Thereafter |
||||||||||||||||||||
| Total debt principal payments |
||||||||||||||||||||
| Accrued and unpaid interest |
||||||||||||||||||||
| Less unamortized discount and debt issuance costs |
( |
) | ( |
) | ( |
) | ||||||||||||||
| Future debt payments, net |
$ | $ | $ | $ | $ | |||||||||||||||
Note 9. Commitments and Contingencies
Commitments
We enter into agreements in the normal course of business with CROs for clinical trials and with vendors for preclinical studies and other services and products for operating purposes, which are cancelable at any time by us, subject to payment of our remaining obligations under binding purchase orders and, in certain cases, nominal early termination fees. These commitments are not deemed significant.
As of December 31, 2023 and 2022, we had commitments under various agreements for capital expenditures totaling $
Contingencies
From time to time, we may have certain contingent legal liabilities that arise in the ordinary course of business activities. We accrue a liability for such matters when it is probable that future expenditures will be made, and such expenditures can be reasonably estimated. We are not aware of any current material pending legal matters or claims.
We received the following grants from the National Multiple Sclerosis Society (“NMSS”): (i) $
Note 10. Income Taxes
The components of loss before income taxes for the years ended December 31, 2023 and 2022 were as follows:
| Year Ended December 31, | ||||||||
| (in thousands) | 2023 | 2022 | ||||||
| United States | $ | ( | ) | $ | ( | ) | ||
| Foreign | ( | ) | ( | ) | ||||
| Net loss before income taxes | $ | ( | ) | $ | ( | ) | ||
We had
| Year Ended December 31, | ||||||||
| (in thousands) | 2023 | 2022 | ||||||
| Income tax expense (benefit) at federal statutory rate | $ | ( | ) | $ | ( | ) | ||
| State income taxes (net of federal benefit) | ( | ) | ( | ) | ||||
| Loss on initial issuance of equity | — | |||||||
| Change in fair value of common stock warrant liabilities | ( | ) | ( | ) | ||||
| Change in fair value of contingent earn-outs | ( | ) | ( | ) | ||||
| Research and development tax credits | ( | ) | ( | ) | ||||
| Stock compensation | ( | ) | ||||||
| Foreign rate differential | ( | ) | ( | ) | ||||
| Adjustment for change in tax rate | ( | ) | ||||||
| Other | ( | ) | ||||||
| Change in valuation allowance | ||||||||
| Income tax benefit | $ | — | $ | — | ||||
Our effective tax rate was
| December 31, | December 31, | |||||||
| (in thousands) | 2023 | 2022 | ||||||
| Deferred tax assets (liabilities): | ||||||||
| Net operating loss carryforwards | $ | $ | ||||||
| Depreciation and amortization | ||||||||
| Research and development tax credits | ||||||||
| Lease liability | ||||||||
| Right-of-use asset | ( | ) | ( | ) | ||||
| Capitalized research and development expenses | ||||||||
| Non-qualified stock options and restricted stock awards | ||||||||
| Accrued compensation | ||||||||
| Other | ( | ) | ||||||
| Total deferred tax assets (liabilities) | ||||||||
| Less: valuation allowance | ( | ) | ( | ) | ||||
| Net deferred tax assets (liabilities) | $ | $ | ||||||
In assessing the realizability of deferred tax assets, we consider whether it is more likely than not that some portion or all of the deferred tax assets will not be realized. The ultimate realization of deferred tax assets is dependent upon the generation of future taxable income during periods in which those temporary differences become deductible. We consider the scheduled reversal of deferred tax liabilities, projected future taxable income, carry back opportunities and tax planning strategies in making the assessment. We believe it is more likely than not that we will not realize the benefits of these deductible differences and have applied a full valuation allowance against them.
We have federal and state net operating losses (“NOLs”) of approximately $
Under the provisions of Section 382 of the Internal Revenue Code of 1986, substantial changes in our ownership may result in limitations on the amount of NOL carryforwards and research and development credits that can be utilized in future years. NOL carryforwards and research and development credits are subject to examination in the year they are utilized regardless of whether the tax year in which they are generated has been closed by statute. The amount subject to disallowance is limited to the amount utilized. Accordingly, we may be subject to examination for prior NOLs and credits generated as such tax attributes are utilized.
We have recorded any amounts for unrecognized tax benefits as of December 31, 2023 and 2022. We recognize interest and penalties related to income tax matters in income tax expense. We have accrual of interest and penalties on the consolidated balance sheets and have recognized interest and penalties in the consolidated statements of operations and comprehensive loss for the years ended December 31, 2023 and 2022.
We are subject to taxation in the U.S., Australia, Netherlands, and various state jurisdictions. Our tax returns from to present are subject to examination by the U.S. and state authorities due to the carry forward of unutilized net operating losses and research and development credits. We currently have no pending examinations. The primary difference between the effective tax rate and the federal statutory tax rate relates to the full valuation allowance on our net operating losses and other deferred tax assets.
Note 11. Benefit Plans
401(k) Plan
Our 401(k) plan is a deferred salary arrangement under Section 401(k) of the Internal Revenue Code. We match
Stock Compensation Plans
The Clene Nanomedicine, Inc. 2014 Stock Plan (the “2014 Plan”) was adopted in July 2014. Effective as of the closing of the Reverse Recapitalization, no additional awards may be granted under the 2014 Plan. As of December 31, 2023,
The Clene Inc. 2020 Amended Stock Plan (the “2020 Plan”) was adopted in December 2020 and amended in May 2023 and
Stock-Based Compensation Expense
Stock-based compensation expense recorded in research and development expense and general and administrative expense for the years ended December 31, 2023 and 2022 was as follows:
| Year Ended December 31, |
||||||||
| (in thousands) |
2023 |
2022 |
||||||
| General and administrative |
$ | $ | ||||||
| Research and development |
||||||||
| Total stock-based compensation expense |
$ | $ | ||||||
Stock-based compensation expense by award type for the years ended December 31, 2023 and 2022 was as follows:
| Year Ended December 31, |
||||||||
| (in thousands) |
2023 |
2022 |
||||||
| Stock options |
$ | $ | ||||||
| Stock awards |
||||||||
| Total stock-based compensation expense |
$ | $ | ||||||
Stock Options
Outstanding stock options and related activity for the year ended December 31, 2023 was as follows:
| (in thousands, except share, per share, and term data) |
Number of Options |
Weighted Average Exercise Price Per Share |
Weighted Average Remaining Term (Years) |
Intrinsic Value |
||||||||||||
| Outstanding – December 31, 2022 |
$ | $ | ||||||||||||||
| Granted |
— | |||||||||||||||
| Forfeited |
( |
) | — | — | ||||||||||||
| Outstanding – December 31, 2023 |
$ | $ | ||||||||||||||
| Vested and exercisable – December 31, 2023 |
$ | $ | ||||||||||||||
| Vested, exercisable or expected to vest – December 31, 2023 |
$ | $ | ||||||||||||||
As of December 31, 2023 and 2022, we had approximately $
The weighted-average grant-date fair value of stock options granted during the year ended December 31, 2023 and 2022 was $
| Year Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Expected stock price volatility | 96.22% –103.31 | 89.57% –99.77 | ||||||
| Risk-free interest rate | 3.26% –4.66 | 1.65% –4.31 | ||||||
| Expected dividend yield | % | % | ||||||
| Expected term of options (in years) | 5.00 –6.43 | 5.00 –6.98 | ||||||
Stock Awards
Stock awards include rights to restricted stock awards with market-based vesting conditions and restricted stock units with service-based vesting conditions. Outstanding stock awards and related activity for the year ended December 31, 2023 was as follows:
| Number of Stock Awards |
Weighted Average Grant Date Fair Value |
|||||||
| Unvested balance – December 31, 2022 |
$ | |||||||
| Granted |
||||||||
| Converted to shares of Common Stock upon vesting |
( |
) | ||||||
| Forfeited |
( |
) | ||||||
| Unvested balance – December 31, 2023 |
$ | |||||||
As of December 31, 2023, we had $
Note 12. Fair Value
Cash, cash equivalents, and marketable securities are carried at fair value. Financial instruments, including accounts receivable, accounts payable, and accrued expenses are carried at cost, which approximates fair value given their short-term nature. Our remaining fair value measures are discussed below.
Financial Instruments with Fair Value Measurements on a Recurring Basis
The fair value hierarchy for financial instruments measured at fair value on a recurring basis as of December 31, 2023 is as follows:
| December 31, 2023 |
||||||||||||||||
| (in thousands) |
Level 1 |
Level 2 |
Level 3 |
Total |
||||||||||||
| Cash equivalents: |
||||||||||||||||
| U.S. Treasury securities |
$ | $ | $ | $ | ||||||||||||
| Money market funds |
||||||||||||||||
| Marketable securities: |
||||||||||||||||
| U.S. Treasury securities |
||||||||||||||||
| Common stock warrant liabilities |
||||||||||||||||
| Clene Nanomedicine contingent earn-out liability |
||||||||||||||||
| Initial Stockholders contingent earn-out liability |
||||||||||||||||
The fair value hierarchy for financial instruments measured at fair value on a recurring basis as of December 31, 2022 is as follows:
| December 31, 2022 |
||||||||||||||||
| (in thousands) |
Level 1 |
Level 2 |
Level 3 |
Total |
||||||||||||
| Cash equivalents: |
||||||||||||||||
| Money market funds |
$ | $ | $ | $ | ||||||||||||
| Marketable securities: |
||||||||||||||||
| Commercial paper |
||||||||||||||||
| Corporate debt securities |
||||||||||||||||
| Clene Nanomedicine contingent earn-out liability |
||||||||||||||||
| Initial Stockholders contingent earn-out liability |
||||||||||||||||
There were no transfers between Level 1, Level 2, or Level 3 during any of the periods above.
Changes in the fair value of our Level 3 financial instruments for the year ended December 31, 2023 were as follows:
| (in thousands) |
Common Stock Warrant Liabilities |
Clene Nanomedicine Contingent Earn-out |
Initial Stockholders Contingent Earn-out |
|||||||||
| Balance – December 31, 2022 |
$ | $ | $ | |||||||||
| Initial fair value of instruments |
||||||||||||
| Change in fair value |
( |
) | ( |
) | ( |
) | ||||||
| Balance – December 31, 2023 |
$ | $ | $ | |||||||||
Changes in the fair value of our Level 3 financial instruments for the year ended December 31, 2022 were as follows:
| (in thousands) |
Common Stock Warrant Liabilities |
Clene Nanomedicine Contingent Earn-out |
Initial Stockholders Contingent Earn-out |
|||||||||
| Balance – December 31, 2021 |
$ | $ | $ | |||||||||
| Change in fair value |
( |
) | ( |
) | ||||||||
| Reclassification from liability to equity |
( |
) | ||||||||||
| Extinguishment of instrument |
( |
) | ||||||||||
| Balance – December 31, 2022 |
$ | $ | $ | |||||||||
Valuation of Notes Payable and Convertible Notes Payable
The 2019 MD Loan and the 2019 Cecil Loan are carried at the greater of principal plus accrued interest or the value of the Phantom Shares (see Note 8) which approximates fair value. The 2021 Avenue Loan, the 2022 MD Loan, and the 2022 DHCD Loan are carried at amortized cost, which approximates fair value due to our credit risk and market interest rates. Our notes payable and convertible notes payable are categorized within Level 3 of the fair value hierarchy.
Valuation of the Common Stock Warrant Liabilities
The Original Avenue Warrant, comprised of the Tranche 1 warrant and the contingently issuable Tranche 2 warrant to purchase shares of Common Stock, was classified as a liability and recorded at fair value at inception of the 2021 Avenue Loan. As of March 31, 2022, we reclassified the Tranche 1 warrant to additional paid-in capital. Our ability to draw Tranche 2 expired on December 31, 2022 and the warrant liability was extinguished and we recognized income of $
The New Avenue Warrant is classified as a liability and carried at fair value. We estimate the fair value using a Black-Scholes option-pricing model with probability weights for the occurrence of the following events: (i) settlement of the instrument upon a change of control transaction, (ii) dissolution of the Company, or (iii) another outcome outside of (i)-(ii). These estimates require significant judgment. The carrying amount may fluctuate significantly and the actual settlement amount may be materially different from the estimated fair value. The unobservable inputs to the Black-Scholes option pricing model were as follows:
| December 31, | ||||
| 2023 | ||||
| Expected stock price volatility | 105.00% –110.00 | |||
| Risk-free interest rate | 3.88% –5.03 | |||
| Expected dividend yield | % | |||
| Expected term (in years) | 0.75 –4.5 | |||
| Probability of change of control | % | |||
| Probability of dissolution | % | |||
| Probability of other outcome | % | |||
The Tranche A Warrants are classified as a liability and carried at fair value (the Tranche B Warrants qualified for equity classification at issuance). We estimate the fair value using a Black-Scholes option-pricing model with probability weights for the occurrence of the following events: (i) FDA acceptance of an NDA for CNM-Au8, (ii) settlement upon a fundamental transaction, (iii) dissolution of the Company, and (iv) another outcome outside of (i)-(iii). These estimates require significant judgment. The carrying amount may fluctuate significantly and the actual settlement amount may be materially different from the estimated fair value. The unobservable inputs to the Black-Scholes option pricing model were as follows:
| December 31, | ||||
| 2023 | ||||
| Expected stock price volatility | 100.00% –110.00 | |||
| Risk-free interest rate | 4.13% –4.74 | |||
| Expected dividend yield | % | |||
| Expected term (in years) | 1.08 –2.46 | |||
| Probability of NDA acceptance | % | |||
| Probability of fundamental transaction | % | |||
| Probability of dissolution | % | |||
| Probability of other outcome | % | |||
Valuation of the Contingent Earn-Out Liabilities
The Contingent Earn-outs are carried at fair value, determined using a Monte Carlo valuation model in order to simulate the future path of our stock price over the earn-out periods. The carrying amount of the liabilities may fluctuate significantly and actual amounts paid may be materially different from the liabilities’ estimated value. The unobservable inputs to the Monte Carlo valuation model were as follows:
| December 31, |
December 31, |
|||||||
| 2023 |
2022 |
|||||||
| Expected stock price volatility |
% | % | ||||||
| Risk-free interest rate |
% | % | ||||||
| Expected dividend yield |
% | % | ||||||
| Expected term (in years) |
||||||||
Note 13. Capital Stock
As of December 31, 2023 and 2022, our amended and restated certificate of incorporation authorized us to issue
Our common stockholders are entitled to one vote per share and to notice of any stockholders’ meeting. Voting, dividend, and liquidation rights of the holders of Common Stock are subject to the prior rights of holders of all classes of stock and are qualified by the rights, powers, preferences, and privileges of the holders of preferred stock. No distributions shall be made with respect to Common Stock until all declared dividends to preferred stock have been paid or set aside for payment. Common Stock is not redeemable at the option of the holder.
Common Stock Warrants
As of December 31, 2023 and 2022, outstanding warrants to purchase shares of Common Stock were as follows:
| Number of Shares Issuable | ||||||||||||||||
| December 31, | December 31, | |||||||||||||||
| Date Exercisable | Exercise Price | Expiration | Classification | 2023 | 2022 | |||||||||||
| December 2020 | $ | December 2025 | (1) | Equity | ||||||||||||
| December 2020 | $ | December 2025 | (2) | Equity | ||||||||||||
| December 2020 | $ | April 2023 | (3) | Equity | ||||||||||||
| May 2021 | $ | May 2026 | (4) | Equity | ||||||||||||
| June 2023 | $ | June 2028 | (5) | Liability | ||||||||||||
| June 2023 | $ | June 2026 | (6) | Liability | ||||||||||||
| June 2023 | $ | June 2030 | (7) | Equity | ||||||||||||
| Total | ||||||||||||||||
| (1) | Represents |
| (2) | Represents |
| (3) | Represents |
| (4) | Represents |
| (5) | Represents |
| (6) | Represents |
| (7) | Represents |
Public Offerings
In October 2022, we sold
In June 2023, we sold
Common Stock Sales Agreement
In April 2022, we entered into an Equity Distribution Agreement which we amended in December 2022 (the “ATM Agreement”). Canaccord acts as placement agent and we may offer and sell shares of Common Stock from time to time through Canaccord having an aggregate offering place of up to $
Pursuant to the ATM Agreement, Canaccord is not required to sell any specific number or dollar amount of Common Stock but will act as our placement agent to sell, on our behalf, all the Common Stock requested by us to be sold, consistent with Canaccord’s normal trading and sales practices, on terms mutually agreed between Canaccord and us. Canaccord is entitled to compensation at a fixed commission rate of
Common Stock Purchase Agreement
In March 2023, we entered into a purchase agreement (the “Purchase Agreement”) with Lincoln Park Capital Fund, LLC (“Lincoln Park”), pursuant to which Lincoln Park committed to purchase up to $
Pursuant to the Purchase Agreement, we may direct Lincoln Park to purchase up to
On the date of the Purchase Agreement, we issued
We evaluated the Purchase Agreement under ASC 815-40 Derivatives and Hedging—Contracts on an Entity's Own Equity as it represents the right to require Lincoln Park to purchase shares of Common Stock in the future, similar to a put option. We concluded it represents a freestanding derivative instrument that does not qualify for equity classification and therefore requires fair value accounting. We analyzed the terms of the contract and concluded the derivative instrument has
Note 14. Net Loss Per Share
The computation of basic and diluted net loss per share attributable to common stockholders for the years ended December 31, 2023 and 2022 was as follows:
| Year Ended December 31, |
||||||||
| (in thousands, except share and per share data) |
2023 |
2022 |
||||||
| Numerator: |
||||||||
| Net loss attributable to common stockholders |
$ | ( |
) | $ | ( |
) | ||
| Denominator: |
||||||||
| Weighted average common shares outstanding |
||||||||
| Net loss per share attributable to common stockholders – basic and diluted |
$ | ( |
) | $ | ( |
) | ||
The following shares of potentially dilutive securities were excluded from the computation of diluted net loss per share attributable to common stockholders for the years ended December 31, 2023 and 2022 because they were antidilutive, out-of-the-money, or the issuance of such shares is contingent upon certain conditions which were not satisfied by the end of the period:
| Year Ended December 31, |
||||||||
| 2023 |
2022 |
|||||||
| Convertible notes payable (see Note 8) |
||||||||
| Common stock warrants (see Note 13) |
||||||||
| Options to purchase common stock (see Note 11) |
||||||||
| Unvested restricted stock awards (see Note 11) |
||||||||
| Contingent earn-out shares (see Note 2) |
||||||||
| Total |
||||||||
Note 15. Related Party Transactions
License and Supply Agreements
In August 2018, we entered into a license agreement (the “License Agreement”) and exclusive supply agreement (the “Supply Agreement”) in conjunction with 4Life’s investment in the Series C preferred stock and warrants of our predecessor.
| ● |
License Agreement. We granted 4Life an exclusive and royalty-bearing license to develop, manufacture, and sell certain non-pharmaceutical, low-concentration dietary supplement products produced by our electro-crystal-chemistry platform. 4Life pays royalties to us equal to |
| ● |
Supply Agreement. We granted 4Life an exclusive right to purchase certain non-pharmaceutical, low-concentration dietary supplement products produced by our electro-crystal-chemistry platform. 4Life’s price to purchase products from us under the Supply Agreement is equal to our fully encumbered manufacturing costs plus |
We currently provide an aqueous zinc-silver ion dietary (mineral) supplement to 4Life on a non-exclusive basis, which is sold by 4Life under the tradename Zinc Factor™; and an aqueous gold dietary (mineral) supplement of very low-concentration gold nanoparticles on an exclusive basis, which is sold by 4Life under the tradename Gold Factor™ and is subject to royalties. Total revenue under the License and Supply Agreements for the years ended December 31, 2023 and 2022 was as follows:
| Year Ended December 31, | ||||||||
| (in thousands) | 2023 | 2022 | ||||||
| Product revenue from related parties | $ | $ | ||||||
| Royalty revenue from related parties | ||||||||
| Total revenue from related parties | $ | $ | ||||||
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None.
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
Under the supervision and with the participation of management, including our principal executive officer and principal financial officer, we conducted an evaluation of the effectiveness of our disclosure controls and procedures as of December 31, 2023, as such term is defined in Rules 13a-15(e) and 15d-15(e) of the Exchange Act. As a result of this evaluation, our principal executive officer and principal financial officer have concluded that, as of December 31, 2023, our disclosure controls and procedures were not effective due to the material weaknesses in internal control over financial reporting described below. Notwithstanding the identified material weaknesses, management, including our principal executive officer and principal financial officer, believes the consolidated financial statements included in this Annual Report on Form 10-K fairly represent, in all material respects, our financial condition, results of operations and cash flows as of and for the periods presented in accordance with U.S. Generally Accepted Accounting Principles.
Disclosure controls and procedures are designed to ensure that information required to be disclosed by us in the reports that we file or submit under the Exchange Act is recorded, processed, summarized, and reported within the time periods specified in the SEC’s rules and forms, and that such information is accumulated and communicated to our management, including our principal executive officer and principal financial officer, as appropriate to allow timely decisions regarding required disclosure.
Management’s Annual Report on Internal Control Over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting, as defined in Rules 13a-15(f) and 15d-15(f) of the Exchange Act. Management has evaluated the effectiveness of our internal control over financial reporting based on criteria established in Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. As a result of this assessment, management has concluded that, as of December 31, 2023, our internal control over financial reporting was not effective due to the material weaknesses in internal control over financial reporting described below. As a smaller reporting company, we are not required to include an attestation report on internal control over financial reporting issued by our independent registered public accounting firm in this Annual Report on Form 10-K.
Material Weaknesses in Internal Control over Financial Reporting
In connection with the audit of our financial statements as of and for the years ended December 31, 2023 and 2022, our management identified material weaknesses in our internal control over financial reporting. A material weakness is a deficiency, or combination of deficiencies, in internal control over financial reporting, such that there is a reasonable possibility that a material misstatement of our annual or interim financial statements will not be prevented or detected on a timely basis. The material weaknesses identified relate to the fact that we did not design or maintain an effective control environment commensurate with our financial reporting requirements. This deficiency in our control environment contributed to the following additional material weaknesses related to control activities and information and communication within our internal control over financial reporting:
| ● |
we did not design and maintain controls over the preparation and review of reconciliations and the review and segregation of duties over manual journal entries, including controls over the completeness and accuracy of information; and |
| ● |
we did not design and maintain information technology (“IT”) general controls for IT systems that are relevant to the preparation of the financial statements. Specifically, we did not design and maintain: (a) user access controls to ensure appropriate segregation of duties and that adequately restrict user and privileged access to financial applications, programs, and data to our appropriate personnel; (b) program change management controls to ensure that IT program and data changes affecting financial IT applications and underlying accounting records are identified, tested, authorized, and implemented appropriately; (c) computer operations controls to ensure that data backups are authorized and monitored; and (d) testing and approval controls for program development to ensure that new software development is aligned with business and IT requirements. |
Each of the control deficiencies described above could result in a misstatement of one or more account balances or disclosures that would result in a material misstatement to the annual or interim consolidated financial statements that would not be prevented or detected. Accordingly, our management has determined that each of the control deficiencies described above constitute material weaknesses.
Material Weakness Remediation
Management continues to be actively engaged and committed to taking the steps necessary to remediate the control deficiencies that constituted the above material weaknesses. During 2023, we made the following enhancements to our control environment:
| ● |
we have continued to strengthen the experience of our internal accounting team through refinement of our processes and internal controls over financial reporting and our IT and technical accounting resources; and |
| ● |
until we have sufficient technical accounting resources, we have engaged external consultants to provide support and to assist us in our evaluation of more complex applications of GAAP. |
We continue to enhance corporate oversight over process-level controls and structures to ensure that there is appropriate assignment of authority, responsibility, and accountability to enable remediation of our material weaknesses. We believe that our remediation plan will be sufficient to remediate the identified material weaknesses and strengthen our internal control over financial reporting. As we continue to evaluate, and work to improve, our internal control over financial reporting, management may determine that additional measures to address control deficiencies or modifications to the remediation plan are necessary.
Changes in Internal Control over Financial Reporting
Other than changes described under “—Material Weakness Remediation” above, there were no changes in our internal control over financial reporting during the quarter ended December 31, 2023, which were identified in connection with management’s evaluation required by paragraph (b) of Rules 13a-15 and 15d-15 under the Exchange Act, that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
During the three months ended December 31, 2023, of the Company’s officers or directors adopted or terminated any “Rule 10b5-1 trading arrangement” or any “non-Rule 10b5-1 trading arrangement,” as each term is defined in Item 408 of Regulation S-K.
Item 9C. Disclosure Regarding Foreign Jurisdictions that Prevent Inspections
Not applicable.
Item 10. Directors, Executive Officers and Corporate Governance
Information required by Item is included in our definitive proxy statement relating to our 2024 Annual Meeting of Stockholders and is incorporated herein by reference. The definitive proxy statement will be filed with the SEC within 120 days after the end of the fiscal year to which this Annual Report relates.
Item 11. Executive Compensation
Information required by Item is included in our definitive proxy statement relating to our 2024 Annual Meeting of Stockholders and is incorporated herein by reference. The definitive proxy statement will be filed with the SEC within 120 days after the end of the fiscal year to which this Annual Report relates.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
Information required by Item is included in our definitive proxy statement relating to our 2024 Annual Meeting of Stockholders and is incorporated herein by reference. The definitive proxy statement will be filed with the SEC within 120 days after the end of the fiscal year to which this Annual Report relates.
Item 13. Certain Relationships and Related Transactions, and Director Independence
Information required by Item is included in our definitive proxy statement relating to our 2024 Annual Meeting of Stockholders and is incorporated herein by reference. The definitive proxy statement will be filed with the SEC within 120 days after the end of the fiscal year to which this Annual Report relates.
Item 14. Principal Accountant Fees and Services
Information required by Item is included in our definitive proxy statement relating to our 2024 Annual Meeting of Stockholders and is incorporated herein by reference. The definitive proxy statement will be filed with the SEC within 120 days after the end of the fiscal year to which this Annual Report relates.
Item 15. Exhibit and Financial Statement Schedules
| (a) |
Documents filed as part of this Annual Report: |
| (1) |
Financial Statements: |
Report of Independent Registered Public Accounting Firm
Consolidated Balance Sheets
Consolidated Statements of Operations and Comprehensive Loss
Consolidated Statements of Stockholders’ Equity
Consolidated Statements of Cash Flows
Notes to Consolidated Financial Statements
| (2) |
Financial Statement Schedules: |
All schedules have been omitted because the required information is included in the consolidated financial statements or the notes thereto, or because it is not required.
| (3) |
Exhibits: |
See exhibits listed under Part (b) below.
| (b) |
Exhibits: |
| * |
Filed herewith. |
| ** |
Furnished herewith. |
| # |
Management contract or compensatory plan or agreement. |
| ## |
Schedules and similar attachments to this exhibit have been omitted pursuant to Item 601(a)(5) of Regulation S-K. We agree to furnish supplementally a copy of such omitted materials to the SEC upon request. |
| † |
Certain portions of this exhibit have been redacted pursuant to Item 601(b)(10)(iv) of Regulation S-K. We agree to furnish supplementally an unredacted copy to the SEC upon request. |
None.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
CLENE INC. |
|
|
|
|
|
| Date: March 13, 2024 |
By: |
/s/ Robert Etherington |
|
|
Robert Etherington |
|
|
|
President, Chief Executive Officer and Director |
|
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed by the following persons on behalf of the registrant in the capacities and on the dates indicated.
| Signature |
|
Title |
|
Date |
|
|
|
|
|
|
| /s/ Robert Etherington |
|
President, Chief Executive Officer and Director |
|
March 13, 2024 |
| Robert Etherington |
|
(Principal Executive Officer) |
|
|
|
|
|
|
|
|
| /s/ Morgan R. Brown |
|
Chief Financial Officer |
|
March 13, 2024 |
| Morgan R. Brown |
|
(Principal Financial and Accounting Officer) |
|
|
|
|
|
|
|
|
| /s/ David J. Matlin |
|
Chairman of the Board |
|
March 13, 2024 |
| David J. Matlin |
|
|
|
|
|
|
|
|
|
|
| /s/ Arjun Desai |
|
Director |
|
March 13, 2024 |
| Arjun Desai |
|
|
|
|
|
|
|
|
|
|
| /s/ Jonathon T. Gay |
|
Director |
|
March 13, 2024 |
| Jonathon T. Gay |
|
|
|
|
|
|
|
|
|
|
| /s/ Shalom Jacobovitz |
|
Director |
|
March 13, 2024 |
| Shalom Jacobovitz |
|
|
|
|
|
|
|
|
|
|
| /s/ Matthew Kiernan |
|
Director |
|
March 13, 2024 |
| Matthew Kiernan |
|
|
|
|
|
|
|
|
|
|
| /s/ Vallerie V. McLaughlin |
|
Director |
|
March 13, 2024 |
| Vallerie V. McLaughlin |
|
|
|
|
|
|
|
|
|
|
| /s/ Alison H. Mosca |
|
Director |
|
March 13, 2024 |
| Alison H. Mosca |
|
|
|
|
| /s/ Reed Neil Wilcox | Director | March 13, 2024 | ||
| Reed Neil Wilcox |