development activities that may include in-licensing activities or partnering certain programs in specific geographies with collaborators, as we have demonstrated through our ongoing collaboration with Neurocrine Biosciences, Inc., which we refer to as Neurocrine. Since our inception, our operations have focused on organizing and staffing our company, business planning, raising capital, establishing our intellectual property portfolio, determining which neurological diseases to pursue, advancing our product candidates including delivery and manufacturing, and conducting preclinical studies and clinical trials. We do not have any product candidates approved for sale and have not generated any revenue from product sales. We have funded our operations primarily through private placements of redeemable convertible preferred stock, public offerings of our common stock, and our strategic collaborations, including our prior collaboration with Sanofi Genzyme Corporation, or the Sanofi Genzyme Collaboration, which commenced in February 2015 and was terminated in June 2019, our prior collaboration with AbbVie Biotechnology Ltd. focusing on tau-related disease, or the AbbVie Tau Collaboration, which commenced in February 2018 and was terminated in August 2020, our prior collaboration with AbbVie Ireland Unlimited Company focusing on pathological species of alpha-synuclein, or the AbbVie Alpha-Synuclein Collaboration, which commenced in February 2019 and was terminated in August 2020, and our ongoing collaboration with Neurocrine, which commenced in March 2019. We refer to our collaboration agreement with Neurocrine as the Neurocrine Collaboration Agreement and the collaboration with Neurocrine as the Neurocrine Collaboration.
Our pipeline of gene therapy programs is summarized in the table below:
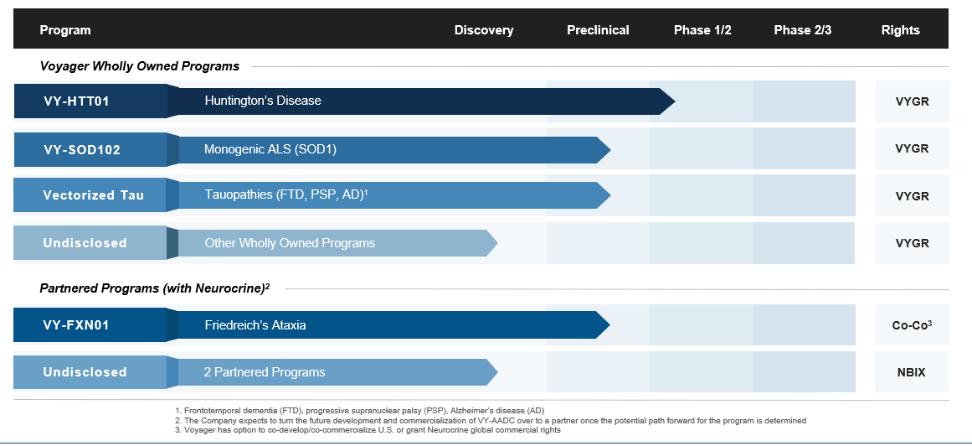
Our pipeline consists of wholly-owned programs for severe neurological indications, including Huntington’s disease; a monogenic form of amyotrophic lateral sclerosis, or ALS; and tau-related diseases including Alzheimer’s disease, frontotemporal dementia, or FTD, and progressive supranuclear palsy, or PSP. We may seek orphan drug designation, breakthrough therapy designation, or other expedited review processes for certain of our product candidates in the United States, Europe, and Japan. Additionally, we continue to partner with Neurocrine on programs for severe neurological diseases including Friedreich’s ataxia.
As part of the Neurocrine Collaboration, we and Neurocrine have been developing VY-AADC (NBIb-1817) for the treatment of Parkinson’s disease, or the VY-AADC Program. VY-AADC (NBIb-1817) is currently being evaluated in the RESTORE-1 Phase 2 clinical trial. The FDA has granted VY-AADC (NBIb-1817) its regenerative medicine advanced therapy, known as RMAT, designation, which provides for an enhanced level of interactions between the company sponsor and the FDA throughout a development program, and has granted VY-AADC (NBIb-1817) fast-track designation.
25