UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM
| ☒ | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
FOR
THE FISCAL YEAR ENDED
| TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
FOR THE TRANSITION PERIOD FROM ________ TO ________.
COMMISSION
FILE NUMBER:
(Exact name of registrant as specified in its charter)
(State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification No.) |
| (Address of principal executive offices) | (Zip Code) |
Registrant’s telephone number, including area code:
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class | Trading Symbol | Name of each exchange where registered | ||
| The
|
Securities registered pursuant to Section 12(g) of the Act: None
Indicate
by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐
Indicate
by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐
Indicate
by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange
Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports),
and (2) has been subject to such filing requirements for the past 90 days.
Indicate
by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant
to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that
the registrant was required to submit such files).
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer ☐ | Accelerated filer ☐ | |
| Non-accelerated filer ☒ | Smaller
reporting company | |
| Emerging
growth company |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. ☐
Indicate
by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ☐
As
of June 30, 2020, the last business day of the registrant’s most recently completed second fiscal quarter, the aggregate
market value of the common stock held by non-affiliates of the registrant was approximately $
As of March 8, 2021, the number of shares outstanding of the registrant’s common stock, $0.0001 par value per share, was .
Documents incorporated by reference
Portions of the registrant’s proxy statement for the 2021 annual meeting of stockholders to be filed pursuant to Regulation 14A within 120 days after the registrant’s fiscal year ended December 31, 2020, are incorporated by reference in Part III of this Form 10-K.
CORBUS PHARMACEUTICALS HOLDINGS, INC.
ANNUAL REPORT ON FORM 10-K
FOR THE YEAR ENDED DECEMBER 31, 2020
TABLE OF CONTENTS
| 2 |
PART I
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS
This report on Form 10-K contains forward-looking statements made pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 under Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. Forward-looking statements include statements with respect to our beliefs, plans, objectives, goals, expectations, anticipations, assumptions, estimates, intentions and future performance, and involve known and unknown risks, uncertainties and other factors, which may be beyond our control, and which may cause our actual results, performance or achievements to be materially different from future results, performance or achievements expressed or implied by such forward-looking statements. All statements other than statements of historical fact are statements that could be forward-looking statements. You can identify these forward-looking statements through our use of words such as “may,” “can,” “anticipate,” “assume,” “should,” “indicate,” “would,” “believe,” “contemplate,” “expect,” “seek,” “estimate,” “continue,” “plan,” “point to,” “project,” “predict,” “could,” “intend,” “target,” “potential” and other similar words and expressions of the future.
There are a number of important factors that could cause the actual results to differ materially from those expressed in any forward-looking statement made by us. These factors include, but are not limited to:
| ● | our history of operating losses; |
| ● | our current and future capital requirements and our ability to satisfy our capital needs; |
| ● | our ability to complete required clinical trials of our product candidates and obtain approval from the FDA or other regulatory agents in different jurisdictions; |
| ● | our ability to internally develop new product candidates, intellectual property, and other product candidates we may acquire and/or license; | |
| ● | our ability to maintain or protect the validity of our patents and other intellectual property; | |
| ● | our ability to retain key executive members; | |
| ● | the potential impact of the COVID-19 pandemic on our operations, including on our clinical development plans and timelines; | |
| ● | interpretations of current laws and the passages of future laws; | |
| ● | acceptance of our business model by investors; | |
| ● | the accuracy of our estimates regarding expenses and capital requirements; and | |
| ● | our ability to adequately support growth. |
The foregoing does not represent an exhaustive list of matters that may be covered by the forward-looking statements contained herein or risk factors that we are faced with that may cause our actual results to differ from those anticipate in our forward-looking statements. Please see “Risk Factors” for additional risks which could adversely impact our business and financial performance.
All forward-looking statements are expressly qualified in their entirety by this cautionary notice. You are cautioned not to place undue reliance on any forward-looking statements, which speak only as of the date of this report or the date of the document incorporated by reference into this report. We have no obligation, and expressly disclaim any obligation, to update, revise or correct any of the forward-looking statements, whether as a result of new information, future events or otherwise. We have expressed our expectations, beliefs and projections in good faith and we believe they have a reasonable basis. However, we cannot assure you that our expectations, beliefs or projections will result or be achieved or accomplished.
| 3 |
| Item 1. | BUSINESS |
All references in this report to “Corbus,” the “Company,” “we,” “us,” or “our” mean Corbus Pharmaceuticals Holdings, Inc. and its subsidiaries unless we state otherwise, or the context otherwise indicates.
Overview
We are a Phase 3, clinical-stage pharmaceutical company focused on the development and commercialization of novel therapeutics that target the endocannabinoid system in the fields of autoimmunity, fibrosis, and cancer. We are developing a diverse pipeline of drug candidates across several distinct programs, including small molecules as well as biologics, while also evaluating potential external candidates complimentary to our existing programs.
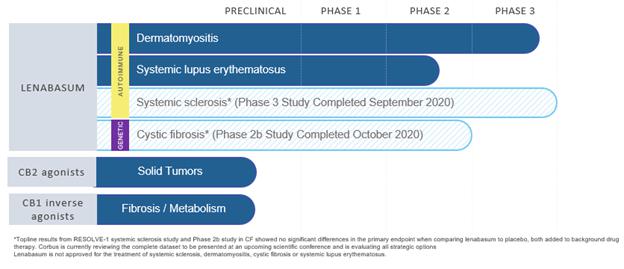
Our pipeline includes the following programs:
| 1. | Lenabasum, a novel, synthetic, oral, cannabinoid receptor type 2 (CB2) agonist designed to resolve chronic inflammation, limit fibrosis and support tissue repair. Lenabasum is in clinical development for treatment of autoimmune diseases. We are currently evaluating lenabasum for safety and efficacy in a Phase 3 study in dermatomyositis, as well as a Phase 2 study in systemic lupus erythematosus (“SLE”). | |
| 2. | Peripherally-restricted cannabinoid receptor type 1 (CB1) inverse agonists designed to normalize metabolic abnormalities or limit inflammation and fibrosis. We are currently evaluating these compounds in pre-clinical studies for the treatment of metabolic disorders and for fibrotic disorders. We are evaluating certain compounds as potential candidates for further clinical development. | |
| 3. | Novel CB2 agonists designed to limit cancer cell growth directly and reduce the fibrosis and immunosuppression in the tumor microenvironment that are associated with tumor growth, metastasis, and resistance to treatment with drugs such as checkpoint inhibitors. We are currently evaluating these compounds in pre-clinical studies for the treatment of cancer, in combination with other cancer therapies such as checkpoint inhibitors. We are evaluating certain compounds as potential candidates for further clinical development. |
Our Pipeline
Lenabasum for the Treatment of Autoimmune Diseases
Lenabasum selectively binds to CB2, which is preferentially expressed on activated immune cells, fibroblasts and other cell types, including muscle and bone cells. Lenabasum reduces inflammation and limits fibrosis, without immunosuppression. Lenabasum inhibits production of inflammatory cytokines and eicosanoids, and stimulates the production of mediators (Specialized Pro-resolving Lipid Mediators) that resolve inflammation. It inhibits transformation of fibroblasts into myofibroblasts and production of fibrotic growth factors and collagen. These biologic effects have been demonstrated in cells, animal models, and humans.
The U.S. Food and Drug Administration, or FDA, granted lenabasum Orphan Drug Designation as well as Fast Track Status for systemic sclerosis and cystic fibrosis, and Orphan Drug Designation for dermatomyositis. The European Medicines Authority, or EMA, has granted lenabasum Orphan Drug Designation for systemic sclerosis, cystic fibrosis, and dermatomyositis.
| 4 |
In 2020, we announced that lenabasum did not meet the primary endpoints in our RESOLVE-1 Phase 3 study of lenabasum for the treatment of systemic sclerosis (the “RESOLVE-1 Study”) or our Phase 2b study of lenabasum for the treatment of cystic fibrosis. Currently, no patients with systemic sclerosis or cystic fibrosis are being treated with lenabasum. We are preparing the data from our RESOLVE-1 Study for publication and will decide on the next steps in the development process for systemic sclerosis pending the outcome of our Phase 3 study of lenabasum for the treatment of dermatomyositis (the “DETERMINE Study”). We are preparing the data from our Phase 2b study of lenabasum for the treatment of cystic fibrosis for publication, but currently we do not have plans for additional clinical studies in cystic fibrosis.
In December 2018, we initiated the DETERMINE Study, our Phase 3 double-blind placebo-controlled multi-center international clinical study. The DETERMINE Study is fully enrolled with 176 patients. In January, 2021, we submitted a protocol amendment to the FDA to shorten the duration of the DETERMINE Study from 52 weeks to 28 weeks. Subjects in the DETERMINE Study are randomized to receive lenabasum 20 mg twice per day, lenabasum 5 mg twice per day, or placebo twice per day in a 2:1:2 ratio. The primary efficacy outcome, which will be measured at week 28, is the American College of Rheumatology/European League Against Rheumatism 2016 Total Improvement Score, which is a weighted composite measure of improvement from baseline in six endpoints, including Physician Global Assessment of Disease Activity, Physician Global Assessment of Extramuscular Disease Activity, Patient Global Assessment of Disease Activity, Health Assessment Questionnaire (patient-reported disability), Manual Muscle Testing, and muscle enzymes. Change from Baseline in the Cutaneous Dermatomyositis Activity and Severity Index activity (CDASI) score is one of several secondary efficacy outcomes in the Phase 3 study. All subjects in the DETERMINE study have completed their week 28 visit, and some need to complete a 28-day safety follow-up visit off study drug, with topline data expected in the second quarter of 2021.
The design of our DETERMINE Study was based on positive data from our 16-week, Phase 2 double-blind, placebo-controlled single center study of safety and efficacy of lenabasum in patients with refractory dermatomyositis skin disease and no more than minimal active muscle involvement at baseline. Our Phase 2 study was completed in October 2017 and showed improvement in skin disease with lenabasum treatment. All subjects remained on their background standard-of-care therapy, which, for a majority of patients, included immunosuppressive therapies, throughout the study. Lenabasum treatment was also associated with numerically better improvements in multiple secondary efficacy outcomes, compared to placebo. Lenabasum was safely administered in this study, with no severe or serious adverse effects. Lenabasum was well-tolerated, with no subjects discontinuing treatment because of an adverse effect related to lenabasum.
In our Phase 2 study of lenabasum for the treatment of dermatomyositis, the mean improvement (reduction) in the primary efficacy outcome, the CDASI score, was 9.3 points for lenabasum treatment versus a reduction of 3.7 points for placebo treatment (p = 0.04, 2-sided MMRM) at Week 16.
| 5 |
Phase 2 Dermatomyositis Study*
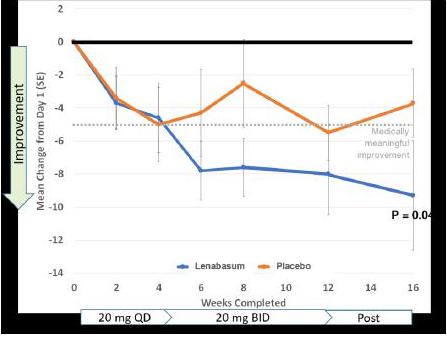
*Data on file.
Our double-blind, randomized, placebo-controlled Phase 2 study of lenabasum in systemic lupus erythematosus (funded by the National Institutes of Health) is underway. The study is expected to dose 100 subjects at 15 sites. Enrollment is expected to be completed in the second fiscal quarter of 2021, and topline results are expected in the second half of 2021.
Lenabasum has demonstrated acceptable safety and tolerability profiles in clinical studies to date.
CB1 Inverse Agonists for the Treatment of Metabolic and Fibrotic Diseases
CB1 is a receptor that is highly expressed in the nervous system and is also expressed in multiple cell lines outside the nervous system. A CB1 agonist is a compound that initiates a pharmacologic response when it binds to CB1. Both CB1 antagonists and CB1 inverse agonists bind to, or block, CB1 and will reduce pharmacologic effects of CB1 agonists. A CB1 inverse agonist binds CB1 but also induces a pharmacological response opposite to a CB1 agonist. Testing of CB1 antagonists and CB1 inverse agonists in animal studies has shown improvement in models of metabolic diseases, including diet-induced obesity, diabetes, diabetic nephropathy, diabetic retinopathy, metabolic syndrome, non-alcoholic steatohepatitis, fibrotic diseases including (lung, cardiac, renal disease, and liver fibrosis), and other diseases including ascites, cognitive defects, Prader-Willi syndrome, and smoking cessation.
| 6 |
In the nervous system, CB1 regulates neurotransmission. Despite the positive results observed in animal studies of CB1 antagonists and CB1 inverse agonists for the treatment of certain diseases, treatment with a particular CB1 inverse agonist, rimonabant (brand name, Acomplia), has also been associated with increased risk of anxiety, depression, and suicidality in humans that led in October 2008 to the withdrawal of rimonabant from the European market, where it had been approved for treatment of obesity.
Importantly, data shows that the metabolic effects of blocking CB1 are mediated by CB1 in the periphery, not the central nervous system. This has led to efforts to develop drugs that block CB1 only outside the central nervous system, to avoid adverse central nervous system effects seen with rimonabant when treating metabolic diseases. When considering treatment of metabolic diseases, CB1 is known to have reciprocal functional activities with the incretins glucose-dependent insulinotropic polypeptide, or GIP, and glucagon-like peptide-1, or GLP-1. This is of importance because recent data show that GIP/GLP-1 receptor agonists semaglutide and tirzepatide reduce obesity and blood sugar in humans. In animal studies, GIP/GLP-1 receptor agonists are reported to have greater metabolic effects when used in combination with CB1 inhibitors than when used as monotherapies. Beneficial effects of the combination of GIP/GLP-1 receptor agonists and CB1 inhibitors have been observed on body weight, fat mass, insulin action, dyslipidemia, and hepatic steatosis in obese diabetic mice.
We have an exclusive worldwide license to develop, manufacture and market drug candidates from more than 600 compounds that have been developed primarily to serve as CB1 inverse agonists with limited blood-brain-barrier penetration, to lessen risks of CB1-mediated central nervous system adverse effects.
We have identified and are conducting pre-clinical studies of several CB1 inverse agonists that have shown low exposure in the brain compared to the plasma. As shown below, the area under the curve exposure in the brain is less than 5-10% of that in the plasma for some of our compounds in murine studies.
Novel CB1 Inverse Agonists Have Low Plasma: Brain Ratios*
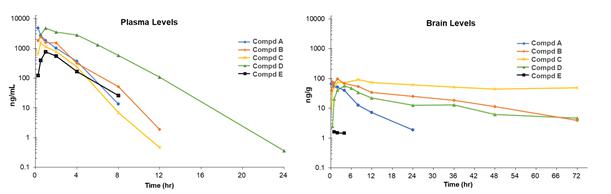
*Data on file.
| 7 |
Some of these compounds have shown metabolic effects in a diet-induced obesity (DIO) murine model, preventing weight gain, or inducing weight loss and improving glucose tolerance. In the experiment shown below, mice received a high fat diet for 16 weeks to induce obesity and glucose intolerance, then continued to receive high fat diet while receiving oral compounds for 4 weeks. Treatment with CRB cmpd C gave dose dependent decreases in body weight that were similar to the positive control rimonabant. At the same doses, but lower exposures, cmpd D appeared to prevent the body weight gains associated with vehicle, though the differences were not statistically significant. However, CRB cmpd D gave exposures that were ~7-12 fold lower than exposures for the same dose of CRB cmpd C, so results for CRB cmpds C and D should not be compared directly. CRB cmpd D (5 mg/kg and 10 mg/kg) significantly reduced blood glucose levels at 15 minutes and 30 minutes post glucose challenge indicating improvement in glucose tolerance. Note that 1 hour after the last study dose, the brain-plasma ratio for CRB cmpd C was 0.04 (5 mg/kg) and 0.02 (10 mg/kg) and for CRB cmpd D was 0.04 for both doses.
Novel CB1 Inverse Agonists Prevent Weight Gain or Induce Weight Loss in a Diet-Induced Obesity Model*
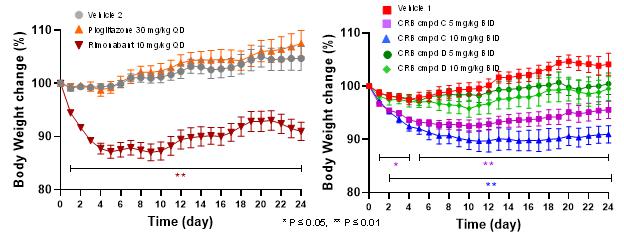
Diet-Induced Obesity Treatment Results: Mouse body weight change induced by study controls Pioglitazone and rimonabant compared to CRB Compounds (cmpd) C and D. Data are means of n = 10 animals per time point. Day 0 = start of investigational compound dosing.
* Data on file. Presented at New York Academy of Sciences Webinar on January 27, 2021.
Novel CB1 Inverse Agonists Improve Glucose Tolerance in a Diet-Induced Obesity Model*
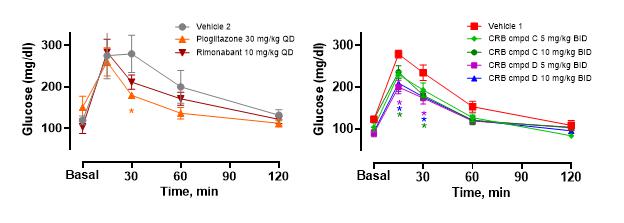
Glucose Tolerance Test: Oral glucose challenge was performed on Day 25. Data are means of n = 5/group. *p < 0.05.
* Data on file. Presented at New York Academy of Sciences Webinar on January 27, 2021.
Some of the CB1 inverse agonist compounds we are evaluating have demonstrated anti-inflammatory and anti-fibrotic effects, as well as the inhibition of inflammatory cytokine production and the fibroblast to myofibroblast transition in pre-clinical studies.
For some of the CB1 inverse agonists, we will further evaluate drug exposure and CB1 occupancy in the brain, relative to the periphery, following chronic dosing in several animal species including non-human primates. We have planned other pre-clinical studies to fully characterize effects of these compounds in animal models of metabolic diseases and fibrosis. We also plan to test metabolic effects of our CB1 inverse agonists in combination with GLP-1 receptor agonists in animal models.
We believe that CB1 inverse agonists with limited CB1 receptor occupancy in the brain may potentially be a safe and effective treatment for metabolic, fibrotic and other diseases. We intend to begin IND-enabling studies with a CB1 inverse agonist (yet to be selected) in 2021 and begin Phase 1 testing in 2022.
| 8 |
Novel CB2 agonists for treatment of cancer
The role of the endocannabinoid system in cancer has been widely researched and is a focus of current oncology research. Unregulated expression of cannabinoid receptors and the elevated levels of endocannabinoids have been observed in a variety of cancer cells (skin, prostate, and colon cancer, hepato- cellular carcinoma, endometrial sarcoma, glioblastoma multiforme, meningioma and pituitary adenoma, Hodgkin lymphoma, chemically induced hepatocarcinoma, mantel cell lymphoma). For example, CB2 expression in breast cancer biopsies correlates with negative clinical outcomes.
Pre-clinical studies of CB2 agonists in tumor models in vitro and in vivo have shown positive data, with a decrease in tumor growth and progression observed. Similarly, plant-derived cannabinoids such as tetrahydrocannabinol and cannabidiol have shown activity in pre-clinical models of cancer. Several pathways downstream from CB2 have been proposed to mediate possible anti-cancer activities of CB2 agonists, as shown in the figure below.
Proposed CB2 Pathways for Anti-Cancer Activities*
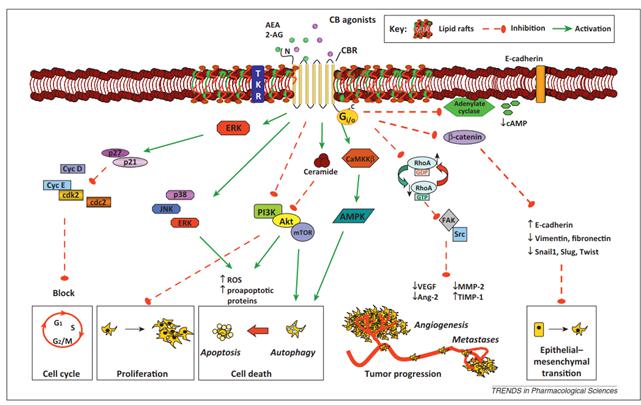
*Pisanti S, Picardi P, D'Alessandro A, Laezza C, Bifulco M. The endocannabinoid signaling system in cancer. Trends Pharmacol Sci. 2013 May;34(5):273-82. doi: 10.1016/j.tips.2013.03.003. Epub 2013 Apr 17. PMID: 23602129.
We have several novel CB2 agonists (which also function as CB1 agonists) that have reduced proliferation of some human tumor cell lines in vitro (some Her2+ breast cancer, estrogen receptor+ breast cancer, triple negative breast cancer, lymphoma, non-small cell lung cancer, and glioblastoma cell lines) in our pre-clinical studies. A time-dependent reduction in phosphorylation of Her2 on Her2+ HCC1954 breast cancer cells in vivo has been observed as shown in the first panel in the figure below. In this experiment, HCC1954 Her2+ breast cancer cells were cultured with vehicle (DMSO) or CRB cmpd DD for different times. Densitometric analysis of the relative expression of the phosphorylated Her2 vs. total Her2 protein was determined. CRB cmpd DD suppressed Her2 phosphorylation in vitro in HCC1954 cells.
| 9 |
We have conducted pre-clinical studies with our CB2 agonists that have shown a reduction in tumor volume of human Her2+ breast cancer cell HCC1954 (shown in the second panel in the figure below) and a triple negative breast cancer in xenograft murine models. In the experiment shown below, female Balb/c nude mice (n = 10/group) were injected in the flank with HCC1954 Her2+ breast cancer cells. Pharmacological treatments for 21 days with vehicle or CRB cmpd DD were started when tumors reached 90-180 mm3,with BKM-129 serving as a concurrent positive control. Tumor dimensions were measured using a caliper and used to calculate tumor volume.
A CB2 Agonist Inhibits Her2 Phosphorylation in vitro in a Cancer Cell Line and in vivo in a Her2+ Tumor Cell Growth in a Xenograft Model
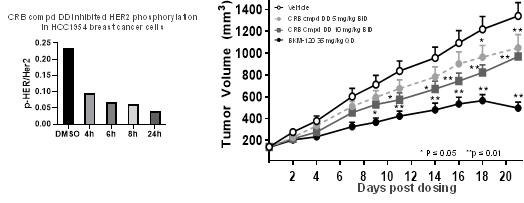
* Data on file. Presented at New York Academy of Sciences Webinar on January 27, 2021.
We are conducting and plan to commence additional pre-clinical studies to define the range of anti-cancer effects of our CB2 agonist compounds and the underlying pathways for these effects. We also plan to test efficacy of these compounds as monotherapy and in combination with other anti-cancer agents such as checkpoint inhibitors, in animal models. We believe that it will be important to demonstrate that these compounds add to the efficacy seen with checkpoint inhibitors alone in animal models before moving these compounds into clinical development. We intend to begin IND-enabling studies with a CB2 inverse agonist (yet to be selected) in 2021 and begin Phase 1 testing in 2022.
Lenabasum Market Opportunity and Developed Competitive Landscape
Dermatomyositis
Dermatomyositis is a serious and rare autoimmune idiopathic inflammatory myopathy with characteristic cutaneous findings. About 80,000 individuals in the U.S., Europe and Japan suffer from dermatomyositis. Dermatomyositis usually strikes adults, with common age of onset in adults between 50-60 years of age.
This systemic disorder most frequently affects the skin and muscles, and dermatomyositis can also include interstitial lung disease/restrictive lung disease, arthritis, gastrointestinal and cardiac involvement. Inflammatory muscle disease associated with dermatomyositis can cause discomfort and significant weakness of the proximal muscles of the arms and legs and of the trunk. Dermatomyositis can include damaging inflammation elsewhere in the body, for example: lung inflammation that leads to lung fibrosis and restrictive lung disease; heart inflammation that causes arrhythmia, congestive heart failure, and pericarditis; inflammation of muscles in the esophagus that causes swallowing problems or aspiration pneumonia; and arthritis. Dermatomyositis patients may have active skin disease despite successful treatment of their muscle and/or lung disease. The skin findings in dermatomyositis can be disfiguring and are inflammatory rashes characterized by redness and itching in exposed areas of the skin, around the eyes, on the hands, and in a “shawl” distribution on the scalp, hands, upper back, and photo-exposed areas. Patients with dermatomyositis have an increased risk of malignancy, most commonly in older patients. By itself, skin involvement in dermatomyositis has a large negative impact on quality of life, comparable to that of cutaneous lupus erythematosus, and much higher than many dermatologic diseases.
Typically, people with dermatomyositis are prescribed immunosuppressive therapies. These therapies may be associated with significant side effects, such as serious infections. FDA-approved treatments for dermatomyositis include systemic corticosteroids and adrenocorticotropic hormone analogue. Additionally, a Phase 3 study of Octagam® 10% in dermatomyositis (NCT02728752) was reported in 2020 to achieve its primary endpoint.
We believe that a safe and effective drug that controls inflammation in the skin, muscles, and other organs and improves overall disease would address a significant unmet medical need in dermatomyositis, particularly a non-immunosuppressive drug like lenabasum.
| 10 |
Systemic Lupus Erythematosus
Systemic lupus erythematosus (SLE) is a prototypical autoimmune disease with a wide array of clinical manifestations, including arthritis, rash, photosensitivity, oral ulcers, pleuritis, pericarditis, kidney problems, seizures and psychosis and blood cell abnormalities. About 550,000 individuals in the U.S., Europe and Japan suffer from SLE. The musculoskeletal system is the most commonly involved system in SLE. Patients with SLE have an increased frequency of related autoimmune problems, such as Sjogren’s syndrome and antiphospholipid syndrome that require additional treatments. Systemic lupus erythematosus may occur with other autoimmune conditions, such as thyroiditis, hemolytic anemia, and idiopathic thrombocytopenia purpura.
The pathology of SLE involves chronic activation of the innate immune system by immune complexes, with activation of the complement cascade, increased production of type 1 interferons and other mediators of inflammation, generation of specific immunity against self-antigens, and resultant tissue inflammation and damage.
Medicines specifically approved by the FDA for treatment of SLE are aspirin, hydroxychloroquine, corticosteroids (for example, prednisone), the corticotropin injection Acthar® and the immunosuppressive drug Benlysta®. Other drugs that are not specifically FDA approved for SLE may be prescribed by physicians, including methotrexate, mycophenolate, azathioprine, and cyclophosphamide. These treatments may be associated with significant side effects, such as serious infections.
We believe that a safe and effective drug that controls inflammation in the joints and skin as well as improves overall disease activity will address a significant unmet medical need in SLE, particularly a non-immunosuppressive drug like lenabasum.
Sales and Marketing for Lenabasum
We are developing our commercial capabilities in anticipation of potential FDA approval for lenabasum. Our intent is to commercialize lenabasum ourselves in the United States with a targeted customer-facing organization to call on treating specialists and payers. In Europe we are evaluating potential partnerships for the commercialization of lenabasum as well as considering the option of commercializing ourselves. In Japan we granted exclusive license rights to Kaken Pharmaceutical Co., Ltd., or Kaken, for the commercialization of lenabasum for the treatment of systemic sclerosis and dermatomyositis.
CB1 Inverse Agonist Market Opportunity
There has been clinical interest in CB1 inverse agonists and antagonists for their potential applications in fibrosis, and metabolic disorders such as obesity. In obesity, rimonabant (brand name Acomplia), a CB1 inverse agonist, received marketing authorization in Europe in 2006 prior to its subsequent withdrawal in 2008 due to safety concerns. In fibrosis, there are two companies with pre-clinical stage CB1 inverse agonist programs. Goldfinch Bio has a preclinical program in diabetic nephropathy. Inversago has preclinical programs in diabetic nephropathy, non-alcoholic steatohepatitis, and Prader-Willi syndrome.
We believe there is continued interest in the potential benefits of reducing obesity in diabetic and other at-risk populations. Recent data from two large clinical studies have demonstrated significant effects of GLP-1 agonists on weight loss in a diabetic population. As of 2019, the market size for GLP-1 agonists was estimated at over $10 billion and expected to grow based on a 2016 estimate of approximately 1.9 billion adults worldwide who are overweight and at increased risk of developing diabetes.We believe a CB1 inverse agonist that avoids the potential central nervous system adverse effects associated with Acomplia could have potential clinical utility in helping treat metabolic disorders.
| 11 |
Market Opportunity for CB2 Agonists That Add Benefit to Immune Checkpoint Inhibitors
The emergence of immune checkpoint inhibitors, or ICIs has transformed the treatment paradigm for multiple cancers. The ICI market reached $24 billion worldwide in 2019 and is projected to grow to more than $50 billion by 2026. However, as of 2019, it is estimated that as few as 44% of patients are eligible to receive and only 12.5% of all patients respond to an ICI. Even for patients who achieve a response, disease progression often occurs due to resistance mechanisms. Therefore, therapies that combine with checkpoint inhibitors to improve outcomes, for example by altering the tumor microenvironment to reduce immunosuppression or fibrosis, may offer an attractive commercial opportunity. We are currently planning to conduct pre-clinical studies of certain of our CB2 agonist compounds with ICIs for the treatment of certain cancer indications.
Intellectual Property
We have filed patent applications directed to lenabasum, compositions and methods for treating disease using lenabasum. If granted, the resulting patents would expire on dates ranging from 2031 to 2034, subject to extension under certain circumstances. The patent application filings are directed to:
| ● | Compositions including an improved ultrapure version of lenabasum and uses of the compositions for the treatment of fibrotic conditions and inflammatory conditions; | |
| ● | The use of lenabasum in the treatment of fibrotic diseases; and | |
| ● | Lenabasum formulations and uses of the formulations for the treatment of disease. |
Issued Patents
On August 6, 2019, the U.S. Patent and Trademark Office (“USPTO”) issued U.S. Patent No. 10,369,131 to the Company with claims covering the use of pharmaceutical compositions comprising lenabasum for the treatment of dermatomyositis. The patent provides exclusivity in the U.S. for this use of lenabasum to February 12, 2034.
| 12 |
On December 18, 2018, USPTO issued U.S. Patent No. 10,154,986 to the Company with claims covering pharmaceutical compositions of lenabasum. The patent provides exclusivity in the U.S. for these lenabasum compositions to February 12, 2034.
On October 3, 2018, the USPTO issued U.S. Patent No. 10,085,964 to the Company with claims covering the use of pharmaceutical compositions comprising lenabasum for the treatment of all fibrotic diseases, encompassing Corbus’ lead indications systemic sclerosis, cystic fibrosis and others. The patent provides exclusivity in the U.S. for this use of lenabasum to February 12, 2034.
On October 31, 2017, the USPTO issued U.S. Patent No. 9,801,849 to the Company with claims covering the use of pharmaceutical compositions comprising lenabasum, for the treatment of all inflammatory diseases. The patent provides exclusivity in the U.S. for this use of lenabasum to February 12, 2034.
On November 27, 2017, the USPTO issued U.S. Patent No. 9,820,964 to the Company with claims covering the use of pharmaceutical compositions comprising lenabasum for the treatment of all fibrotic diseases, encompassing the Company’s lead indications systemic sclerosis, cystic fibrosis and others. The patent provides intellectual property protection in the United States for this use of lenabasum to February 12, 2034.
On September 20, 2018, we entered into an exclusive license agreement with Jenrin Discovery, LLC which provides us with an exclusive worldwide license to develop and market cannabinoid compounds covered by the Jenrin issued patents and patent applications that cover the composition and method of use of selective cannabinoid receptor modulators. The Jenrin intellectual property portfolio includes sixteen granted United States patents, one pending United States application and twenty-two granted or pending foreign patents and applications. This portfolio includes U.S. Patent No. 8,680,131, which granted with claims covering the cannabinoid receptor blocker CRB-4001 and methods of using the same for treating obesity related disorders, diabetes, various inflammatory disorders, various cardiometabolic disorders, various hepatic disorders, and/or various cancers. The licensed intellectual property portfolio provides intellectual property protection in the United States for CRB-4001 and these uses to July of 2033, not including any potential patent term extension.
Lenabasum has been granted Orphan Drug Designation for cystic fibrosis, dermatomyositis and systemic sclerosis in the U.S. and in the European Union and for systemic sclerosis in Japan. In addition, in systemic sclerosis and in cystic fibrosis, lenabasum has been granted a Fast Track Designation by the FDA. Orphan designation for lenabasum may be pursued for other inflammatory diseases in the U.S., Europe, and Japan. Orphan drug status provides seven years of market exclusivity in the U.S. and ten years in Europe and Japan beginning on the date of drug approval.
Our commercial success depends in part on our ability to obtain and maintain patent and other proprietary protection for lenabasum and to operate without infringing the proprietary right of others and to prevent others from infringing our proprietary rights. We strive to protect our intellectual property through a combination of patents and trademarks as well as through the confidentiality provisions in our contracts. With respect to lenabasum, we endeavor to obtain and maintain patent protection in the U.S. and internationally on all patentable aspects of the drug. We cannot be sure that the patents will be granted with respect to any patent applications we may own or license in the future, nor can we be sure that any patents issued or licensed to us in the future will be useful in protecting our technology. For this and more comprehensive risks related to our intellectual property, please see “Risk Factors—Risks Relating to Our Intellectual Property Rights.”
In addition to patent protection, we rely on trade secrets and know-how to develop and maintain our competitive position. For example, aspects of our proprietary technology platform are based on unpatented trade secrets and know-how related to the manufacturing of lenabasum. Trade secrets and know-how can be difficult to protect. We seek to protect our proprietary technology and processes, in part, by confidentiality agreements and invention assignment agreements with our employees, consultants, scientific advisors, contractors and commercial partners. These agreements are designed to protect our proprietary information and, in the case of the invention assignment agreements, to grant us ownership of technologies that are developed through a relationship with a third party. We also seek to preserve the integrity and confidentiality of our data and trade secrets by maintaining physical security of our premises and physical and electronic security of our information technology systems. While we have confidence in these individuals, organizations and systems, agreements or security measures may be breached, and we may not have adequate remedies for any breach. In addition, our trade secrets may otherwise become known or be independently discovered by competitors. To the extent that our contractors use intellectual property owned by others in their work for us, disputes may arise as to the rights in related or resulting know-how and inventions.
| 13 |
We also seek and will continue to seek trademark protection in the United States and outside of the United States where available and when appropriate. We use and intend to use these registered marks in connection with our pharmaceutical research and development as well as our product candidates.
Manufacturing and Supply for Lenabasum and Our Other Product Candidates
Lenabasum is a synthetic molecule and there are readily available supplies of all raw materials necessary for manufacturing lenabasum. We have developed and validated a good manufacturing practice, or GMP, to manufacture lenabasum’s active pharmaceutical ingredient and drug product through our contract manufacturers. Our existing active pharmaceutical ingredient contract manufacturer has produced multi-kilogram scale bulk batches under GMP for our on-going clinical studies and is under agreement to produce sufficient API required prior to submitting an NDA filing with the FDA. We do not own or operate manufacturing facilities for the production of lenabasum. We expect to depend on third-party suppliers and manufacturing organizations for all our pre-clinical and clinical trial quantities of raw materials and drug substance.
Regulatory Matters
Government Regulation
The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local and foreign statutes and regulations require the expenditure of substantial time and financial resources. Failure to comply with the applicable requirements at any time during the product development process, approval process or after approval, may subject an applicant to administrative or judicial sanctions. These sanctions could include the FDA’s refusal to approve pending applications, withdrawal of an approval, a clinical hold, warning letters, product recalls or withdrawals from the market, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement, or civil or criminal penalties. Any agency or judicial enforcement action could have a material adverse effect on us.
Any product development activities related to lenabasum or products that we may develop or acquire in the future will be subject to extensive regulation by various government authorities, including the FDA, other federal, state and local agencies and comparable regulatory authorities in other countries, which regulate the design, research, clinical and non-clinical development, testing, manufacturing, storage, distribution, import, export, labeling, advertising and marketing of pharmaceutical products and devices. Generally, before a new drug can be sold, considerable data demonstrating its quality, safety and efficacy must be obtained, organized into a format specific to each regulatory authority, submitted for review and approved by the regulatory authority. The data are often generated in two distinct development states: pre-clinical and clinical.
Development of Drugs in the United States
Lenabasum or other products that we may develop or acquire in the future must be approved by the FDA before they may be legally marketed in the United States. For new chemical entities, the pre-clinical development stage generally involves synthesizing the active component, developing the formulation and determining the manufacturing process, and drug stability as well as carrying out non-human toxicology, pharmacology and drug metabolism studies that support subsequent clinical testing. These pre-clinical laboratory and animal tests are often performed under the FDA’s Good Laboratory Practices regulations. A drug’s sponsor must submit the result of the pre-clinical tests, together with manufacturing information, analytical data and any available clinical data or literature and a proposed clinical protocol to the FDA as part of an IND application, which is a request for authorization from the FDA to administer an investigational drug or biological product to humans. Similar filings are required in other countries.
| 14 |
The clinical stage of development can generally be divided into three sequential phases that may overlap, Phase 1, Phase 2 and Phase 3 clinical trials. In Phase 1, generally, small numbers of healthy volunteers are initially exposed to single escalating doses and then multiple escalating doses of the product candidate. The primary purpose of these studies is to assess the metabolism, pharmacologic action and general safety of the drug. Phase 2 trials typically involve studies in disease-affected patients to determine the dose required to produce the desired benefits, common short-term side effects and risks. Phase 2 studies are typically well-controlled, closely monitored, and conducted in a relatively small number of patients, usually involving no more than several hundred subjects. Phase 3 trials are intended to gather the additional information about effectiveness and safety that is needed to evaluate the overall benefit-risk relationship of the drug and to provide an adequate basis for physician labeling. Phase 3 studies usually include from several hundred to several thousand subjects and are closely controlled and monitored. In addition to these Phase 1-3 trials, other trials may be conducted to gather additional safety, pharmacokinetic and pharmacodynamic information., Pharmaceutical products with active ingredients equal or similar to those already approved by the FDA often have more streamlined development programs than compounds entirely new to the agency, often skipping Phase 1 and 2 trials.
A clinical plan must be submitted to the FDA prior to commencement of a clinical trial. If the FDA has concerns about the clinical plan or the safety of the proposed studies, they may suspend or terminate the study at any time. Studies must be conducted in accordance with good clinical practice and reporting of study progress and any adverse experiences is required. Studies are also subject to review by independent institutional review boards responsible for overseeing studies at particular sites and protecting human research study subjects. An independent institutional review board may also suspend or terminate a study once initiated. Accordingly, we cannot be sure that submission of an IND will result in the FDA allowing clinical trials to begin, or that once begun, issues will not arise that could cause the trial to be suspended or terminated.
Post-approval studies, sometimes referred to as Phase 4 clinical trials, may be conducted after initial marketing approval. Sometimes, these studies are used to gain additional experience from the treatment of patients in the intended therapeutic condition. In certain instances, the FDA may mandate the performance of Phase 4 studies. In other situations, post-approval studies aim to gain additional indications for a medication.
Special Protocol Assessment
The Federal Food, Drug, and Cosmetic Act directs the FDA to meet with sponsors, pursuant to a sponsor’s written request, for the purpose of reaching agreement on the design and size of clinical trials intended to form the primary basis of an efficacy claim in an NDA. If an agreement is reached, the FDA will reduce the agreement to writing and make it part of the administrative record. This agreement is called a special protocol assessment, or SPA. While the FDA’s guidance on SPAs states that documented SPAs should be considered binding on the review division, the FDA has latitude to change its assessment if certain exceptions apply. Exceptions include public health concerns emerging that were unrecognized at the time of the protocol assessment, identification of a substantial scientific issue essential to the safety or efficacy testing that later comes to light, a sponsor’s failure to follow the protocol agreed upon, or the FDA’s reliance on data, assumptions or information that are determined to be wrong.
Review and Approval in the United States
Following pivotal or Phase 3 trial completion, data are analyzed to determine safety and efficacy. Data are then filed with the FDA in a New Drug Application, or an NDA, along with proposed labeling for the product and information about the manufacturing and testing processes and facilities that will be used to ensure product quality. In the United States, FDA approval of an NDA must be obtained before marketing a pharmaceutical product. The NDA must contain proof of safety, purity, potency and efficacy, which entails extensive pre-clinical and clinical testing.
The FDA will likely re-analyze the clinical trial data, which could result in extensive discussions between the FDA and us during the review process. The review and evaluation of applications by the FDA is extensive and time consuming and may take several years to complete. The FDA may conduct a pre-approval inspection of the manufacturing facilities for the new product to determine whether they comply with current good manufacturing practice requirements and may also audit data from clinical and pre-clinical trials.
| 15 |
There is no assurance that the FDA will act favorably or quickly in making such reviews and significant difficulties or costs may be encountered in our efforts to obtain FDA approvals. The FDA may require that certain contraindications, warnings or precautions be included in the product labeling, or may condition the approval of the NDA on other changes to the proposed labeling, development of adequate controls and specifications, or a commitment to conduct post-marketing testing or clinical trials and surveillance programs to monitor the safety of approved products that have been commercialized. Further, the FDA may place conditions on approvals including the requirement for a risk evaluation and mitigation strategy, or REMS, to assure the safe use of the drug. If the FDA concludes a REMS is needed, the sponsor of the NDA must submit a proposed REMS; the FDA will not approve the NDA without an approved REMS, if required. A REMS could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. Any of these limitations on approval or marketing could restrict the commercial promotion, distribution, prescription or dispensing of products. Product approvals may be withdrawn for non-compliance with regulatory standards or if problems occur.
Orphan Drug Designation
Under the Orphan Drug Act, the FDA may grant orphan drug designation to a drug intended to treat a rare disease or condition, which is generally a disease or condition that affects fewer than 200,000 individuals in the United States. Orphan product designation must be requested before submitting an NDA. After the FDA grants orphan drug designation, the identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. Orphan product designation does not convey any advantage in or shorten the duration of regulatory review and approval process. In addition to the potential period of exclusivity, orphan designation makes a company eligible for grant funding of up to $400,000 per year for four years to defray costs of clinical trial expenses, tax credits for clinical research expenses and potential exemption from the FDA application user fee.
If a product that has orphan designation subsequently receives the first FDA approval for the disease or condition for which it has such designation, the product is entitled to orphan drug exclusivity, which means the FDA may not approve any other applications to market the same drug for the same indication for seven years, except in limited circumstances, such as (i) the drug’s orphan designation is revoked; (ii) its marketing approval is withdrawn; (iii) the orphan exclusivity holder consents to the approval of another applicant’s product; (iv) the orphan exclusivity holder is unable to assure the availability of a sufficient quantity of drug; or (v) a showing of clinical superiority to the product with orphan exclusivity by a competitor product. If a drug designated as an orphan product receives marketing approval for an indication broader than what is designated, it may not be entitled to orphan drug exclusivity. We have received orphan drug designation for lenabasum for cystic fibrosis and systemic sclerosis. There can be no assurance that we will receive orphan drug designation for lenabasum for DM, or additional orphan diseases.
Drug Development in Europe
In the European Union, our future products may also be subject to extensive regulatory requirements. Similar to the U.S., the marketing of medicinal products is subject to the granting of marketing authorizations by regulatory agencies. Also, as in the U.S., the various phases of pre-clinical and clinical research in the European Union are subject to significant regulatory controls.
Review and Approval in the European Union
In the European Union, approval of new medicinal products can be obtained through one of three processes: the mutual recognition procedure, the centralized procedure and the decentralized procedure. We intend to determine which process we will follow, if any, in the future.
Mutual Recognition Procedure: An applicant submits an application in one European Union member state, known as the reference member state. Once the reference member state has granted the marketing authorization, the applicant may choose to submit applications in other concerned member states, requesting them to mutually recognize the marketing authorizations already granted. Under this mutual recognition process, authorities in other concerned member states have 55 days to raise objections, which must then be resolved by discussion among the concerned member states, the reference member state and the applicant within 90 days of the commencement of the mutual recognition procedure. If any disagreement remains, all considerations by authorities in the concerned member states are suspended and the disagreement is resolved through an arbitration process. The mutual recognition procedure results in separate national marketing authorizations in the reference member state.
| 16 |
Centralized Procedure: This procedure is currently mandatory for products developed by means of a biotechnological process and optional for new active substances and other “innovative medicinal products with novel characteristics.” Under this procedure, an application is submitted to the European Agency for the Evaluation of Medical Products. Two European Union member states are appointed to conduct an initial evaluation of each application. These countries each prepare an assessment report that is then used as the basis of a scientific opinion of the Committee on Proprietary Medical Products. If this opinion is favorable, it is sent to the European Commission, which drafts a decision. After consulting with the member states, the European Commission adopts a decision and grants a marketing authorization, which is valid throughout the European Union and confers the same rights and obligations in each of the member states as a marketing authorization granted by that member state.
Decentralized Procedure: The most recently introduced of the three processes for obtaining approval of new medicinal processes in the European Union, the decentralized procedure is similar to the mutual recognition procedure described above, but with differences in the timing that key documents are provided to concerned member states by the reference member state, the overall timing of the procedure and the possibility of, among other things, “clock stops” during the procedure.
Post-Marketing Requirements
Following approval of a new product, a pharmaceutical company and the approved product are subject to continuing regulation by the FDA and other federal and state regulatory authorities, including, among other things, monitoring and recordkeeping activities, reporting to applicable regulatory authorities of adverse experiences with the product, providing the regulatory authorities with updated safety and efficacy information, product sampling and distribution requirements, and complying with promotion and advertising requirements, which include, among others, standards for direct-to-consumer advertising, restrictions on promoting drugs for uses or in patient populations not described in the drug’s approved labeling (known as “off-label use”), and limitations on industry-sponsored scientific and educational activities. Although physicians may prescribe legally available drugs for off-label uses, manufacturers may not market or promote such off-label uses. Modifications or enhancements to the products or labeling or changes of site of manufacture are often subject to the approval of the FDA and other regulators, which may or may not be received or may result in a lengthy review process. The FDA regulations require the products be manufactured in specific approved facilities and in accordance with current good manufacturing practices, and NDA holders must list their products and register their manufacturing establishments with the FDA. These regulations also impose certain organizational, procedural and documentation requirements with respect to manufacturing and quality assurance activities. Drug manufacturers and other entities involved in the manufacture and distribution of approved drugs are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with current good manufacturing practice and other laws. NDA holders using contract manufacturers, laboratories or packagers are responsible for the selection and monitoring of qualified firms. These firms are subject to inspections by the FDA at any time, and the discovery of violative conditions could result in enforcement actions that interrupt the operation of any such facilities or the ability to distribute products manufactured, processed or tested by them.
Other Regulatory Matters
Manufacturing, sales, promotion and other activities following product approval are also subject to regulation by numerous regulatory authorities in addition to the FDA, including, in the United States, the Centers for Medicare & Medicaid Services, or CMS, other divisions of the Department of Health and Human Services, the Drug Enforcement Administration, the Consumer Product Safety Commission, the Federal Trade Commission, the Occupational Safety & Health Administration, the Environmental Protection Agency, and state and local governments. These regulations include:
● the federal healthcare program anti-kickback law which prohibits, among other things, persons from soliciting, receiving or providing remuneration, directly or indirectly, to induce either the referral of an individual, for an item or service or the purchasing or ordering of a good or service, for which payment may be made under federal healthcare programs such as the Medicare and Medicaid programs;
| 17 |
● federal false claims laws which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid, or other government reimbursement programs that are false or fraudulent. The government may assert that a claim including items or services resulting from a violation of the federal healthcare program anti-kickback law or related to off-label promotion constitutes a false or fraudulent claim for purposes of the federal false claims laws;
● the Federal Physician Payments Sunshine Act within the ACA, and its implementing regulations, require that certain manufacturers of drugs, devices, biological and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program (with certain exceptions) to report information related to certain payments or other transfers of value made or distributed to physicians and teaching hospitals, or to entities or individuals at the request of, or designated on behalf of, the physicians and teaching hospitals and to report annually certain ownership and investment interests held by physicians and their immediate family members; and
● the Health Insurance Portability and Accountability Act, or HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, or HITECH, and its implementing regulations, imposes certain requirements relating to the privacy, security and transmission of individually identifiable health information. Among other things, HITECH makes HIPAA’s privacy and security standards directly applicable to “business associates”—independent contractors or agents of covered entities that receive or obtain protected health information in connection with providing a service on behalf of a covered entity. HITECH also created four new tiers of civil monetary penalties, amended HIPAA to make civil and criminal penalties directly applicable to business associates and possibly other persons, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorneys’ fees and costs associated with pursuing federal civil actions.
● applicable child-resistant packaging requirements under the U.S. Poison Prevention Packaging Act.
● The Lanham Act and federal antitrust laws.
● state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws, which may apply to items or services reimbursed by any third-party payer, including commercial insurers, and state laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and often are not preempted by federal laws, thus complicating compliance efforts.
Distribution of pharmaceutical products is subject to additional requirements and regulations, including extensive record-keeping, licensing, traceability, and storage and security requirements intended to prevent the unauthorized sale of pharmaceutical products
The handling of any controlled substances must comply with the U.S. Controlled Substances Act and the Controlled Substances Import and Export Act. In the U.S., our product candidate, lenabasum, is currently classified as Schedule I controlled substance as defined in the Controlled Substance Act (“CSA”).
Schedule I controlled substances are pharmaceutical products subject to specific regulations under the CSA, that establishes, among other things, certain registration, manufacturing quotas, security, recordkeeping, reporting, import, export and other requirements administered by the DEA. All parties responsible for the manufacturing, distribution and testing the drug in clinical studies must apply for and obtain a license from the DEA before they are permitted to perform these activities with lenabasum. Furthermore, these parties must have the security, control, recordkeeping, reporting and inventory mechanisms required by the DEA to prevent drug loss and diversion. All licensed facilities are required to renew their registrations annually if they intend to continue to work with our drug. The DEA conducts periodic inspections of certain registered establishments that handle controlled substances. We have been working with our manufacturers, distributors, exporters and clinical sites to obtain the necessary licenses to work with lenabasum. The parties responsible for the manufacturing, distribution and export of lenabasum have already applied for and have been granted DEA licenses and a number of institutions responsible for conducting our current clinical studies have also been granted DEA licenses.
| 18 |
Individual states have also established controlled substance laws and regulations. Though state-controlled substances laws often mirror federal law because the states are separate jurisdictions, they may separately schedule drugs, as well. While some states automatically schedule a drug based on federal action, other states schedule drugs through rulemaking or a legislative action. The requirement for state registrations could also result in delay of the manufacturing, distribution of lenabasum or in the completion of our current clinical studies. We and our manufacturing vendors and clinical sites must also obtain separate state registrations, permits or licenses in order to be able to obtain, handle, and distribute controlled substances for clinical trials or commercial sale, and failure to meet applicable regulatory requirements could lead to enforcement and sanctions by the states in addition to those from the DEA or otherwise arising under federal law.
Third-Party Payer Coverage and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of any of our drug candidates that ultimately may obtain regulatory approval. In both the United States and foreign markets, our ability to commercialize our product candidates successfully, and to attract commercialization partners for our product candidates, depends in significant part on the availability of adequate financial coverage and reimbursement from third-party payers, including, in the United States, governmental payers such as the Medicare and Medicaid programs, managed care organizations, and private health insurers. Medicare is a federally funded program managed by the CMS, through local fiscal intermediaries and carriers that administer coverage and reimbursement for certain healthcare items and services furnished to the elderly and disabled. Medicaid is an insurance program for certain categories of patients whose income and assets fall below state defined levels and who are otherwise uninsured that is both federally and state funded and managed by each state. The federal government sets general guidelines for Medicaid and each state creates specific regulations that govern its individual program. Each payer has its own process and standards for determining whether it will cover and reimburse a procedure or particular product. Private payers often rely on the lead of the governmental payers in rendering coverage and reimbursement determinations. Therefore, achieving favorable CMS coverage and reimbursement is usually a significant gating issue for successful introduction of a new product. The competitive position of some of our products will depend, in part, upon the extent of coverage and adequate reimbursement for such products and for the procedures in which such products are used. Prices at which we or our customers seek reimbursement for our product candidates can be subject to challenge, reduction or denial by the government and other payers.
The United States Congress and state legislatures may, from time to time, propose and adopt initiatives aimed at cost containment, which could impact our ability to sell our product candidates profitably. For example, the two-year spending law signed by the President of United States on February 9, 2018 includes a provision raising the manufacturer discount to 70% in 2019 in the Medicare Part D coverage gap, also known as the “donut hole.” Under prior law, manufacturers were required to provide a 50% discount on prescription drugs purchased in the donut hole. Manufacturers of branded drugs will face much higher liabilities from donut hole payments beginning in 2019, estimated at multiple billions of dollars for some of the largest companies.
The cost of pharmaceuticals continues to generate substantial governmental and third-party payer interest. We expect that the pharmaceutical industry will experience pricing pressures due to the trend toward managed healthcare, the increasing influence of managed care organizations and additional legislative proposals. Our results of operations could be adversely affected by current and future healthcare reforms.
Some third-party payers also require pre-approval of coverage for new or innovative devices or drug therapies before they will reimburse healthcare providers that use such therapies. While we cannot predict whether any proposed cost-containment measures will be adopted or otherwise implemented in the future, the announcement or adoption of these proposals could have a material adverse effect on our ability to obtain adequate prices for our product candidates and operate profitably.
| 19 |
In addition, in some foreign countries, the proposed pricing for a drug must be approved before it may be lawfully marketed. The requirements governing drug pricing vary widely from country to country. For example, the European Union provides options for its member states to restrict the range of medicinal products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. A member state may approve a specific price for the medicinal product or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the medicinal product on the market. There can be no assurance that any country that has price controls or reimbursement limitations for pharmaceutical products will allow favorable reimbursement and pricing arrangements for any of our products. Historically, products launched in the European Union do not follow price structures of the United States and generally tend to be significantly lower.
Employees
We had 76 full-time employees at December 31, 2020. All our employees are engaged in administration, finance, clinical, manufacturing, regulatory and business development functions. We believe our relations with our employees are good. In addition, we utilize and will continue to utilize consultants, clinical research organizations and third parties to perform our pre-clinical studies, clinical studies, manufacturing and regulatory functions.
Corporate Information
Corbus Pharmaceuticals, Inc. (formerly known as JB Therapeutics Inc.), was incorporated on April 24, 2009 under the laws of the State of Delaware. On April 11, 2014, JB Therapeutics, Inc. completed a merger with Corbus Pharmaceuticals Holdings, Inc. and changed its name to Corbus Pharmaceuticals, Inc. Upon the consummation of the merger, Corbus Pharmaceuticals, Inc. became a wholly-owned subsidiary of Corbus Pharmaceuticals Holdings, Inc. which continues to operate the business of Corbus Pharmaceuticals, Inc. Our principal executive offices are located at 500 River Ridge Drive, Norwood, Massachusetts 02062, and our telephone number is (617) 963-0100. Our website address is www.corbuspharma.com.
We make available free of charge on or through the Investor Relations link on our website, www.corbuspharma.com, access to press releases and investor presentations, as well as all materials that we file electronically with the SEC, including our annual report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports, filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act as soon as reasonably practicable after electronically filing such materials with, or furnishing them to, the SEC. During the period covered by this Form 10-K, we made all such materials available through our website as soon as reasonably practicable after filing such materials with the SEC. In addition, the SEC maintains an Internet website, www.sec.gov, that contains reports, proxy and information statements and other information that we file electronically with the SEC.
This report and the information incorporated herein by reference contain references to trademarks, service marks and trade names owned by us or other companies. Solely for convenience, trademarks, service marks and trade names referred to in this report and the information incorporated herein, including logos, artwork, and other visual displays, may appear without the ® or ™ symbols, but such references are not intended to indicate, in any way, that we will not assert, to the fullest extent under applicable law, our rights or the rights of the applicable licensor to these trademarks, service marks and trade names. We do not intend our use or display of other companies’ trade names, service marks or trademarks to imply a relationship with, or endorsement or sponsorship of us by, any other companies. Other trademarks, trade names and service marks appearing in this report are the property of their respective owners.
| 20 |
| ITEM 1A. | RISK FACTORS |
An investment in our common stock is speculative and illiquid and involves a high degree of risk including the risk of a loss of your entire investment. You should carefully consider the risks and uncertainties described below and the other information contained in this report and our other reports filed with the Securities and Exchange Commission. The risks set forth below are not the only ones facing us. Additional risks and uncertainties may exist that could also adversely affect our business, operations and financial condition. If any of the following risks actually materialize, our business, financial condition and/or operations could suffer. In such event, the value of our common stock could decline, and you could lose all or a substantial portion of the money that you pay for our common stock.
Risk Related to our Company and our Business
Risks Related to Our Financial Position and Need for Capital
We are a clinical stage pharmaceutical company with a limited operating history.
We are a clinical stage pharmaceutical company with a limited operating history. We must complete clinical studies and other development activity and receive regulatory approval of a New Drug Application, or NDA, before commercial sales of a product can commence. The likelihood of success of our business plan must be considered in light of the problems, substantial expenses, difficulties, complications and delays frequently encountered in connection with developing and expanding early-stage businesses and the regulatory and competitive environment in which we operate. Pharmaceutical product development is a highly speculative undertaking, involves a substantial degree of risk and is a capital-intensive business.
Accordingly, you should consider our prospects in light of the costs, uncertainties, delays and difficulties frequently encountered by companies in the early stages of development, especially clinical pharmaceutical companies such as ours. Potential investors should carefully consider the risks and uncertainties that a company with a limited operating history will face. In particular, potential investors should consider that we cannot assure you that we will be able to:
| ● | successfully implement or execute our current business plan, and we cannot assure you that our business plan is sound; | |
| ● | successfully manufacture our clinical products and establish commercial drug supply; | |
| ● | obtain Drug Enforcement Administration, or DEA, licenses necessary for the manufacturing of lenabasum and for evaluating lenabasum in our clinical trials; | |
| ● | successfully complete the preclinical and clinical trials necessary to obtain regulatory approval for the marketing of our drug candidates, including lenabasum and our cannabinoid drug candidates; | |
| ● | secure market exclusivity and/or adequate intellectual property protection for our drug candidates; | |
| ● | attract and retain an experienced management and advisory team; | |
| ● | secure acceptance of our drug candidates in the medical community and with third party payors and consumers; | |
| ● | launch commercial sales of our drug candidates, whether alone or in collaboration with others; and | |
| ● | raise sufficient funds in the capital markets to effectuate our business plan. |
If we cannot successfully execute any one of the foregoing, our business may not succeed and your investment will be adversely affected.
| 21 |
We have incurred operating losses in each year since our inception and expect to continue to incur substantial losses for the foreseeable future. We may never become profitable or, if we achieve profitability, be able to sustain profitability.
We expect to incur substantial expenses without corresponding revenues unless and until we are able to obtain regulatory approval and successfully commercialize any of our drug candidates. To date, we have not generated any revenue from our drug candidates and we expect to incur significant expense to complete our preclinical and clinical program for our drug candidates in the United States and elsewhere. We may never be able to obtain regulatory approval for the marketing of our drug candidates in any indication in the United States or internationally. Even if we are able to commercialize our drug candidates, there can be no assurance that we will generate significant revenues or ever achieve profitability. Our net losses for the years ended December 31, 2020 and December 31, 2019 were approximately $111,269,000 and $71,454,000, respectively. As of December 31, 2020, we had an accumulated deficit of approximately $304.1 million.
We may elect to pursue FDA approval for lenabasum in other indications and for other drug candidates, which will result in significant additional research and development expenses. As a result, we expect to continue to incur substantial losses for the foreseeable future, and these losses will increase. We are uncertain when or if we will be able to achieve or sustain profitability. If we achieve profitability in the future, we may not be able to sustain profitability in subsequent periods. Failure to become and remain profitable would impair our ability to sustain operations and adversely affect the price of our common stock and our ability to raise capital.
Our cash or cash equivalents will only fund our operations for a limited time and we will need to raise additional capital to support our development and commercialization efforts.
We are currently operating at a loss and expect our operating costs will increase significantly as we incur further costs related to preclinical development and the clinical trials for our drug candidates. As of December 31, 2020, we held cash and cash equivalents of approximately $85.4 million.
On January 26, 2018, we entered into the Cystic Fibrosis Program Related Investment Agreement (the “Investment Agreement”) with the Cystic Fibrosis Foundation, a non-profit drug discovery and development corporation, pursuant to which we received a development award for up to $25 million in funding (the “2018 CFF Award”) to support a Phase 2b clinical trial (the “Phase 2b Clinical Trial”) of lenabasum in patients with cystic fibrosis, of which we received $22.5 million to date. The remainder of the 2018 CFF Award is payable to us incrementally upon the achievement of the remaining milestones related to the progress of the Phase 2b Clinical Trial, as set forth in the Investment Agreement and we expect to receive the remainder before the end of the first half of 2021.
On January 3, 2019, we entered into a strategic collaboration with Kaken Pharmaceutical Co., Ltd. (“Kaken”) for the development and commercialization in Japan of lenabasum for the treatment of SSc and DM. Under the terms of the agreement, Kaken receives an exclusive license to commercialize and market lenabasum in Japan for SSc and DM. Kaken made an upfront payment to us of $27 million. We are eligible to receive in addition up to $173 million upon achievement of certain regulatory, development and sales milestones as well as double-digit royalties.
On July 28, 2020, we entered into a Loan and Security Agreement (the “Loan Agreement”) with our subsidiary, Corbus Pharmaceuticals, Inc., as borrower, us, as guarantor, each lender party thereto (the “Lenders”), K2 HealthVentures LLC (“K2HV”), an unrelated third party, as administrative agent for the Lenders, and Ankura Trust Company, LLC, an unrelated third party, as collateral agent for the Lenders, pursuant to which K2HV may provide us with term loans in an aggregate principal amount of up to a $50,000,000.
On August 7, 2020, we entered into an Open Market Sale AgreementSM (the “August 2020 Sale Agreement”) with Jefferies LLC (“Jefferies”), as sales agent, pursuant to which we may issue and sell, from time to time, through Jefferies, shares of our common stock. We will pay Jefferies a commission of 3.0% of the aggregate gross proceeds from each sale of common stock and have agreed to provide Jefferies with customary indemnification and contribution rights. We have also agreed to reimburse Jefferies for certain specified expenses. As of August 7, 2020, we were authorized to offer and sell up to $150 million of our common stock pursuant to the August 2020 Sale Agreement. As of December 31, 2020 we have sold 15,546,151 shares of our common stock for gross proceeds to us totaling $21,404,000, less issuance costs incurred of approximately $642,000.
We expect the cash and cash equivalents of approximately $85.4 million at December 31, 2020, $58.9 million of proceeds raised from the August 2020 Sale Agreement from January 1, 2021 through March 15, 2021, and the remaining $2.5 million of proceeds that we expect to receive under the 2018 CFF Award before the end of the first half of 2021 to be sufficient to meet our operating and capital requirements into 2024, based on planned expenditures.
| 22 |
We may seek additional capital through a combination of private and public equity offerings, debt financings and strategic collaborations. Debt financing, if obtained, may involve agreements that include covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, and could increase our expenses and require that our assets secure such debt.
Equity financing, if obtained, could result in dilution to our then existing stockholders and/or require such stockholders to waive certain rights and preferences. If such financing is not available on satisfactory terms, or is not available at all, we may be required to delay, scale back or eliminate the development of business opportunities and our operations and financial condition may be materially adversely affected. We can provide no assurances that any additional sources of financing will be available to us on favorable terms, if at all. In addition, if we are unable to secure sufficient capital to fund our operations, we may choose to pursue, as an alternative, strategic collaborations that could require us to share commercial rights to our drug candidates with third parties in ways that we currently do not intend or on terms that may not be favorable to us. If we choose to pursue additional indications and/or geographies for our drug candidates or otherwise expand more rapidly than we presently anticipate we may also need to raise additional capital sooner than expected.
Our Loan and Security Agreement contains restrictive and financial covenants that may limit our operating flexibility.
Our Loan Agreement with K2HV for up to $50,000,000 is secured by a lien covering substantially all of our personal property, excluding intellectual property.
The Loan Agreement contains customary representations, warranties and covenants. including restrictive covenants by the Company and Borrower limiting additional indebtedness, liens, mergers and acquisitions, dispositions, investments, distributions, subordinated debt, transactions with affiliates and fundamental changes. We therefore may not be able to engage in any of the foregoing types of transactions unless we obtain the consent of K2 Health Ventures or prepay the outstanding amount under the Loan Agreement. The Loan Agreement also contains certain financial covenants, including requirements to maintain unrestricted cash in the amount of $10,000,000 or the amount of all principal loans outstanding if certain regulatory and developmental milestones do not occur.
The restrictions and covenants in the Loan Agreement, as well as those contained in any future debt financing agreements that we may enter into, may restrict our ability to finance our operations and engage in, expand or otherwise pursue our business activities and strategies. Our ability to comply with these covenants and restrictions may be affected by events beyond our control, and breaches of these covenants and restrictions could result in a default under the loan agreement and any future financing agreements that we may enter into.
| 23 |
Risks Related to Product Development, Regulatory Approval, Manufacturing and Commercialization
Our near-term success is substantially dependent upon successful development of lenabasum, our first compound to enter clinical development, and our longer-term success is dependent upon successful development of other compounds in our pipeline or that we may acquire. If we are unable to generate revenues from lenabasum, or any other product candidates our ability to create stockholder value will be limited.
We do not generate revenues from any FDA approved drug products. Our current business currently depends heavily on the successful development, regulatory approval, and commercialization of lenabasum, which may never occur. Currently, our most advanced product candidate is lenabasum, for which we have completed a Phase 3 double-blind, placebo-controlled study in systemic sclerosis and a double-blind, placebo-controlled study Phase 2b study in cystic fibrosis, and have an ongoing double-blind, placebo-controlled study Phase 3 study in DM. The Phase 3 study in systemic sclerosis and Phase 2 study in cystic fibrosis did not meet their primary efficacy endpoints. There is no guarantee that our Phase 3 trial in DM will be successful or that, if positive, it would support FDA approval of a New Drug Application for lenabasum for treatment of DM.
We are currently conducting pre-clinical trials and testing for a number of CB1 inverse agonists and CB2 agonists. We note that most drug candidates never reach the clinical development stage and even those that do have only a small chance of successfully completing clinical development and gaining regulatory approval.
The coronavirus COVID-19 pandemic or the widespread outbreak of any other communicable disease could materially and adversely affect our business, financial condition and results of operations.
We face risks related to health epidemics or outbreaks of communicable diseases, for example, the outbreak around the world of the highly transmissible and pathogenic coronavirus, COVID-19. The outbreak of such communicable diseases, including COVID-19 and variants, could result in a widespread health crisis that could adversely affect general commercial activity and the economies and financial markets of many countries.
In December 2019, a novel strain of coronavirus, COVID-19, was reported to have surfaced in Wuhan, China and on March 11, 2020 was declared a pandemic by the World Health Organization. The extent to which COVID-19 may impact our preclinical and clinical trial operations will depend on future developments, which are highly uncertain and cannot be predicted with confidence, such as the duration of the outbreak, the severity of COVID-19, including its variants, and the effectiveness of actions to contain and treat COVID-19, including the effectiveness of vaccines and the ability of governments and healthcare providers to administer vaccines quickly and effectively
To limit the spread of COVID-19, governments have taken various actions from time to time including the issuance of travel restrictions, complete or partial prohibitions of non-essential activities, restrictions or shutdowns of non-essential businesses, stay-at-home orders and social distancing guidelines. Such events may result in a period of business, supply and drug product manufacturing disruption, and in reduced operations, any of which could materially affect our business, financial condition and results of operations.
Some of our business partners and manufacturing operations, including production of our commercial and clinical active pharmaceutical ingredient of lenabasum, are conducted internationally and may be impacted by the global spread of COVID-19. Although we have not experienced any material disruptions to these manufacturing operations or any material delays in shipping our commercial and clinical active pharmaceutical ingredient to our clinical trial sites to date, the continued impact resulting from the COVID-19 outbreak where we have operations, or if the COVID-19 outbreak in these areas were to increase in severity, and the measures taken by the governments of countries affected could adversely affect our business, financial condition or results of operations by limiting our ability to manufacture or ship materials or forcing temporary closure of facilities that we rely upon.
The global spread of COVID-19 has created significant volatility and uncertainty in global financial markets and may materially affect us economically and such conditions continue to persist. While the potential economic impact brought by, and the duration of, COVID-19 may be difficult to assess or predict, a widespread pandemic could result in significant disruption of global financial markets, reducing our ability to access capital, which could in the future negatively affect our liquidity. In addition, a recession or market correction resulting from the spread of COVID-19 could materially affect our business and the value of our common shares.
The continued spread of COVID-19 globally, and the resulting travel restrictions in place by governments to help stop the spread of COVID-19, could adversely impact our clinical trial operations, including the ability of our patients, principal investigators and site staff to travel to our clinical trial sites, and our ability to recruit and retain principal investigators and site staff who, as healthcare providers, may have heightened exposure to COVID-19 if an outbreak occurs in their geography. We cannot predict whether clinical testing sites will withdraw from participation in any of our studies temporarily or permanently. In addition, if the patients enrolled in our clinical trials become infected with COVID-19, we may have more adverse events and deaths in our clinical trials as a result. We may also face difficulties enrolling patients in our clinical trials if the patient populations that are eligible for our clinical trials are impacted by the coronavirus disease. Vulnerable patients, including patients with autoimmune disorders like the patients enrolled in our clinical trials, may be at a higher risk of contracting COVID-19 and may experience more severe symptoms from the disease, adversely affecting our chances for regulatory approval or requiring further clinical studies.
The COVID-19 outbreak may also affect the ability of our staff and the parties we work with to carry out our non-clinical, clinical, and drug development and manufacturing activities. We rely on clinical sites, investigators and other study staff, consultants, independent contractors, contract research organizations and other third-party service providers to assist us in managing, monitoring and otherwise carrying out our nonclinical studies and clinical trials. We also rely on consultants, independent contractors, contract development and manufacturing organizations, and other third-party service providers to assist us in managing, monitoring and otherwise carrying out our API production, formulation, and drug manufacturing activities. COVID-19 may affect the ability of any of these external people, organizations, or companies to devote sufficient time and resources to our programs or to travel to perform work for us.
Potential negative impacts of the COVID-19 outbreak on the conduct of current or future clinical studies include delays in gaining feedback from regulatory agencies, starting new clinical studies, and recruiting subjects to studies that are enrolling. Although we have implemented remote data monitoring procedures for our clinical trials, the potential negative impacts also include inability to have study visits at study sites, incomplete collection of safety and efficacy data, and higher rates of drop-out of subjects from ongoing studies, delays in site entry of study data into the data base, delays in monitoring of study data because of restricted physical access to study sites, delays in site responses to queries, delays in data-base lock, delays in data analyses, delays in time to top-line data, and delays in completing study reports. New or worsening COVID-19 disruptions or restrictions could have the potential to further negatively impact our non-clinical studies, clinical trials, and drug manufacturing activities.
As a result of the factors described above, the expected timeline for data readouts of our drug manufacturing activities, non-clinical studies, clinical trials, and certain regulatory filings may be negatively impacted, which would adversely affect our ability to obtain regulatory approval for and to commercialize our product candidates, increase our operating expenses and have a material adverse effect on our financial results.
If we are not able to obtain any required regulatory approvals for our drug candidates, we will not be able to commercialize our product candidates and our ability to generate revenue will be limited.
Our clinical trials may be unsuccessful, which would materially harm our business. Even if our ongoing clinical trials are successful, we will be required to conduct additional clinical trials to establish the safety and efficacy of our drug candidates, before a New Drug Application, or NDA, can be filed with the FDA for marketing approval of any of our drug candidates.
Clinical testing is expensive, is difficult to design and implement, can take many years to complete and is uncertain as to outcome. Success in early phases of pre-clinical and clinical trials does not ensure that later clinical trials will be successful, and interim results of a clinical trial do not necessarily predict final results. A failure of one or more of our clinical trials can occur at any stage of testing. We may experience numerous unforeseen events during, or as a result of, the clinical trial process that could delay or prevent our ability to receive regulatory approval or commercialize our drug candidates. The research, testing, manufacturing, labeling, packaging, storage, approval, sale, marketing, advertising and promotion, pricing, export, import and distribution of drug products are subject to extensive regulation by the FDA and other regulatory authorities in the United States and other countries, which regulations differ from country to country. We are not permitted to market any of our drug candidates as prescription pharmaceutical products in the United States until we receive approval of an NDA from the FDA or in foreign markets until we receive the requisite approval from comparable regulatory authorities in such countries. In the United States, the FDA generally requires the completion of clinical trials of each drug to establish its safety and efficacy and extensive pharmaceutical development to ensure its quality before an NDA is approved. Regulatory authorities in other jurisdictions impose similar requirements. Of the large number of drugs in development, only a small percentage result in the submission of an NDA to the FDA and even fewer are eventually approved for commercialization. We have never submitted an NDA to the FDA or any comparable applications to other regulatory authorities. If our development efforts for our drug candidates, including regulatory approval, are not successful for our planned indications, or if adequate demand for our drug candidates is not generated, our business will be harmed.
| 24 |
Receipt of necessary regulatory approval is subject to a number of risks, including the following:
| ■ | the FDA or comparable foreign regulatory authorities or institutional review boards, or IRBs, may disagree with the design or implementation of our clinical trials, including the shortened duration of treatment in our DETERMINE phase 3 study of lenabasum for treatment of dermatomyositis from 52 weeks to 26 weeks; | |
| ■ | we may not be able to provide acceptable evidence of the safety and efficacy of our drug candidates; | |
| ■ | the results of our clinical trials may not be satisfactory or may not meet the level of statistical or clinical significance required by the FDA, the European Medicines Agency, or EMA, or other comparable foreign regulatory authorities for marketing approval; | |
| ■ | the dosing of our drug candidates in a particular clinical trial may not be at an optimal level; | |
| ■ | patients in our clinical trials may suffer adverse effects for reasons that may or may not be related to our drug candidates; | |
| ■ | the data collected from clinical trials may not be sufficient to support the submission of an NDA or other submission or to obtain regulatory approval in the United States or elsewhere; | |
| ■ | the FDA or comparable foreign regulatory authorities may fail to approve the manufacturing processes or facilities of third-party manufacturers with which we contract for clinical and commercial supplies; | |
| ■ | the approval policies or regulations of the FDA or comparable foreign regulatory authorities may significantly change in a manner rendering our clinical data insufficient for approval; and | |
| ■ | the FDA or comparable foreign regulatory authorities may decide that the clinical trial endpoints we have chosen, the statistical analysis plans that we use, or any other parameter that we rely on to show the safety and efficacy of our drugs, are not parameters that can be used to support approval of our products. |
Failure to obtain regulatory approval for any of our drug candidates for the foregoing or any other reasons will prevent us from commercializing such product candidate as a prescription product, and our ability to generate revenue will be materially impaired. We cannot guarantee that regulators will agree with the endpoints that we have chosen to use in our clinical trials, our assessment of the results of our clinical trials or that such trials will be considered by regulators to have shown safety or efficacy of our product candidates. The FDA, EMA and other regulators have substantial discretion in the approval process and may refuse to accept any application or may decide that our data is insufficient for approval and require additional clinical trials, or pre-clinical or other studies. In addition, varying interpretations of the data obtained from pre-clinical and clinical testing could delay, limit or prevent regulatory approval of a product candidate.
We have only limited experience in filing the applications necessary to gain regulatory approvals and expect to rely on consultants and third party contract research organizations, or CROs, with expertise in this area to assist us in this process. Securing FDA approval requires the submission of pre-clinical, clinical and/or pharmacokinetic data, information about product manufacturing processes and inspection of facilities and supporting information to the FDA for each therapeutic indication to establish a product candidate’s safety and efficacy for each indication. Our drug candidates may prove to have undesirable or unintended side effects, toxicities or other characteristics that may preclude our obtaining regulatory approval or prevent or limit commercial use with respect to one or all intended indications.
| 25 |
The process of obtaining regulatory approvals is expensive, often takes many years, if approval is obtained at all, and can vary substantially based upon, among other things, the type, complexity and novelty of the product candidates involved, the jurisdiction in which regulatory approval is sought and the substantial discretion of regulatory authorities. Changes in the regulatory approval policy during the development period, changes in or the enactment of additional statutes or regulations, or changes in regulatory review for a submitted product application may cause delays in the approval or rejection of an application. Regulatory approval obtained in one jurisdiction does not necessarily mean that a product candidate will receive regulatory approval in all jurisdictions in which we may seek approval, but the failure to obtain approval in one jurisdiction may negatively impact our ability to seek approval in a different jurisdiction. Failure to obtain regulatory marketing approval for any of our drug candidates in any indication will prevent us from commercializing such product candidates, and our ability to generate revenue will be materially impaired.
Clinical drug development involves a lengthy and expensive process with an uncertain outcome, and results of earlier studies and trials may not be predictive of future trial results.
Clinical testing is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. Our drug candidates are in various stages of preclinical and clinical testing. Preclinical tests are performed at an early stage of a product's development and provide information about a drug candidate's safety and effectiveness on laboratory animals. Preclinical tests can last years. If a product passes its preclinical tests satisfactorily and we determine that further development is warranted, we would file an IND application for the product with the FDA, and if the FDA gives its approval, we would begin Phase 1 clinical tests. If Phase 1 test results are satisfactory and the FDA gives its approval, we can begin Phase 2 clinical tests. If Phase 2 test results are satisfactory and the FDA gives its approval, we can begin Phase 3 pivotal studies. Once clinical testing is completed and a BLA or NDA is filed with the FDA, it may take more than a year to receive FDA approval.
The results of pre-clinical studies and early clinical trials may not be predictive of the results of later-stage clinical trials. We cannot assure you that the FDA will view the results as we do or that any future trials of our drug candidates will achieve positive results. Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy traits despite having progressed through pre-clinical studies and initial clinical trials. A number of companies in the pharmaceutical industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials. Any future clinical trial results for our drug candidates may not be successful.
In all cases, we must show that a drug candidate is both safe and effective before the FDA, or drug approval agencies of other countries where we intend to sell the product, will approve it for sale. Our research and testing programs must comply with drug approval requirements both in the United States and in other countries, since we are developing our drug candidates with the intention to, or could later decide to, commercialize them both in the U.S. and abroad. A product may fail for safety or effectiveness at any stage of the testing process. A major risk we face is the possibility that none of our products under development will come through the testing process to final approval for sale, with the result that we cannot derive any commercial revenue from them after investing significant amounts of capital in multiple stages of preclinical and clinical testing. In addition, a number of factors could contribute to a lack of favorable safety and efficacy results for our drug candidates. For example, our trials could result in increased variability due to varying site characteristics, such as local standards of care, differences in evaluation period and surgical technique, and due to varying patient characteristics, including demographic factors and health status.
Even if we receive regulatory approval for our drug candidates, we still may not be able to successfully commercialize any of our products, and the revenue that we generate from sales, if any, may be limited.
If approved for marketing, the commercial success of our drug candidates will depend upon their acceptance by the medical community, including physicians, patients and health care payors. The degree of market acceptance of our drug candidates will depend on a number of factors, including:
| ■ | demonstration of clinical safety and efficacy; | |
| ■ | relative convenience, pill burden and ease of administration; | |
| ■ | the prevalence and severity of any adverse effects; | |
| ■ | the willingness of physicians to prescribe our drug candidates and of the target patient population to try new therapies; | |
| ■ | safety, tolerability and efficacy of our drug candidates compared to competing products; | |
| ■ | the introduction of any new products that may in the future become available to treat indications for which our drug candidates may be approved; | |
| ■ | new procedures or methods of treatment that may reduce the incidences of any of the indications in which our drug candidates may show utility; | |
| ■ | pricing and cost-effectiveness; | |
| ■ | the inclusion or omission of our drug candidates in applicable treatment guidelines; |
| 26 |
| ■ | the effectiveness of our or any future collaborators’ sales and marketing strategies; | |
| ■ | limitations or warnings contained in FDA-approved labeling; | |
| ■ | our ability to obtain and maintain sufficient third-party coverage or reimbursement from government health care programs, including Medicare and Medicaid, private health insurers and other third-party payors; and | |
| ■ | the willingness of patients to pay out-of-pocket in the absence of third-party coverage or reimbursement. |
If any of our drug candidates are approved, but do not achieve an adequate level of acceptance by physicians, health care payors and patients, we may not generate sufficient revenue and we may not be able to achieve or sustain profitability. Our efforts to educate the medical community and third-party payors on the benefits of our drug candidates may require significant resources and may never be successful.
In addition, even if we obtain regulatory approvals, the timing or scope of any approvals may prohibit or reduce our ability to commercialize our drug candidates successfully. For example, if the approval process takes too long, we may miss market opportunities and give other companies the ability to develop competing products or establish market dominance. Any regulatory approval we ultimately obtain may be limited or subject to restrictions or post-approval commitments that render our drug candidates not commercially viable. For example, regulatory authorities may approve our drug candidates for fewer or more limited indications than we request, may not approve the prices we intend to charge for our drug candidates, may grant approval contingent on the performance of costly post-marketing clinical trials, or may approve our drug candidates with labels that do not include the labeling claims necessary or desirable for the successful commercialization of a particular indication. Further, the FDA or comparable foreign regulatory authorities may place conditions on approvals, such as risk management plans and a Risk Evaluation and Mitigation Strategy, or REMS, to assure the safe use of the drug. If the FDA concludes a REMS is needed, the sponsor of the NDA must submit a proposed REMS; the FDA will not approve the NDA without an approved REMS, if required. A REMS could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. The FDA may also require a REMS for an approved product when new safety information emerges. Any of these limitations on approval or marketing could restrict the commercial promotion, distribution, prescription or dispensing of our drug candidates. Moreover, product approvals may be withdrawn for non-compliance with regulatory standards or if problems occur following the initial marketing of the product. Any of the foregoing scenarios could materially harm the commercial success of our drug candidates.
Even if we obtain marketing approval for our drug candidates, we will be subject to ongoing obligations and continued regulatory review, which may result in significant additional expense. Additionally, our drug candidates could be subject to labeling and other restrictions and withdrawal from the market and we may be subject to penalties if we fail to comply with regulatory requirements or if we experience unanticipated problems with our drug candidates.
Even if we obtain United States regulatory approval of our drug candidates for an indication, the FDA may still impose significant restrictions on their indicated uses or marketing or the conditions of approval, or impose ongoing requirements for potentially costly and time-consuming post-approval studies, including Phase 4 clinical trials, and post-market surveillance to monitor safety and efficacy. Our drug candidates will also be subject to ongoing regulatory requirements governing the manufacturing, labeling, packaging, storage, distribution, safety surveillance, advertising, promotion, recordkeeping and reporting of adverse events and other post-market information. These requirements include registration with the FDA, continued compliance with current Good Clinical Practices regulations, or cGCPs, for any clinical trials that we conduct post-approval, continued compliance with the CSA and ongoing review by the DEA. In addition, manufacturers of drug products and their facilities are subject to continual review and periodic inspections by the FDA and other regulatory authorities for compliance with current Good Manufacturing Practices, or cGMP, requirements relating to quality control, quality assurance and corresponding maintenance of records and documents.
| 27 |
With respect to sales and marketing activities by us or any future partner, advertising and promotional materials must comply with FDA rules in addition to other applicable federal, state and local laws in the United States and similar legal requirements in other countries. In the United States, the distribution of product samples to physicians must comply with the requirements of the U.S. Prescription Drug Marketing Act. Application holders must obtain FDA approval for product and manufacturing changes, depending on the nature of the change. We may also be subject, directly or indirectly through our customers and partners, to various fraud and abuse laws, including, without limitation, the U.S. Anti-Kickback Statute, U.S. False Claims Act, and similar state laws, which impact, among other things, our proposed sales, marketing, and scientific/educational grant programs. If we participate in the U.S. Medicaid Drug Rebate Program, the Federal Supply Schedule of the U.S. Department of Veterans Affairs, or other government drug programs, we will be subject to complex laws and regulations regarding reporting and payment obligations. All of these activities are also potentially subject to U.S. federal and state consumer protection and unfair competition laws. Similar requirements exist in many of these areas in other countries.
In addition, if any of our drug candidates are approved for an indication, our product labeling, advertising and promotion would be subject to regulatory requirements and continuing regulatory review. The FDA strictly regulates the promotional claims that may be made about prescription products. In particular, a product may not be promoted for uses that are not approved by the FDA as reflected in the product’s approved labeling. If we receive marketing approval for any of our drug candidates, physicians may nevertheless legally prescribe such products to their patients in a manner that is inconsistent with the approved label. However, if we are found to have promoted such off-label uses, we may become subject to significant liability and government fines. The federal government has levied large civil and criminal fines against companies for alleged improper promotion and has enjoined several companies from engaging in off-label promotion. The FDA has also requested that companies enter into consent decrees of permanent injunctions under which specified promotional conduct is changed or curtailed.
If we or a regulatory agency discover previously unknown problems with a product, such as adverse events of unanticipated severity or frequency or problems with the facility where the product is manufactured, or if we or our manufacturers fail to comply with applicable regulatory requirements, we may be subject to the following administrative or judicial sanctions:
| ■ | restrictions on the marketing or manufacturing of the product, withdrawal of the product from the market, or voluntary or mandatory product recalls; | |
| ■ | issuance of warning letters or untitled letters; | |
| ■ | injunctions or the imposition of civil or criminal penalties or monetary fines; | |
| ■ | suspension of any ongoing clinical trials; | |
| ■ | refusal to approve pending applications or supplements to approved applications filed by us, or suspension or revocation of product license approvals; | |
| ■ | suspension of, or imposition of restrictions on, operations, including costly new manufacturing requirements; or | |
| ■ | product seizure or detention or refusal to permit the import or export of product. |
The occurrence of any event or penalty described above may inhibit our ability to commercialize our drug candidates and generate revenue. Adverse regulatory action, whether pre- or post-approval, can also potentially lead to product liability claims and increase our product liability exposure.
| 28 |
The collaboration and license agreement, or the Collaboration Agreement, with Kaken Pharmaceuticals Co., Ltd., or Kaken, is important to our business. If we or Kaken fail to adequately perform under the Collaboration Agreement, or if we or Kaken terminate the Collaboration Agreement, the development and commercialization of lenabasum for the treatment of SSc and DM in Japan would be delayed or terminated and our business would be adversely affected.
On January 3, 2019, we entered into the Collaboration Agreement with Kaken, pursuant to which we granted to Kaken an exclusive license to commercialize and market lenabasum for the prevention and treatment of DM and SSc in Japan. Our ability to generate revenue under the Collaboration Agreement will depend in large part on our success in further clinical development of lenabasum and Kaken’s success in achieving regulatory approval for, and commercializing lenabasum, in Japan. Such efforts are subject to significant uncertainty. We have no control over the resources, time and effort that Kaken may devote to the commercialization of lenabasum. Any of several events or factors could have a material adverse effect on our ability to generate revenue from Kaken’s commercialization of lenabasum in Japan. For example, Kaken:
| ■ | may not achieve satisfactory levels of market acceptance and reimbursement by physicians, patients and third-party payers for lenabasum for the treatment of DM and SSc; | |
| ■ | may not compete successfully against other products and therapies for DM and SSc; | |
| ■ | may have to comply with additional requests and recommendations from foreign regulatory authorities; | |
| ■ | may not make all regulatory filings and obtain all necessary approvals from foreign regulatory agencies and all commercially necessary reimbursement approvals; | |
| ■ | may not commit sufficient resources to the marketing and distribution of lenabasum, whether for competitive or strategic reasons or otherwise due to a change in business priorities; and | |
| ■ | may cease to perform its obligations under the terms of the Collaboration Agreement. |
In addition, pursuant to the Collaboration Agreement, we and Kaken have agreed to negotiate in good faith to enter into a supply agreement and a quality agreement. There can be no assurance that we will be able to reach mutually agreeable terms on such agreements with Kaken, and the absence of agreement on such terms would prevent us from gaining the expected benefit of the Collaboration Agreement.
Further, we and Kaken agreed to provide mutual indemnification against losses in connection with third-party claims arising out of breaches of or inaccuracies in the Collaboration Agreement, gross negligence or willful misconduct, and the development or commercialization of lenabasum pursuant to the Collaboration Agreement. Conflicts may arise in connection with these indemnification obligations.
After a specified period of time, Kaken may unilaterally terminate the Collaboration Agreement on 180 days’ prior written notice without any reason and without any further commitment. Kaken may also terminate in the event of certain safety concerns and clinical failures, and either we or Kaken may terminate in the case of the other party’s material breach or insolvency. Termination of the Collaboration Agreement could cause significant delays in our product candidate development and commercialization efforts, which could prevent us from commercializing lenabasum without first expanding our internal capabilities or entering into another agreement with a third party. Any suitable alternative collaboration or license agreement would take considerable time to negotiate and could also be on less favorable terms to us.
We have entered into, and may in the future enter into, collaboration agreements for the licensing, development and ultimate commercialization of some of our drug candidates. In such cases, we will depend greatly on our third-party collaborators to license, develop and commercialize such drug candidates, and they may not meet our expectations.
We may enter into further co-development and commercialization partnerships for our drug candidates where appropriate. The process of identifying collaborators and negotiating collaboration agreements for the licensing, development and ultimate commercialization of some of our drug candidates may cause delays and increased costs. We may not be able to enter into collaboration agreements on terms favorable to us or at all. Furthermore, some of those agreements may give substantial responsibility over our drug candidates to the collaborator. Some collaborators may be unable or unwilling to devote sufficient resources to develop our drug candidates as their agreements require. They often face business risks similar to ours, and this could interfere with their efforts. Also, collaborators may choose to devote their resources to products that compete with ours. If a collaborator does not successfully develop any one of our products, we will need to find another collaborator to do so. The success of our search for a new collaborator will depend on our legal right to do so at the time and whether the product remains commercially viable.
| 29 |
If we enter into collaboration agreements for one or more of our drug candidates, the success of such drug candidates will depend in great part upon our and our collaborators’ success in promoting them as superior to other treatment alternatives. We believe that our drug candidates can be proven to offer disease treatment with notable advantages over drugs in terms of patient compliance and effectiveness. However, there can be no assurance that we will be able to prove these advantages or that the advantages will be sufficient to support the successful commercialization of our drug candidates.
We currently have a limited sales and marketing organization. If we are unable to secure a sales and marketing partner or establish satisfactory sales and marketing capabilities, we may not successfully commercialize our drug candidates.
At present, we have a team of three employees in the commercial organization in order to commercialize products that are approved for commercial sales in the United States. We must either collaborate with third parties that have such commercial infrastructure or continue to develop our own sales and marketing infrastructure. If we are not successful in entering into appropriate collaboration arrangements, or recruiting sales and marketing personnel or in building a sales and marketing infrastructure, we will have difficulty successfully commercializing our drug candidates, which would adversely affect our business, operating results and financial condition.
We may not be able to enter into collaboration agreements on terms acceptable to us or at all. In addition, even if we enter into such relationships, we may have limited or no control over the sales, marketing and distribution activities of these third parties. Our future revenues may depend heavily on the success of the efforts of these third parties. If we elect to establish a sales and marketing infrastructure we may not realize a positive return on this investment. In addition, we will have to compete with established and well-funded pharmaceutical and biotechnology companies to recruit, hire, train and retain sales and marketing personnel. Factors that may inhibit our efforts to commercialize our drug candidates without strategic partners or licensees include:
| ■ | our inability to recruit and retain adequate numbers of effective sales and marketing personnel; | |
| ■ | the inability of sales personnel to obtain access to or persuade adequate numbers of physicians to prescribe our drug candidates; | |
| ■ | the lack of complementary products to be offered by sales personnel, which may put us at a competitive disadvantage relative to companies with more extensive product lines; and | |
| ■ | unforeseen costs and expenses associated with creating an independent sales and marketing organization. |
We face competition from other biotechnology and pharmaceutical companies and our operating results will suffer if we fail to compete effectively.
The biotechnology and pharmaceutical industries are intensely competitive and subject to rapid and significant technological change. We have competitors in a number of jurisdictions, many of which have substantially greater name recognition, commercial infrastructures and financial, technical and personnel resources than we have. Established competitors may invest heavily to quickly discover and develop novel compounds that could make our drug candidates obsolete or uneconomical. Any new product that competes with an approved product may need to demonstrate compelling advantages in efficacy, cost, convenience, tolerability and safety to be commercially successful. Other competitive factors, including generic competition, could force us to lower prices or could result in reduced sales. In addition, new products developed by others could emerge as competitors to our drug candidates. If we are not able to compete effectively against our current and future competitors, our business will not grow and our financial condition and operations will suffer.
| 30 |
Recently enacted and future legislation may increase the difficulty and cost for us to obtain marketing approval of and commercialize our drug candidates and affect the prices we may obtain.
In the United States and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval for our drug candidates, restrict or regulate post-approval activities and affect our ability to profitably sell our drug candidates. Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for pharmaceutical products. We do not know whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of our drug candidates, if any, may be. In addition, increased scrutiny by the U.S. Congress of the FDA’s approval process may significantly delay or prevent marketing approval, as well as subject us to more stringent product labeling and post-marketing testing and other requirements.
In the United States, under the Medicare Modernization Act, or MMA, Medicare Part D provides coverage to the elderly and disabled for outpatient prescription drugs by approving and subsidizing prescription drug plans offered by private insurers. The MMA also authorizes Medicare Part D prescription drug plans to use formularies where they can limit the number of drugs that will be covered in any therapeutic class. The Part D plans use their formulary leverage to negotiate rebates and other price concessions from drug manufacturers. Also under the MMA, Medicare Part B provides coverage to the elderly and disabled for physician-administered drugs on the basis of the drug’s average sales price, a price that is calculated according to regulatory requirements and that the manufacturer reports to Medicare quarterly.
Both Congress and the Centers for Medicare & Medicaid Services (CMS), the agency that administers the Medicare program, from time to time consider legislation, regulations, or other initiatives to reduce drug costs under Medicare Parts B and D. For example, under the 2010 Affordable Care Act, drug manufacturers are required to provide a 50% discount on prescriptions for branded drugs filled while the beneficiary is in the Medicare Part D coverage gap, also known as the “donut hole.” There have been legislative proposals to repeal the “non-interference” provision of the MMA to allow CMS to leverage the Medicare market share to negotiate larger Part D rebates. Further cost reduction efforts could decrease the coverage and price that we receive for our drug candidates and could seriously harm our business. Private payors often follow Medicare coverage policy and payment limitations in setting their own reimbursement rates, and any reduction in reimbursement under the Medicare program may result in a similar reduction in payments from private payors.
The 2010 Affordable Care Act is intended to broaden access to health insurance and reduce or constrain the growth of healthcare spending. Further, the Affordable Care Act imposes a significant annual fee on companies that manufacture or import branded prescription drug products. It also increased the amount of the rebates drug manufacturers must pay to state Medicaid programs, required that Medicaid rebates be paid on managed Medicaid utilization, and increased the additional rebate on “line extensions” (such as extended release formulations) of solid oral dosage forms of branded products. The law also contains substantial provisions affecting fraud and abuse compliance and transparency, which may require us to modify our business practices with healthcare practitioners, and incur substantial costs to ensure compliance.
| 31 |
In addition, other legislative changes have been proposed and adopted in the United States since the ACA was enacted. For example, the Budget Control Act of 2011 included, among other things, provisions that have led to 2% across-the-board reductions in Medicare payment amounts. Several states have adopted or are considering adopting laws that require pharmaceutical companies to provide notice prior to raising prices and to justify price increases. We expect that additional healthcare reform measures will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, and in turn could significantly reduce the projected value of certain development projects and reduce our profitability.
Our future growth depends, in part, on our ability to enter into and succeed in markets outside of the United States, where we may choose to rely on third party collaborations and will be subject to additional regulatory and commercial burdens, risks and other uncertainties.
Our future profitability will depend, in part, on our ability to gain approval of and commercialize our drug candidates in non-U.S. markets. In some or all of these non-U.S. markets, we intend to enter into licensing and contractual collaborations with third parties, such as Kaken, to handle some or all of the tasks and responsibilities necessary to succeed. Our activities in non-U.S. markets are subject to additional risks and uncertainties, including:
| ■ | our ability to enter into favorable licensing and contractual arrangements with our partners; | |
| ■ | our ability to select partners who are capable of achieving success at the tasks they agree to perform; | |
| ■ | obtaining timely and sufficient favorable approval terms for our drug candidates; | |
| ■ | obtaining favorable pricing and reimbursement; | |
| ■ | our inability to directly control commercial activities because we are relying on third parties; | |
| ■ | the burden of complying with complex and changing foreign regulatory, tax, accounting and legal requirements; | |
| ■ | different medical practices and customs in foreign countries affecting acceptance in the marketplace; | |
| ■ | import or export licensing requirements; | |
| ■ | longer accounts receivable collection times; | |
| ■ | longer lead times for shipping; | |
| ■ | language barriers for technical training; | |
| ■ | reduced protection of intellectual property rights in some foreign countries; | |
| ■ | foreign currency exchange rate fluctuations; and | |
| ■ | the interpretation of contractual provisions governed by foreign laws in the event of a contract dispute. |
International sales of our drug candidates could also be adversely affected by the imposition of governmental controls, political and economic instability, and trade restrictions and changes in tariffs, any of which may adversely affect our results of operations.
| 32 |
If we market our drug candidates in a manner that violates healthcare fraud and abuse laws, or if we violate government price reporting laws, we may be subject to civil or criminal penalties.
The FDA enforces laws and regulations which require that the promotion of pharmaceutical products be consistent with the approved prescribing information. While physicians may prescribe an approved product for a so-called “off label” use, it is unlawful for a pharmaceutical company to promote its products in a manner that is inconsistent with its approved label and any company which engages in such conduct may be subject to significant liability. Similarly, industry codes in the European Union and other foreign jurisdictions prohibit companies from engaging in off-label promotion and regulatory agencies in various countries enforce violations of the code with civil penalties. While we intend to ensure that our promotional materials are consistent with our label, regulatory agencies may disagree with our assessment and may issue untitled letters, warning letters or may institute other civil or criminal enforcement proceedings. In addition to FDA restrictions on marketing of pharmaceutical products, several other types of state and federal healthcare fraud and abuse laws have been applied in recent years to restrict certain marketing practices in the pharmaceutical industry. These laws include the U.S. Anti-Kickback Statute, U.S. False Claims Act and similar state laws. Because of the breadth of these laws and the narrowness of the safe harbors, it is possible that some of our business activities could be subject to challenge under one or more of these laws.
The U.S. Anti-Kickback Statute prohibits, among other things, knowingly and willfully offering, paying, soliciting or receiving remuneration to induce, or in return for, purchasing, leasing, ordering or arranging for the purchase, lease or order of any healthcare item or service reimbursable under Medicare, Medicaid or other federally financed healthcare programs. This statute has been interpreted broadly to apply to arrangements between pharmaceutical manufacturers on the one hand and prescribers, purchasers and formulary managers on the other. Although there are several statutory exemptions and regulatory safe harbors protecting certain common activities from prosecution, the exemptions and safe harbors are drawn narrowly, and practices that involve remuneration intended to induce prescribing, purchasing or recommending may be subject to scrutiny if they do not qualify for an exemption or safe harbor. Our practices may not, in all cases, meet all of the criteria for safe harbor protection from anti-kickback liability. Moreover, recent health care reform legislation has strengthened these laws. For example, the Health Care Reform Law, among other things, amends the intent requirement of the U.S. Anti-Kickback Statute and criminal health care fraud statutes; a person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it. In addition, the Health Care Reform Law provides that the government may assert that a claim including items or services resulting from a violation of the U.S. Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the U.S. False Claims Act. Federal false claims laws prohibit any person from knowingly presenting, or causing to be presented, a false claim for payment to the federal government or knowingly making, or causing to be made, a false statement to get a false claim paid.
Over the past few years, pharmaceutical and other healthcare companies have been prosecuted under these laws for a variety of alleged promotional and marketing activities, such as: allegedly providing free trips, free goods, sham consulting fees and grants and other monetary benefits to prescribers; reporting to pricing services inflated average wholesale prices that were then used by federal programs to set reimbursement rates; engaging in off-label promotion that caused claims to be submitted to Medicare or Medicaid for non-covered, off-label uses; and submitting inflated best price information to the Medicaid Rebate Program to reduce liability for Medicaid rebates. Most states also have statutes or regulations similar to the U.S. Anti-Kickback Statute and the U.S. False Claims Act, which apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the payor. Sanctions under these federal and state laws may include substantial civil monetary penalties, exclusion of a manufacturer’s products from reimbursement under government programs, substantial criminal fines and imprisonment.
We are, and will be, completely dependent on third parties to manufacture our drug candidates, and our commercialization of our drug candidates could be halted, delayed or made less profitable if those third parties fail to obtain manufacturing approval from the FDA or comparable foreign regulatory authorities, fail to provide us with sufficient quantities of our drug candidates or fail to do so at acceptable quality levels or prices.
We do not currently have, nor do we plan to acquire, the capability or infrastructure to manufacture the active pharmaceutical ingredients of our drug candidates, or the finished drug products, for use in our clinical trials or for commercial product, if any. As a result, we will be obligated to rely on contract manufacturers if and when our drug candidates are approved for commercialization.
| 33 |
We currently rely on a single foreign supplier for manufacturing the starting chemical intermediates and finished bulk drug product for lenabasum. We also rely on a single foreign supplier for the manufacturing of the finished lenabasum capsules. The facilities used by our two contract manufacturers to manufacture lenabasum must be approved by the FDA pursuant to inspections that will be conducted after we submit our NDAs to the FDA. We do not control the manufacturing processes of, and are completely dependent on, our two contract manufacturing partners for compliance with cGMPs for manufacture of all active drug substances and finished drug products. These cGMP regulations cover all aspects of the manufacturing, testing, quality control and record keeping relating to our drug candidates. If our contract manufacturers cannot successfully manufacture material that conforms to our specifications and the strict regulatory requirements of the FDA or others, they will not be able to secure and/or maintain regulatory approval for their manufacturing facilities. If the FDA or a comparable foreign regulatory authority does not approve these facilities for the manufacture of lenabasum or our other product candidates or if it withdraws any such approval in the future, we may need to find alternative manufacturing facilities, which would significantly impact our ability to develop, obtain regulatory approval for or market our drug candidates, if approved.
Our contract manufacturers will be subject to ongoing periodic unannounced inspections by the FDA and corresponding state and foreign agencies for compliance with cGMPs and similar regulatory requirements. We will not have control over our contract manufacturers’ compliance with these regulations and standards. Failure by any of our contract manufacturers to comply with applicable regulations could result in sanctions being imposed on us, including fines, injunctions, civil penalties, failure to grant approval to market our drug candidates, delays, suspensions or withdrawals of approvals, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect our business. In addition, we will not have control over the ability of our contract manufacturers to maintain adequate quality control, quality assurance and qualified personnel. Failure by our contract manufacturers to comply with or maintain any of these standards could adversely affect our ability to develop, obtain regulatory approval for or market our drug candidates.
If for any reason, these third parties are unable or unwilling to perform, we may not be able to terminate our agreements with them, and we may not be able to locate alternative manufacturers or formulators or enter into favorable agreements with them and we cannot be certain that any such third parties will have the manufacturing capacity to meet future requirements. If these manufacturers or any alternate manufacturer of finished drug product experiences any significant difficulties in its respective manufacturing processes for our active pharmaceutical ingredient, or API, or our finished products or should cease doing business with us, we could experience significant interruptions in the supply of our drug candidates or may not be able to create a supply of our drug candidates at all. Were we to encounter manufacturing issues, our ability to produce a sufficient supply of our drug candidates might be negatively affected. Our inability to coordinate the efforts of our third party manufacturing partners, or the lack of capacity available at our third party manufacturing partners, could impair our ability to supply our drug candidates at required levels. Because of the significant regulatory requirements that we would need to satisfy in order to qualify a new bulk or finished product manufacturer, if we face these or other difficulties with our current manufacturing partners, we could experience significant interruptions in the supply of our drug candidates if we decided to transfer the manufacture of our drug candidates to one or more alternative manufacturers in an effort to deal with the difficulties.
Any manufacturing problem or the loss of a contract manufacturer could be disruptive to our operations and result in lost sales. Additionally, we rely on third parties to supply the raw materials needed to manufacture our potential products. Any reliance on suppliers may involve several risks, including a potential inability to obtain critical materials and reduced control over production costs, delivery schedules, reliability and quality. Any unanticipated disruption to a future contract manufacturer caused by problems at suppliers could delay shipment of our drug candidates, increase our cost of goods sold and result in lost sales.
We cannot guarantee that our manufacturing and supply partners will be able to manufacture our drug candidates at commercial scale on a cost-effective basis. If the commercial-scale manufacturing costs of our drug candidates are higher than expected, these costs may significantly impact our operating results. In order to reduce costs, we may need to develop and implement process improvements. However, in order to do so, we will need, from time to time, to notify or make submissions with regulatory authorities, and the improvements may be subject to approval by such regulatory authorities. We cannot be sure that we will receive these necessary approvals or that these approvals will be granted in a timely fashion. We also cannot guarantee that we will be able to enhance and optimize output in our commercial manufacturing process. If we cannot enhance and optimize output, we may not be able to reduce our costs over time.
| 34 |
There are risks associated with scaling up manufacturing to commercial scale. If our contract manufacturers are unable to manufacture our drug candidates on a commercial scale, this could potentially delay regulatory approval and commercialization or materially adversely affect our results of operations.
There are risks associated with scaling up manufacturing to commercial volumes including, among others, cost overruns, technical problems with process scale-up, process reproducibility, stability issues, and lot consistency. Even if we obtain regulatory approval for our drug candidates, there is no assurance that our contract manufacturers will be able to manufacture the approved products to specifications acceptable to the FDA or other regulatory authorities, to produce them in sufficient quantities to meet the requirements for the potential launch of the product or to meet potential future demand. If our manufacturers are unable to produce sufficient quantities of approved products for commercialization, either on a timely basis or at all, our commercialization efforts would be impaired, which would have a material adverse effect on our business, financial condition, results of operations and growth prospects.
Our lead product candidate, lenabasum, is currently classified as a Schedule I controlled substance subject to U.S. controlled substance laws and regulations, including regulations of the Drug Enforcement Agency and the U.S. Food and Drug Administration. Failure to obtain the necessary licenses and registrations and failure to comply with these laws could result in the delay in the manufacturing and distribution of lenabasum and could delay the completion of clinical studies. Such delays and the cost of compliance with these laws and regulations, could adversely affect our business operations and our financial condition.
In the United States, our lead product candidate, lenabasum, is currently classified as a Schedule I controlled substance as defined in the Controlled Substance Act, or CSA. This designation is mainly based on lenabasum’s chemical structure (it is a synthetic compound that is structurally related to the non-psychoactive terminal metabolite of tetrahydrocannabinol).
Schedule I controlled substances are pharmaceutical products subject to specific regulations under the CSA, which establishes, among other things, certain registration, manufacturing quotas, security, recordkeeping, reporting, import, export and other requirements administered by the DEA. All parties responsible for the manufacturing, distribution and testing of the drug in clinical studies must apply for and obtain a license from the DEA before they are permitted to perform these activities with lenabasum. Furthermore, these parties must have the security, control, recordkeeping, reporting and inventory mechanisms required by the DEA to prevent drug loss and diversion. All licensed facilities are required to renew their registrations annually if they intend to continue to work with our drug. The DEA conducts periodic inspections of certain registered establishments that handle controlled substances. We have been working with our manufacturers, distributors, exporters and clinical sites to obtain the necessary licenses to work with lenabasum. The parties responsible for the manufacturing, distribution and export of lenabasum have already applied for and have been granted DEA licenses and a number of institutions responsible for conducting our current clinical studies have also been granted DEA licenses. However, the failure to maintain the necessary registrations, and the delay or failure of additional clinical sites to obtain DEA registrations, could delay the manufacturing, distribution and export of lenabasum and could delay the completion of the clinical studies. Furthermore, failure to maintain compliance with the CSA, particularly non-compliance resulting in loss or diversion, could result in regulatory action that could have a material adverse effect on our business, financial condition and results of operations. The DEA may seek civil penalties, refuse to renew necessary registrations, or initiate proceedings to restrict, suspend or revoke those registrations. In certain circumstances, violations could lead to criminal proceedings. In addition, if the FDA, DEA, or any foreign regulatory authority determines that lenabasum may have potential for abuse, it may require us to generate more clinical or other data than we currently anticipate to establish whether or to what extent the substance has an abuse potential, which could increase the cost and/or delay the launch of lenabasum.
Individual states have also established controlled substance laws and regulations. Though state-controlled substances laws often mirror federal law, because the states are separate jurisdictions, they may separately schedule drugs, as well. While some states automatically schedule a drug based on federal action, other states schedule drugs through rulemaking or a legislative action. The requirement for state registrations could also result in delay of the manufacturing and distribution of lenabasum or in the completion of our clinical studies. We and our manufacturing vendors and clinical sites must also obtain separate state registrations, permits or licenses in order to be able to obtain, handle and distribute controlled substances for clinical trials or commercial sale, and failure to meet applicable regulatory requirements could lead to enforcement and sanctions by the states in addition to those from the DEA or otherwise arising under federal law.
| 35 |
The manufacturing and distribution of lenabasum is subject to the DEA’s annual manufacturing and procurement quota requirements. The annual quota allocated to us or our contract manufacturers for the controlled substances in lenabasum may not be sufficient to complete clinical trials. Consequently, any delay or refusal by the DEA in establishing our, or our contract manufacturers’, procurement and/or production quota for controlled substances could delay or stop our clinical trials or product launches, which could have a material adverse effect on our business, financial position and operations.
While lenabasum is a Schedule I controlled substance, if lenabasum is approved for medical use by the FDA, it will have satisfied the “accepted medical use” requirement of the CSA. If and when lenabasum receives FDA approval, the DEA will make a scheduling determination and place lenabasum in a schedule other than Schedule I or declassify it in order for it to be prescribed to patients in the United States. As part of the scheduling determination, FDA will assess the abuse and dependence potential of lenabasum and make a scheduling recommendation to DEA. If approved by the FDA, the length of time the DEA takes to complete the rescheduling or declassification of lenabasum is uncertain and could be lengthy and we will not be able to sell the drug until the rescheduling is complete. Any delays in the rescheduling could have a material adverse impact on our results of operations.
Delays in shipping our drug candidates could have a material adverse effect on our business, results of operations and financial condition.
The import and export of our drug candidates requires import and export licenses. In addition, because lenabasum is currently a Schedule I controlled substance in the United States, in addition to the FDA and U.S. Customs and Border Protection, its import and export is also regulated by the DEA. We may not be granted, or if granted, maintain, such licenses for import or export from the authorities these regulatory agencies. Even if we obtain the relevant licenses, shipments of our drug candidates may be held up in transit by any of these authorities, which could cause significant delays and may lead to product batches which no longer meet specifications for use in clinical trials or commercial distribution. Such events could result in delayed development timelines, increased expenses and partial or total loss of revenue from our drug candidates.
We expect that we will rely on third parties to assist us in conducting clinical trials for our drug candidates. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval for or commercialize our drug candidates and our business would be substantially harmed.
We expect to enter into agreements with third-party CROs to assist us in conducting and managing our clinical programs, including contracting with clinical sites to perform our clinical studies. We plan to rely on these parties for execution of clinical studies for our drug candidates and we will control only certain aspects of conducting the clinical studies. Nevertheless, we will be responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards, and our reliance on CROs and clinical sites will not relieve us of our regulatory responsibilities. We and our CROs will be required to comply with cGCPs, which are regulations and guidelines enforced by the FDA, the Competent Authorities of the Member States of the European Economic Area and comparable foreign regulatory authorities for any products in clinical development. The FDA enforces these cGCP regulations through periodic inspections of trial sponsors, principal investigators and trial sites. If we or our CROs fail to comply with applicable cGCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot assure you that, upon inspection, the FDA will determine that any of our clinical trials comply with cGCPs. In addition, our clinical trials must be conducted with products produced under cGMP regulations and will require a large number of test subjects. Our failure or the failure of our CROs or clinical sites to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process and could also subject us to enforcement action up to and including civil and criminal penalties.
| 36 |
Although we intend to design the clinical trials for our drug candidates in consultation with CROs, we expect that the CROs will manage and assist us with the clinical trials conducted at contracted clinical sites. As a result, many important aspects of our drug development programs would be outside of our direct control. In addition, the CROs and clinical sites may not perform all of their obligations under arrangements with us or in compliance with regulatory requirements. If the CROs or clinical sites do not perform clinical trials in a satisfactory manner, or if they breach their obligations to us or fail to comply with regulatory requirements, the development and commercialization of our drug candidates for the subject indications may be delayed or our development program materially and irreversibly harmed. We cannot control the amount and timing of resources these CROs and clinical sites will devote to our program or our drug candidates. If we are unable to rely on clinical data collected by our CROs, we could be required to repeat, extend the duration of, or increase the size of our clinical trials, which could significantly delay commercialization and require significantly greater expenditures.
If any of our relationships with these third-party CROs or clinical sites terminate, we may not be able to enter into arrangements with alternative CROs or clinical sites. If CROs do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols, regulatory requirements or for other reasons, any such clinical trials may be extended, delayed or terminated, and we may not be able to obtain regulatory approval for or successfully commercialize our drug candidates. As a result, our financial results and the commercial prospects for our drug candidates would be harmed, our costs could increase and our ability to generate revenue could be delayed.
Any termination or suspension of or delays in the commencement or completion of any necessary studies of our drug candidates for any indications could result in increased costs to us, delay or limit our ability to generate revenue and adversely affect our commercial prospects.
The commencement and completion of clinical studies can be delayed for a number of reasons, including delays related to:
| ■ | the FDA failing to grant permission to proceed and placing the clinical study on hold; | |
| ■ | subjects failing to enroll or remain in our trials at the rate we expect; | |
| ■ | a facility manufacturing any of our drug candidates being ordered by the FDA or other government or regulatory authorities to temporarily or permanently shut down due to violations of cGMP requirements or other applicable requirements, or cross-contaminations of product in the manufacturing process; | |
| ■ | any changes to our manufacturing process that may be necessary or desired; | |
| ■ | subjects choosing an alternative treatment for the indications for which we are developing our drug candidates, or participating in competing clinical studies; | |
| ■ | subjects experiencing severe or unexpected drug-related adverse effects; | |
| ■ | reports of similar technologies and products raising safety and/or efficacy concerns; | |
| ■ | third-party clinical investigators losing their license or permits necessary to perform our clinical trials, not performing our clinical trials on our anticipated schedule or employing methods consistent with the clinical trial protocol, cGCP requirements, or other third parties not performing data collection and analysis in a timely or accurate manner; | |
| ■ | inspections of clinical study sites by the FDA or IRBs finding regulatory violations that require us to undertake corrective action, result in suspension or termination of one or more sites or the imposition of a clinical hold on the entire study, or that prohibit us from using some or all of the data in support of our marketing applications; | |
| ■ | third-party contractors becoming debarred or suspended or otherwise penalized by the FDA or other government or regulatory authorities for violations of regulatory requirements, in which case we may need to find a substitute contractor, and we may not be able to use some or any of the data produced by such contractors in support of our marketing applications; |
| 37 |
| ■ | one or more IRBs refusing to approve, suspending or terminating the study at an investigational site precluding enrollment of additional subjects, or withdrawing its approval of the trial; reaching agreement on acceptable terms with prospective CROs and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; | |
| ■ | deviations of the clinical sites from trial protocols or dropping out of a trial; | |
| ■ | adding new clinical trial sites; | |
| ■ | the inability of the CRO to execute any clinical trials for any reason; | |
| ■ | government or regulatory delays or “clinical holds” requiring suspension or termination of a trial; and | |
| ■ | delays related to the impacts of COVID-19, including slowdowns in enrollment or our ability complete our clinical trials on our expected timeline. |
Product development costs for our drug candidates will increase if we have delays in testing or approval or if we need to perform more or larger clinical studies than planned. Additionally, changes in regulatory requirements and policies may occur and we may need to amend study protocols to reflect these changes. Amendments may require us to resubmit our study protocols to the FDA and IRBs for reexamination, which may impact the costs, timing or successful completion of that study. If we experience delays in completion of, or if we, the FDA or other regulatory authorities, any IRBs, or other reviewing entities, or any of our clinical study sites suspend or terminate any of our clinical studies of our drug candidates, our commercial prospects may be materially harmed and our ability to generate product revenues will be delayed. Any delays in completing our clinical trials will increase our costs, slow down our development and approval process and jeopardize our ability to commence product sales and generate revenues. Any of these occurrences may harm our business, financial condition and prospects significantly. In addition, many of the factors that cause, or lead to, termination or suspension of, or a delay in the commencement or completion of, clinical studies may also ultimately lead to the denial of regulatory approval of our drug candidates. In addition, if one or more clinical studies are delayed, our competitors may be able to bring products to market before we do, and the commercial viability of our drug candidates could be significantly reduced.
We may not be able to obtain or maintain orphan drug designation or exclusivity for our product candidates.
We have been granted orphan drug designation in the United States and in the European Union for lenabasum for the treatment of CF, SSc and DM. Upon receipt of regulatory approval, orphan drug status will provide us with seven years of market exclusivity in the United States under the Orphan Drug Act. However, there is no guarantee that the FDA will grant orphan drug designation for any of our drug candidates for any future indication, which would make us ineligible for the additional exclusivity and other benefits of orphan drug designation. Moreover, there can be no assurance that another company also holding orphan drug designation for the same indication or which may receive orphan drug designation in the future will not receive approval prior to us, in which case our competitor would have the benefit of the seven years of market exclusivity, and we would be unable to commercialize our product for the same indication until the expiration of such seven-year period. Even if we are the first to obtain approval for the orphan drug indication, there are circumstances under which a competing product may be approved for the same indication during our seven-year period of exclusivity.
Under the Orphan Drug Act, the FDA may grant orphan drug designation to a drug intended to treat a rare disease or condition, which is generally a disease or condition that affects fewer than 200,000 individuals in the United States and for which there is no reasonable expectation that the cost of developing and making a drug available in the Unites States for this type of disease or condition will be recovered from sales of the product. Orphan drug designation must be requested before submitting an NDA. After the FDA grants orphan drug designation, the identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. Orphan designation does not convey any advantage in or shorten the duration of regulatory review and approval process. In addition to the potential period of exclusivity, orphan designation makes a company eligible for grant funding of up to $400,000 per year for four years to defray costs of clinical trial expenses, tax credits for clinical research expenses and potential exemption from the FDA application user fee.
| 38 |
If a product that has orphan designation subsequently receives the first FDA approval for the disease or condition for which it has such designation, the product is entitled to orphan drug exclusivity, which means the FDA may not approve any other applications to market the same drug for the same indication for seven years, except in limited circumstances, such as (i) the drug’s orphan designation is revoked; (ii) its marketing approval is withdrawn; (iii) the orphan exclusivity holder consents to the approval of another applicant’s product; (iv) the orphan exclusivity holder is unable to assure the availability of a sufficient quantity of drug; or (v) a showing of clinical superiority to the product with orphan exclusivity by a competitor product. If a drug designated as an orphan product receives marketing approval for an indication broader than what is designated, it may not be entitled to orphan drug exclusivity. There can be no assurance that we will receive orphan drug designation for any of our drug candidates for any additional indications, if we elect to seek such designation.
Any fast track designation or grant of priority review status by the FDA may not actually lead to a faster development or regulatory review or approval process, nor will it assure FDA approval of our product candidates. Additionally, our product candidates may treat indications that do not qualify for priority review vouchers.
We have received fast track designation for lenabasum for the treatment of cystic fibrosis and systemic sclerosis in the United States and European Union and may seek fast track designation or priority review of applications for approval of our product candidate for future indications. If a drug is intended for the treatment of a serious or life-threatening condition and the drug demonstrates the potential to address unmet medical needs for this condition, the drug sponsor may apply for FDA fast track designation. If a product candidate offers major advances in treatment, the FDA may designate it eligible for priority review. The FDA has broad discretion whether or not to grant these designations, so even if we believe a particular product candidate is eligible for these designations, we cannot assure you that the FDA would decide to grant them. Even if we do receive fast track designation or priority review, we may not experience a faster development process, review or approval compared to conventional FDA procedures. The FDA may withdraw fast track designation if it believes that the designation is no longer supported by data from our clinical development program.
Any breakthrough therapy designation granted by the FDA for our product candidate may not lead to a faster development or regulatory review or approval process, and it does not increase the likelihood that our product candidate will receive marketing approval.
We have applied for, and may in the future apply for, a breakthrough therapy designation of our product candidates for future indications. A breakthrough therapy is defined as a drug that is intended, alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or condition, and preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. For drugs and biologics that have been designated as breakthrough therapies, interaction and communication between the FDA and the sponsor of the trial can help to identify the most efficient path for clinical development while minimizing the number of patients placed in ineffective control regimens. Drugs designated as breakthrough therapies by the FDA may also be eligible for accelerated approval if the relevant criteria are met.
Designation of a product candidate as a breakthrough therapy is within the discretion of the FDA. Accordingly, even if we believe our product candidate meets the criteria for designation as a breakthrough therapy, the FDA may disagree and instead determine not to make such designation. In any event, the receipt of a breakthrough therapy designation for a product candidate may not result in a faster development process, review or approval compared to drugs considered for approval under conventional FDA procedures and does not assure ultimate approval by the FDA. In addition, even if one or more of our product candidates qualify as breakthrough therapies, the FDA may later decide that the products no longer meet the conditions for qualification or decide that the time period for FDA review or approval will not be shortened.
| 39 |
Third-party coverage and reimbursement and health care cost containment initiatives and treatment guidelines may constrain our future revenues.
Our ability to successfully market our drug candidates will depend in part on the level of reimbursement that government health administration authorities, private health coverage insurers and other organizations provide for the cost of our products and related treatments. Countries in which our drug candidates are expected to be sold through reimbursement schemes under national health insurance programs frequently require that manufacturers and sellers of pharmaceutical products obtain governmental approval of initial prices and any subsequent price increases. In certain countries, including the United States, government-funded and private medical care plans can exert significant indirect pressure on prices. We may not be able to sell our drug candidates profitably if adequate prices are not approved or coverage and reimbursement is unavailable or limited in scope. Increasingly, third-party payors attempt to contain health care costs in ways that are likely to impact our development of products including:
| ■ | failing to approve or challenging the prices charged for health care products; | |
| ■ | introducing reimportation schemes from lower priced jurisdictions; | |
| ■ | limiting both coverage and the amount of reimbursement for new therapeutic products; | |
| ■ | denying or limiting coverage for products that are approved by the regulatory agencies but are considered to be experimental or investigational by third-party payors; and | |
| ■ | refusing to provide coverage when an approved product is used in a way that has not received regulatory marketing approval. |
| 40 |
Risks Relating to Our Intellectual Property Rights
It is difficult and costly to protect our intellectual property rights, and we cannot ensure the protection of these rights.
Our commercial success will depend, in part, on maintaining and obtaining additional patent protection for our technologies, products and processes, successfully defending these patents against third-party challenges and successfully enforcing these patents against third party competitors. The patent positions of pharmaceutical companies can be highly uncertain and involve complex legal, scientific and factual questions for which important legal principles remain unresolved. Changes in either the patent laws or in interpretations of patent laws may diminish the value of our intellectual property. Accordingly, we cannot predict the breadth of claims that may be allowable in our pending applications or, the enforceability of our existing and future patents. Our pending patent applications for lenabasum and its uses may never be approved by United States or foreign patent offices and the existing patents and patent applications relating to lenabasum and related technologies may be challenged, invalidated or circumvented by third parties and may not protect us against competitors with similar products or technologies.
The degree of our current and future protection for our proprietary rights is uncertain, because legal means afford only limited protection and may not adequately protect our rights, permit us to gain or keep our competitive advantage, or provide us with any competitive advantage at all. For example, others have filed, and in the future are likely to file, patent applications covering products and technologies that are similar, identical or competitive to lenabasum, or important to our business. We cannot be certain that any patents or patent application owned by a third party will not have priority over patents and patent applications filed by us, or that we will not be involved in interference, opposition or invalidity proceedings before United States or foreign patent offices.
We also rely on trade secrets to protect technology, especially in cases when we believe patent protection is not appropriate or obtainable. However, trade secrets are difficult to protect. While we require employees, academic collaborators, consultants and other contractors to enter into confidentiality agreements, we may not be able to adequately protect our trade secrets or other proprietary or licensed information. Typically, research collaborators and scientific advisors have rights to publish data and information in which we may have rights. If we cannot maintain the confidentiality of our proprietary technology and other confidential information, our ability to receive patent protection and our ability to protect valuable information owned by us may be imperiled. Enforcing a claim that a third-party entity illegally obtained and is using any of our trade secrets is expensive and time consuming, and the outcome is unpredictable. In addition, courts are sometimes less willing to protect trade secrets than patents. Moreover, our competitors may independently develop equivalent knowledge, methods and know-how.
If we fail to maintain or obtain additional patent protection or trade secret protection for lenabasum or our technologies, third parties could use our proprietary information, which could impair our ability to compete in the market and adversely affect our ability to generate revenues and attain profitability.
We may also rely on the trademarks we may develop to distinguish our products from the products of our competitors. We cannot guarantee that any trademark applications filed by us or our business partners will be approved. Third parties may also oppose such trademark applications, or otherwise challenge our use of the trademarks. In the event that the trademarks we use are successfully challenged, we could be forced to rebrand our products, which could result in loss of brand recognition, and could require us to devote resources to advertising and marketing new brands. Further, we cannot provide assurance that competitors will not infringe the trademarks we use, or that we will have adequate resources to enforce these trademarks.
We have in-licensed a portion of our intellectual property, and if we fail to comply with our obligations under these arrangements, we could lose such intellectual property rights or owe damages to the licensor of such intellectual property.
We are a party to a license agreement with Jenrin pursuant to which we licensed the exclusive worldwide rights to develop, manufacture and market drug candidates from Jenrin. This agreement is important to our business, and we may enter into additional license agreements in the future. Certain of our in-licensed intellectual property covers, or may cover and potential cannabinoid developmental candidates. Our existing license agreement imposes, and we expect that future license agreements will impose, various diligence, milestone payment, royalty and other obligations on us. If there is any conflict, dispute, disagreement or issue of non-performance between us and our licensing partners regarding our rights or obligations under the license agreements, including any such conflict, dispute or disagreement arising from our failure to satisfy payment obligations under any such agreement, we may owe damages, our licensor may have a right to terminate the affected license, and our ability to utilize the affected intellectual property in our product discovery and development efforts and our ability to enter into collaboration or marketing agreements for an affected product candidate may be adversely affected.
| 41 |
Lenabasum and our other product candidates may infringe the intellectual property rights of others, which could increase our costs and delay or prevent our development and commercialization efforts.
Our success depends in part on avoiding infringement of the proprietary technologies of others. The pharmaceutical industry has been characterized by frequent litigation regarding patent and other intellectual property rights. Identification of third-party patent rights that may be relevant to our proprietary technology is difficult because patent searching is imperfect due to differences in terminology among patents, incomplete databases and the difficulty in assessing the meaning of patent claims. Additionally, because patent applications are maintained in secrecy until the application is published, we may be unaware of third-party patents that may be infringed by commercialization of lenabasum or any of our other product candidates. There may be certain issued patents and patent applications claiming subject matter that we may be required to license in order to research, develop or commercialize lenabasum or our other product candidates, and we do not know if such patents and patent applications would be available to license on commercially reasonable terms, or at all. Any claims of patent infringement asserted by third parties would be time-consuming and may:
| ■ | result in costly litigation; | |
| ■ | divert the time and attention of our technical personnel and management; | |
| ■ | prevent us from commercializing a product until the asserted patent expires or is held finally invalid or not infringed in a court of law; | |
| ■ | require us to cease or modify our use of the technology and/or develop non-infringing technology; or | |
| ■ | require us to enter into royalty or licensing agreements. |
Although no third party has asserted a claim of infringement against us, others may hold proprietary rights that could prevent our product candidates from being marketed. Any patent-related legal action against us claiming damages and seeking to enjoin commercial activities relating to our product candidates or our processes could subject us to potential liability for damages and require us to obtain a license to continue to manufacture or market lenabasum or any other product candidates. We cannot predict whether we would prevail in any such actions or that any license required under any of these patents would be made available on commercially acceptable terms, if at all. In addition, we cannot be sure that we could redesign lenabasum or any other product candidates or processes to avoid infringement, if necessary. Accordingly, an adverse determination in a judicial or administrative proceeding, or the failure to obtain necessary licenses, could prevent us from developing and commercializing lenabasum or another product candidate, which could harm our business, financial condition and operating results.
A number of companies, including several major pharmaceutical companies, have conducted research on anti-inflammatory and anti-fibrosis therapies which resulted in the filing of many patent applications related to this research. If we were to challenge the validity of these or any issued United States patent in court, we would need to overcome a statutory presumption of validity that attaches to every issued United States patent. This means that, in order to prevail, we would have to present clear and convincing evidence as to the invalidity of the patent’s claims.
If we were to challenge the validity of these or any issued United States patent in an administrative trial before the Patent Trial and Appeal Board in the United States Patent and Trademark Office, we would have to prove that the claims are unpatentable by a preponderance of the evidence. There is no assurance that a jury and/or court would find in our favor on questions of infringement, validity or enforceability.
We may be subject to claims that we have wrongfully hired an employee from a competitor or that we or our employees have wrongfully used or disclosed alleged confidential information or trade secrets of their former employers.
As is commonplace in our industry, we employ individuals who were previously employed at other pharmaceutical companies, including our competitors or potential competitors. Although no claims against us are currently pending, we may be subject in the future to claims that our employees or prospective employees are subject to a continuing obligation to their former employers (such as non-competition or non-solicitation obligations) or claims that our employees or we have inadvertently or otherwise used or disclosed trade secrets or other proprietary information of their former employers. Litigation may be necessary to defend against these claims. Even if we are successful in defending against these claims, litigation could result in substantial costs and be a distraction to management.
| 42 |
We may be subject to claims challenging the inventorship of our patents and other intellectual property.
Although we are not aware of any asserted third-party claims challenging inventorship on our patents or ownership of our intellectual property, we may in the future be subject to claims that former employees, strategic partners, commercial counterparties or other third parties associated with us or one of our predecessors in ownership of lenabasum have an interest in our patents or other intellectual property as an inventor or co-inventor. While it is our policy to require our employees and contractors who may be involved in the conception or development of intellectual property to execute agreements assigning such intellectual property to us, we cannot fully control the enforcement of these policies by third parties with which we contract, nor can we be certain that assignment agreements between us and our employees, between us and our counterparties, or between our counterparties and their employees or between our predecessors of ownership and their employees and counterparties, will effectively protect our interests as to any party who conceives or develops intellectual property that we regard as our own. Among other issues, the assignment of intellectual property rights may not be self-executing, the assignment agreements may be breached, or we may have disputes arise from conflicting obligations of consultants or others who are involved in developing our product candidates. As we approach potential commercialization of our product candidates, we are more closely analyzing all facts that we believe might be used to assert an inventorship claim against us. Determinations like these involve complex sets of fact and applications of sometimes-unsettled patent law, resulting in inherent uncertainties regarding ownership rights. Determining the history of development of certain of our intellectual property is made more difficult by the fact that certain of our intellectual property was developed by other companies for other indications before being acquired by us. Consequently, we cannot be sure that we have all of the documentary records relevant to such an analysis. In the course of our analysis we identified a potential issue regarding incomplete inventorship on certain aspects of our lenabasum portfolio that were developed prior to our acquisition of lenabasum. Since identifying this potential issue, we reached agreement with the relevant third-party co-inventors and received assignments of such co-inventors’ rights in and to the relevant patents.
If claims challenging inventorship are made against us, we may need to resort to litigation to resolve those claims. If we fail in defending against any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of valuable intellectual property rights or the right to assert those rights against third-parties marketing competing products. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
There are risks to our Intellectual Property based on our international business operations.
We may face risks to our technology and intellectual property as a result of our conducting business outside of the United States, including as a result of our license and collaboration agreement with Kaken, and particularly in jurisdictions that do not have comparable levels of protection of corporate proprietary information and assets such as intellectual property, trademarks, trade secrets, know-how and customer information and records. While these risks are common to many companies, conducting business in certain foreign jurisdictions, housing technology, data and intellectual property abroad, or licensing technology to joint ventures with foreign partners may have more significant exposure. Pursuant to our license and collaboration agreement with Kaken, we have granted Kaken an exclusive license to commercialize lenabasum in Japan, and an exclusive, worldwide license for the development and manufacturing of lenabasum in connection with Kaken’s commercialization efforts. As a result, and in the event Kaken partners with other companies in other foreign jurisdictions in connection with the development and manufacturing of lenabasum, we may be exposed to material risks of theft of our proprietary information and other intellectual property, including technical data, manufacturing processes, data sets or other sensitive information. For example, our products or components may be reverse engineered by other business partners or other parties, which could result in our patents being infringed or our know-how or trade secrets stolen. The risk can be by direct intrusion wherein technology and intellectual property is stolen or compromised through cyber intrusions or physical theft through corporate espionage, including with the assistance of insiders, or via more indirect routes.
| 43 |
General Company-Related Risks
We will need to grow the size of our organization, and we may experience difficulties in managing this growth.
As of December 31, 2020, we had 76 full-time employees. As our development and commercialization plans and strategies develop, we will need to expand the size of our employee base for managerial, operational, sales, marketing, financial and other resources. Future growth would impose significant added responsibilities on members of management, including the need to identify, recruit, maintain, motivate and integrate additional employees. In addition, our management may have to divert a disproportionate amount of its attention away from our day-to-day activities and devote a substantial amount of time to managing these growth activities. Our future financial performance and our ability to commercialize our drug candidates and our ability to compete effectively will depend, in part, on our ability to effectively manage our future growth.
Future capital raises may dilute our existing stockholders’ ownership and/or have other adverse effects on our operations.
If we raise additional capital by issuing equity securities, our existing stockholders’ percentage ownership will be reduced and these stockholders may experience substantial dilution. We may also issue equity securities that provide for rights, preferences and privileges senior to those of our common stock. If we raise additional funds by issuing debt securities, these debt securities would have rights senior to those of our common stock and the terms of the debt securities issued could impose significant restrictions on our operations, including liens on our assets. If we raise additional funds through collaborations and licensing arrangements, we may be required to relinquish some rights to our technologies or candidate products, or to grant licenses on terms that are not favorable to us.
| 44 |
If we are not successful in attracting and retaining highly qualified personnel, we may not be able to successfully implement our business strategy. In addition, the loss of the services of certain key employees, including Yuval Cohen, our Chief Executive Officer, Barbara White, our Chief Medical Officer, Craig Millian, our Chief Commercial Officer, and Sean Moran, our Chief Financial Officer would adversely impact our business prospects.
Our ability to compete in the highly competitive pharmaceuticals industry depends in large part upon our ability to attract highly qualified managerial, scientific and medical personnel. In order to induce valuable employees to remain with us, we intend to provide employees with stock options that vest over time. The value to employees of stock options that vest over time will be significantly affected by movements in the price of our common stock that we will not be able to control and may at any time be insufficient to counteract more lucrative offers from other companies.
Our management team has expertise in many different aspects of drug development and commercialization. However, we will need to hire additional personnel as we further develop our drug candidates. Competition for skilled personnel in our market is intense and competition for experienced scientists may limit our ability to hire and retain highly qualified personnel on acceptable terms. Despite our efforts to retain valuable employees, members of our management, scientific and medical teams may terminate their employment with us on short notice. We have entered into employment agreements with certain of our executive officers. However, these employment arrangements provide for at-will employment, which means that any of our employees could leave our employment at any time, with or without notice. The loss of the services of any of our executive officers or other key employees could potentially harm our business, operating results or financial condition. In particular, we believe that the loss of the services of Yuval Cohen, Ph.D., our Chief Executive Officer, Barbara White, M.D., our Chief Medical Officer, Craig Millian, our Chief Commercial Officer and Sean Moran, C.P.A., M.B.A., our Chief Financial Officer, would have a material adverse effect on our business. Our success also depends on our ability to continue to attract, retain and motivate highly skilled junior, mid-level, and senior managers as well as junior, mid-level, and senior scientific and medical personnel.
Other pharmaceutical companies with which we compete for qualified personnel have greater financial and other resources, different risk profiles, and a longer history in the industry than we do. They also may provide more diverse opportunities and better chances for career advancement. Some of these characteristics may be more appealing to high-quality candidates than what we have to offer. If we are unable to continue to attract and retain high-quality personnel, the rate and success at which we can develop and commercialize product candidates would be limited.
If product liability lawsuits are brought against us, we may incur substantial liabilities and may be required to limit commercialization of our drug candidates.
We face a potential risk of product liability as a result of the clinical testing of our drug candidates and will face an even greater risk if we commercialize our drug candidates. For example, we may be sued if any product we develop or any materials that we use in our products allegedly causes injury or is found to be otherwise unsuitable during product testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability and a breach of warranties. Claims could also be asserted under state consumer protection acts. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit commercialization of our drug candidates. Even successful defense would require significant financial and management resources. Regardless of the merits or eventual outcome, liability claims may result in:
| ● | decreased demand for our drug candidates; | |
| ● | injury to our reputation; | |
| ● | withdrawal of clinical trial participants; | |
| ● | costs to defend the related litigation; | |
| ● | a diversion of management’s time and our resources; | |
| ● | substantial monetary awards to trial participants or patients; | |
| ● | product recalls, withdrawals or labeling, marketing or promotional restrictions; | |
| ● | the inability to commercialize our drug candidates; and | |
| ● | a decline in the value of our stock. |
| 45 |
Our inability to obtain and retain sufficient product liability insurance at an acceptable cost to protect against potential product liability claims could prevent or inhibit the commercialization of products we develop. We intend to obtain product liability insurance covering our clinical trials. Although we will maintain such insurance, any claim that may be brought against us could result in a court judgment or settlement in an amount that is not covered, in whole or in part, by our insurance or that is in excess of the limits of our insurance coverage. Our insurance policies also have various exclusions, and we may be subject to a product liability claim for which we have no coverage. We may have to pay any amounts awarded by a court or negotiated in a settlement that exceed our coverage limitations or that are not covered by our insurance, and we may not have, or be able to obtain, sufficient capital to pay such amounts.
We may acquire businesses, assets or products, or form strategic alliances, in the future, and we may not realize the benefits of such acquisitions.
We may acquire additional businesses, assets or products, form strategic alliances or create joint ventures with third parties that we believe will complement or augment our existing business. If we acquire businesses with promising markets or technologies, we may not be able to realize the benefit of acquiring such businesses if we are unable to successfully integrate them with our existing operations and company culture. We may encounter numerous difficulties in developing, manufacturing and marketing any new delay or prevent us from realizing their expected benefits or enhancing our business. We cannot assure you that, following any such acquisition, we will achieve the expected synergies to justify the transaction.
Risks Related to our Common Stock
We will be unable to issue additional shares for future capital raising transactions or strategic transactions unless we obtain stockholder approval to amend our certificate of incorporation to increase the number of authorized shares of our common stock available for issuance.
We have 150,000,000 authorized shares of common stock. As of March 15, 2021, we have 125,033,006 shares of common stock outstanding and 23,370,094 shares of common stock reserved for future issuance related to stock options and warrants. As a result, as of March 15, 2021, we have approximately 90,694 shares of authorized shares of common stock available for future issuance. We will be limited by the number of additional shares available for future capital raising transactions or business development transactions unless we obtain stockholder approval of an amendment to our certificate of incorporation to increase the number of authorized shares of common stock. We plan to solicit the approval of our stockholders to amend our certificate of incorporation to increase the number of authorized shares of common stock, but we cannot be certain that our stockholders will approve the amendment. A delay in securing, or a failure to secure, stockholder approval to amend our certificate of incorporation could cause a delay in our future capital raising, collaboration, partnership or other strategic transactions, and may have a material adverse effect on our business and financial condition.
Our affiliates may control our company for the foreseeable future, including the outcome of matters requiring stockholder approval.
Our officers, directors, and five percent stockholders collectively owned approximately 20.2% of our outstanding shares of common stock as of December 31, 2020. This concentration of voting power and control could have a significant effect in delaying, deferring or preventing an action that might otherwise be beneficial to our other stockholders and be disadvantageous to our stockholders with interests different from those entities and individuals. Certain of these individuals also have significant control over our business, policies and affairs as officers or directors of our company. Therefore, you should not invest in reliance on your ability to have any control over our company.
An active, liquid trading market for our common stock may not be sustained.
Presently, our common stock is traded on the Nasdaq Global Market, or Nasdaq, and an investment in our company may require a long-term commitment, with no certainty of return. If we are unable to maintain an active, liquid active trading market:
| ● | investors may have difficulty buying and selling or obtaining market quotations; | |
| ● | market visibility for shares of our common stock may be limited; and | |
| ● | a lack of visibility for shares of our common stock may have a depressive effect on the market price for shares of our common stock. |
The lack of an active market could impair your ability to sell your shares at the time you wish to sell them or at a price that you consider reasonable. The lack of an active market may also reduce the fair market value of your shares. An inactive market may also impair our ability to raise capital to continue to fund operations by selling shares and may impair our ability to acquire additional intellectual property assets by using our shares as consideration.
| 46 |
We are currently listed on the Nasdaq Global Market. If we are unable to maintain listing of our securities on the Nasdaq Global Market or any stock exchange, our stock price could be adversely affected and the liquidity of our stock and our ability to obtain financing could be impaired and it may be more difficult for our stockholders to sell their securities.
Although our common stock is currently listed on the Nasdaq Global Market, we may not be able to continue to meet the exchange’s minimum listing requirements or those of any other national exchange. If we are unable to maintain listing on Nasdaq or if a liquid market for our common stock does not develop or is sustained, our common stock may remain thinly traded.
The Listing Rules of Nasdaq require listing issuers to comply with certain standards in order to remain listed on its exchange. If, for any reason, we should fail to maintain compliance with these listing standards and Nasdaq should delist our securities from trading on its exchange and we are unable to obtain listing on another national securities exchange, a reduction in some or all of the following may occur, each of which could have a material adverse effect on our stockholders:
| ● | the liquidity of our common stock; | |
| ● | the market price of our common stock; | |
| ● | our ability to obtain financing for the continuation of our operations; | |
| ● | the number of institutional and general investors that will consider investing in our common stock; | |
| ● | the number of investors in general that will consider investing in our common stock; | |
| ● | the number of market makers in our common stock; | |
| ● | the availability of information concerning the trading prices and volume of our common stock; and | |
| ● | the number of broker-dealers willing to execute trades in shares of our common stock. |
The market price of our common stock may be significantly volatile.
The market price for our common stock may be volatile and subject to wide fluctuations in response to factors including the following:
| ● | actual or anticipated fluctuations in our quarterly or annual operating results; | |
| ● | changes in financial or operational estimates or projections; | |
| ● | conditions in markets generally; | |
| ● | changes in the economic performance or market valuations of companies similar to ours; and | |
| ● | general economic or political conditions in the United States or elsewhere. |
In particular, the market prices of biotechnology companies like ours have been highly volatile due to factors, including, but not limited to:
| ● | any delay or failure to conduct a clinical trial for our product or receive approval from the FDA and other regulatory agencies; | |
| ● | developments or disputes concerning a company’s intellectual property rights; | |
| ● | technological innovations of such companies or their competitors; | |
| ● | changes in market valuations of similar companies; | |
| ● | announcements by such companies or their competitors of significant contracts, acquisitions, strategic partnerships, joint ventures, capital commitments, new technologies, or patents; and | |
| ● | failure to complete significant transactions or collaborate with vendors in manufacturing a product. |
The securities market has from time to time experienced significant price and volume fluctuations that are not related to the operating performance of particular companies. These market fluctuations may also materially and adversely affect the market price of shares of our common stock.
Future sales of shares by existing stockholders could cause our stock price to decline.
Sales of a substantial number of shares of our common stock in the public market could occur at any time. These sales, or the perception in the market that the holders of a large number of shares of common stock intend to sell shares, could reduce the market price of our common stock.
| 47 |
As of December 31, 2020, we had outstanding options to purchase an aggregate of 14,289,643 shares of our common stock at a weighted average exercise price of $5.15 per share and warrants to purchase an aggregate of 1,506,206 shares of our common stock at a weighted average exercise price of $9.46 per share. The exercise of such outstanding options and warrants will result in further dilution of your investment. If our existing stockholders sell substantial amounts of our common stock in the public market, or if the public perceives that such sales could occur, this could have an adverse impact on the market price of our common stock, even if there is no relationship between such sales and the performance of our business.
We do not currently intend to pay dividends on our common stock in the foreseeable future, and consequently, your ability to achieve a return on your investment will depend on appreciation in the price of our common stock.
We have never declared or paid cash dividends on our common stock and do not anticipate paying any cash dividends to holders of our common stock in the foreseeable future. Consequently, investors must rely on sales of their common stock after price appreciation, which may never occur, as the only way to realize any future gains on their investments. There is no guarantee that shares of our common stock will appreciate in value or even maintain the price at which our investors have purchased their shares.
There may be limitations on the effectiveness of our internal controls, and a failure of our control systems to prevent error or fraud may materially harm our company.
We are required, pursuant to Section 404 of the Sarbanes-Oxley Act, to furnish a report by our management on, among other things, the effectiveness of our internal control over financial reporting. This assessment will need to include disclosure of any material weaknesses identified by our management in our internal control over financial reporting. A material weakness is a deficiency, or combination of deficiencies, in internal control over financial reporting such that there is a reasonable possibility that a material misstatement of annual or interim financial statements will not be prevented or detected on a timely basis.
Effective internal control over financial reporting is necessary for us to provide reliable and timely financial reports and, together with adequate disclosure controls and procedures, are designed to reasonably detect and prevent fraud. Any failure to implement required new or improved controls, or difficulties encountered in their implementation could cause us to fail to meet our reporting obligations. Undetected material weaknesses in our internal control over financial reporting could lead to financial statement restatements and require us to incur the expense of remediation.
We do not expect that our disclosure controls or internal control over financial reporting will prevent or detect all error or all fraud. We may in the future discover weaknesses in our system of internal control over financial reporting that could result in a material misstatement of our financial statements. A control system, no matter how well designed and operated, can provide only reasonable, not absolute, assurance that the control system’s objectives will be met. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that misstatements due to error or fraud will not occur or that all control issues and instances of fraud will be detected. If we identify one or more material weaknesses in our internal controls, investors could lose confidence in the reliability of our financial statements, the market price of our stock could decline and we could be subject to sanctions or investigations by The Nasdaq Stock Market, the SEC or other regulatory authorities. Failure of our control systems to detect or prevent error or fraud could materially adversely impact us.
| 48 |
We may be unable to complete our analysis of our internal controls over financial reporting in a timely manner, or these internal controls may not be determined to be effective, which may adversely affect investor confidence in our company and, as a result, the value of our common stock.
We may not be able to complete our evaluation and testing of our internal control over financial reporting and any required remediation in a timely fashion. During the evaluation and testing process, if we identify one or more material weaknesses in our internal control over financial reporting, we will be unable to assert that our internal controls are effective.
If we are unable to assert that our internal control over financial reporting is effective, or, if applicable, our independent registered public accounting firm is unable to express an opinion on the effectiveness of our internal controls, we could lose investor confidence in the accuracy and completeness of our financial reports, which would cause the price of our common stock to decline, and we may be subject to investigation or sanctions by the SEC. We will also be required to disclose changes made in our internal control and procedures on a quarterly basis.
If we identify a material weakness, our remediation efforts may not enable us to avoid a material weakness in our internal control over financial reporting in the future. Any of the foregoing occurrences, should they come to pass, could negatively impact the public perception of our company, which could have a negative impact on our stock price.
Upon dissolution of our company, you may not recoup all or any portion of your investment.
In the event of a liquidation, dissolution or winding-up of our company, whether voluntary or involuntary, the proceeds and/or assets of our company remaining after giving effect to such transaction, and the payment of all of our debts and liabilities and distributions required to be made to holders of any outstanding preferred stock will then be distributed to the stockholders of common stock on a pro rata basis. There can be no assurance that we will have available assets to pay to the holders of common stock, or any amounts, upon such a liquidation, dissolution or winding-up of our Company. In this event, you could lose some or all of your investment.
Our ability to use our net operating loss carryforwards and certain other tax attributes may be limited.
We have incurred substantial losses during our history and do not expect to become profitable in the near future, and we may never achieve profitability. Unused federal net operating losses for tax years beginning before January 1, 2018 may be carried forward to offset future taxable income, if any, until such unused net operating losses expire. Under legislation enacted in 2017, informally titled the Tax Cuts and Jobs Act, or the Tax Act, as modified by legislation enacted on March 27, 2020, entitled the Coronavirus Aid, Relief, and Economic Security Act, or the CARES Act, federal net operating losses incurred in tax years beginning after December 31, 2017, can be carried forward indefinitely, but the deductibility of such federal net operating losses in tax years beginning after December 31, 2020 is limited to 80% of taxable income. In addition, as a result of our merger in April 2014 with Corbus Pharmaceuticals, Inc., our wholly-owned subsidiary, our ability to utilize our federal net operating loss, carryforwards and federal tax credit prior to that date may be limited under Sections 382 of the Internal Revenue Code. The limitations apply if an “ownership change,” as defined by Section 382, occurs. Generally, an ownership change occurs if the percentage of the value of the stock that is owned by one or more direct or indirect “five percent shareholders” increases by more than 50 percentage points over their lowest ownership percentage at any time during the applicable testing period (typically three years). In addition, future changes in our stock ownership, which may be outside of our control, may trigger an “ownership change” and, consequently, Section 382 limitations. As a result, if we earn net taxable income, our ability to use our pre-change net operating loss carryforwards and other tax attributes to offset United States federal taxable income may be subject to limitations, which could potentially result in increased future tax liability to us.
Legislation or other changes in U.S. tax law could adversely affect our business and financial condition.
The rules dealing with U.S. federal, state, and local income taxation are constantly under review by persons involved in the legislative process and by the Internal Revenue Service and the U.S. Treasury Department. Changes to tax laws (which changes may have retroactive application) could adversely affect us or holders of our common stock. In recent years, many changes have been made to applicable tax laws and changes are likely to continue to occur in the future. For example, the Tax Act, made significant changes to corporate taxation, including reduction of the corporate tax rate from a top marginal rate of 35% to a flat rate of 21%; limitation of the tax deduction for interest expense to 30% of adjusted earnings (except for certain small businesses); and, subject to certain changes in tax law made by the CARES Act as discussed above, limitation of the deduction of net operating losses generated in tax years beginning after December 31, 2017 to 80% of taxable income, indefinite carryforward of net operating losses generated in tax years after 2018 and elimination of net operating loss carrybacks generated in tax years ending after December 31, 2017; changes in the treatment of offshore earnings regardless of whether they are repatriated; current inclusion in U.S. federal taxable income of certain earnings of controlled foreign corporations, mandatory capitalization of research and development expenses beginning in 2022; immediate deductions for certain new investments instead of deductions for depreciation expense over time; further deduction limits on executive compensation; and modifying, repealing and creating many other business deductions and credits, including the reduction in the orphan drug credit from 50% to 25% of qualifying expenditures. We continue to examine the impact this tax reform legislation may have on our business. Notwithstanding the reduction in the corporate income tax rate, the overall impact of the Tax Act is uncertain and our business and financial condition could be adversely affected. The impact of this tax reform on holders of our common stock is also uncertain and could be adverse. This periodic report does not discuss any such tax legislation or the manner in which it might affect us or our stockholders in the future. We urge our stockholders to consult with their legal and tax advisors with respect to such legislation. In addition, the CARES Act included certain changes in tax law intended to stimulate the U.S. economy in light of the COVID-19 outbreak, including temporary beneficial changes to the treatment of net operating losses, interest deductibility limitations and payroll tax matters.
It cannot be predicted whether, when, in what form, or with what effective dates, new tax laws may be enacted, or regulations and rulings may be enacted, promulgated or issued under existing or new tax laws, which could result in an increase in our or our shareholders’ tax liability or require changes in the manner in which we operate in order to minimize or mitigate any adverse effects of changes in tax law or in the interpretation thereof.
| 49 |
Our certificate of incorporation, as amended, allows for our board to create new series of preferred stock without further approval by our stockholders, which could adversely affect the rights of the holders of our common stock.
Our board of directors has the authority to fix and determine the relative rights and preferences of preferred stock. We anticipate that our board of directors will have the authority to issue up to 10,000,000 shares of our preferred stock without further stockholder approval. As a result, our board of directors could authorize the issuance of a series of preferred stock that would grant to holders the preferred right to our assets upon liquidation and the right to receive dividend payments before dividends are distributed to the holders of common stock. In addition, our board of directors could authorize the issuance of a series of preferred stock that has greater voting power than our common stock or that is convertible into our common stock, which could decrease the relative voting power of our common stock or result in dilution to our existing stockholders.
| Item 1B. | UNRESOLVED STAFF COMMENTS |
Not applicable.
| Item 2. | PROPERTIES |
Our principal offices are located at 500 River Ridge Drive, Norwood, MA 02062 and consisted of 63,256 square feet of leased office space at December 31. 2020. The lease term for this office space ends on November 30, 2026.
| Item 3. | LEGAL PROCEEDINGS |
We are not currently subject to any material legal proceedings. However, we may from time to time become a party to various legal proceedings arising in the ordinary course of our business.
| Item 4. | MINE SAFETY DISCLOSURES |
Not applicable.
| 50 |
PART II
| Item 5. | MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES |
Market Information
Our common stock is currently listed on the Nasdaq Global Market under the symbol “CRBP.” Our shares of common stock began trading on the Nasdaq Capital Market under the symbol “CRBP” effective April 16, 2015.
Dividends
We have never declared or paid cash dividends on our common stock. We do not intend to declare or pay cash dividends on our common stock for the foreseeable future, but currently intend to retain any future earnings to fund the development and growth of our business. The payment of cash dividends if any, on the common stock will rest solely within the discretion of our board of directors and will depend, among other things, upon our earnings, capital requirements, financial condition, and other relevant factors.
Record Holders
As of March 8, 2021, there are approximately 85 record holders of shares of our common stock.
| Item 6. | SELECTED FINANCIAL DATA |
Not applicable.
| Item 7. | MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
The following discussion and analysis of our financial condition and results of operations should be read together with our financial statements and the related notes and the other financial information included elsewhere in this Annual Report. This discussion contains forward-looking statements that involve risks and uncertainties. Our actual results could differ materially from those anticipated in these forward-looking statements as a result of various factors, including those discussed below and elsewhere in this Annual Report, particularly those under “Risk Factors.”
Overview
We are a Phase 3, clinical-stage pharmaceutical company focused on the development and commercialization of novel therapeutics that target the endocannabinoid system in the fields of autoimmunity, fibrosis, and cancer. We are developing a diverse pipeline of drug candidates across several distinct programs, including small molecules as well as biologics, as well as evaluating potential external candidates complimentary to our existing programs.
| 51 |
Our pipeline includes the following programs:
| 1. | Lenabasum, a novel, synthetic, oral, CB2 agonist designed to resolve chronic inflammation, limit fibrosis and support tissue repair. Lenabasum is in clinical development for treatment of autoimmune diseases. We are currently evaluating lenabasum for safety and efficacy in a Phase 3 study in dermatomyositis, as well as a Phase 2 study in SLE”. | |
| 2. | Peripherally-restricted CB1 inverse agonists that are designed to normalize metabolic abnormalities or limit inflammation and fibrosis. We are currently evaluating these compounds in pre-clinical studies for the treatment of metabolic disorders and for fibrotic disorders. We are evaluating certain compounds as potential candidates for further clinical development. | |
| 3. | Novel CB2 agonists that are designed to limit cancer cell growth directly and reduce the fibrosis and immunosuppression in the tumor microenvironment that are associated with tumor growth, metastasis, and resistance to treatment with drugs such as checkpoint inhibitors. We are currently evaluating these compounds in pre-clinical studies for the treatment of cancer, in combination with other cancer therapies such as checkpoint inhibitors. We are evaluating certain compounds as potential candidates for further clinical development. |
Lenabasum selectively binds to CB2, which is preferentially expressed on activated immune cells, fibroblasts and other cell types, including muscle and bone cells. Lenabasum reduces inflammation and limits fibrosis, without immunosuppression. Lenabasum inhibits production of inflammatory cytokines and eicosanoids and stimulates the production of mediators (Specialized Pro-resolving Lipid Mediators) that resolve inflammation. It inhibits transformation of fibroblasts into myofibroblasts and production of fibrotic growth factors and collagen. These biologic effects have been demonstrated in cells, animal models, and humans.
The U.S. Food and Drug Administration, or FDA, has granted lenabasum Orphan Drug Designation as well as Fast Track Status for systemic sclerosis and cystic fibrosis, and Orphan Drug Designation for dermatomyositis. The European Medicines Authority, or EMA, has granted lenabasum Orphan Drug Designation for systemic sclerosis, cystic fibrosis, and dermatomyositis.
In 2020, we announced that lenabasum did not meet the primary endpoints in our RESOLVE-1 Phase 3 study of lenabasum for the treatment of systemic sclerosis or our Phase 2b study of lenabasum for the treatment of cystic fibrosis. Currently, no patients with systemic sclerosis or cystic fibrosis are being treated with lenabasum. We are preparing the data from our RESOLVE-1 Study for publication and will decide on the next steps in the development process for systemic sclerosis pending the outcome of our Phase 3 study of lenabasum for the treatment of dermatomyositis (the “DETERMINE Study”). We are preparing the data from our Phase 2b study of lenabasum for the treatment of cystic fibrosis for publication, but currently we do not have plans for additional clinical studies in cystic fibrosis.
In December 2018, we initiated the DETERMINE Study, our Phase 3 double-blind placebo-controlled multi-center international clinical study. The DETERMINE Study is fully enrolled with 176 patients. In January, 2021, we submitted a protocol amendment to the FDA to shorten the duration of the DETERMINE Study from 52 weeks to 28 weeks. Subjects in the DETERMINE Study are randomized to receive lenabasum 20 mg twice per day, lenabasum 5 mg twice per day, or placebo twice per day in a 2:1:2 ratio. The primary efficacy outcome, which will be measured at week 28, is the American College of Rheumatology/European League Against Rheumatism 2016 Total Improvement Score, which is a weighted composite measure of improvement from baseline in six endpoints, including Physician Global Assessment of Disease Activity, Physician Global Assessment of Extramuscular Disease Activity, Patient Global Assessment of Disease Activity, Health Assessment Questionnaire (patient-reported disability), Manual Muscle Testing, and muscle enzymes. Change from Baseline in the Cutaneous Dermatomyositis Activity and Severity index activity (CDASI) score is one of several secondary efficacy outcomes in the Phase 3 study. Last subject, last dose in the placebo-controlled part of the DETERMINE Study has been completed in the first fiscal quarter of 2021, with topline data expected in the second fiscal quarter of 2021.
Since our inception, we have devoted substantially all of our efforts to business planning, research and development, recruiting management and technical staff, acquiring operating assets and raising capital. Our research and development activities have included conducting pre-clinical studies, developing manufacturing methods and the manufacturing of our drug lenabasum for clinical trials and conducting clinical studies in patients.
In September 2018, pursuant to a license agreement (the ‘Jenrin Agreement”) with Jenrin Discovery LLC (“Jenrin”) we acquired an exclusive worldwide license to develop, manufacture and market drug candidates from more than 600 compounds targeting the endocannabinoid system. The portfolio of compounds includes cannabinoid candidates targeting liver, lung, heart and kidney fibrotic diseases.
On January 3, 2019, we entered into a strategic collaboration with Kaken Pharmaceutical Co., Ltd. (“Kaken”) for the development and commercialization in Japan of our investigational drug lenabasum for the treatment of systemic sclerosis and dermatomyositis. Under the terms of the agreement, Kaken receives an exclusive license to commercialize and market lenabasum in Japan for systemic sclerosis and dermatomyositis. In March 2019, Kaken made an upfront payment to us of $27 million. We are also eligible to receive up to $173 million upon achievement of certain regulatory, development and sales milestones as well as double- digit royalties from Kaken.
On January 30, 2019, we consummated an underwritten public offering of shares of our common stock pursuant to which we sold an aggregate of 6,198,500 shares of our common stock at a purchase price of $6.50 per share with gross proceeds to us totaling approximately $40.3 million, less estimated issuance costs incurred of approximately $2.6 million.
| 52 |
On February 11, 2020, we consummated an underwritten public offering of shares of our common stock pursuant to which we sold an aggregate of 7,666,667 shares of our common stock at a purchase price of $6.00 per share with gross proceeds to us totaling approximately $46.0 million, less estimated issuance costs incurred of approximately $3.0 million.
On April 7, 2020, we entered into an Open Market Sale AgreementSM (“April 2020 Sale Agreement”) with Jefferies LLC (“Jefferies”) pursuant to which Jefferies is serving as our sales agent to sell up to $75,000,000 of shares of the Company’s common stock through an “at the market offering”. As of December 31, 2020 we sold 10,539,374 shares of our common stock under the April 2020 Sale Agreement for gross proceeds to us totaling $75,000,000, less issuance costs incurred of approximately $2,250,000.
On July 28, 2020, we entered into the Loan Agreement with our subsidiary, Corbus Pharmaceuticals, Inc., as borrower, us, as guarantor, each lender party thereto (the “Lenders”), K2 HealthVentures LLC (“K2HV”), an unrelated third party, as administrative agent for the Lenders, and Ankura Trust Company, LLC, an unrelated third party, as collateral agent for the Lenders, pursuant to which K2HV may provide us with term loans in an aggregate principal amount of up to a $50,000,000.
On August 7, 2020, we entered into an Open Market Sale AgreementSM (the “August 2020 Sale Agreement”) with Jefferies, as sales agent, pursuant to which we may issue and sell, from time to time, through Jefferies, shares of our common stock. As of August 7, 2020, we are authorized to offer and sell up to $150 million of our common stock pursuant to the August 2020 Sale Agreement. As of December 31, 2020 we have sold 15,546,151 shares of our common stock under the August 2020 Sale Agreement for gross proceeds totaling $21,404,000, less issuance costs incurred of approximately $642,000.
We expect the cash and cash equivalents of approximately $85.4 million at December 31, 2020, $58.9 million of proceeds raised from the August 2020 Sale Agreement from January 1, 2021 through March 15, 2021, and the remaining $2.5 million of proceeds that we expect to receive under the 2018 CFF Award before the end of the first half of 2021 to be sufficient to meet our operating and capital requirements into 2024, based on planned expenditures.
Financial Operations Overview
We are a clinical stage pharmaceutical company and have not generated any revenues from the sale of products. We have never been profitable and at December 31, 2020, we had an accumulated deficit of approximately $304.1 million. Our net losses for the years ended December 31, 2020 and 2019 were approximately $111,269,000 and $71,454,000, respectively.
We expect to continue to incur significant expenses for the foreseeable future. We expect our expenses to decline in 2021 due to the completion of our clinical studies in systemic sclerosis and cystic fibrosis in 2020 and dermatomyositis in 2021. While we expect expenses to decline in 2021, we will still incur significant operating losses and accordingly we will need additional financing to support our continuing operations. We will seek to fund our operations through public or private equity or debt financings or other sources, which may include government grants and collaborations with third parties. Adequate additional financing may not be available to us on acceptable terms, or at all. Our failure to raise capital as and when needed would have a negative impact on our financial condition and our ability to pursue our business strategy. We will need to generate significant revenues to achieve profitability, and we may never do so.
We expect to continue to incur operating losses for at least the next several years in connection with our ongoing activities, as we:
| ● | conduct preclinical and clinical trials for our product candidates in DM, systemic lupus erythematosus and other indications; | |
| ● | continue our research and development efforts; and | |
| ● | manufacture clinical study materials. |
Critical Accounting Policies
Our consolidated financial statements have been prepared in accordance with accounting principles generally accepted in the United States of America (“GAAP”). The preparation of these financial statements requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period.
On an ongoing basis, we evaluate our estimates and judgments for all assets and liabilities, including those related to stock-based compensation expense. We base our estimates and judgments on historical experience, current economic and industry conditions and on various other factors that are believed to be reasonable under the circumstances. This forms the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions.
| 53 |
We believe that full consideration has been given to all relevant circumstances that we may be subject to, and the consolidated financial statements accurately reflect our best estimate of the results of operations, financial position and cash flows for the periods presented.
Revenue Recognition
Revenue from awards for the years ended December 31, 2020 and 2019 was approximately $3,937,000 and $9,144,000, respectively, and pertains only to the 2018 CFF Award. No revenue from licenses was recognized for the year ended December 31, 2020. Revenue from licenses for the year ended December 31, 2019 included the recognition of the $27,000,000 upfront payment received from Kaken in March 2019 for which we satisfied the combined performance obligation by June 30, 2019, upon which we recognized the $27,000,000 as revenue in the second quarter of 2019.
We will assess any new agreements we enter into under GAAP, including whether such agreements fall under the scope of such standard. This standard applies to all contracts with customers, except for contracts that are within the scope of other standards, such as leases, insurance, collaboration arrangements and financial instruments. Under GAAP, an entity recognizes revenue when its customer obtains control of promised goods or services, in an amount that reflects the consideration which the entity expects to receive in exchange for those goods or services. To determine revenue recognition for contracts with customers, the entity performs the following five steps: (i) identify the contract(s) with a customer; (ii) identify the performance obligations in the contract; (iii) determine the transaction price; (iv) allocate the transaction price to the performance obligations in the contract; and (v) recognize revenue when (or as) the entity satisfies a performance obligation. The five-step model is applied to contracts when it is probable that the entity will collect the consideration it is entitled to in exchange for the goods or services it transfers to the customer. At contract inception, we assess the goods or services promised within each contract and determine those that are performance obligations, and assess whether each promised good or service is distinct. We then recognize as revenue the amount of the transaction price that is allocated to the respective performance obligation when (or as) the performance obligation is satisfied.
Revenue associated with the performance obligation is being recognized as revenue as the research and development services are provided using an input method, according to the costs incurred as related to the research and development activities and the costs expected to be incurred in the future to satisfy the performance obligation. The transfer of control occurs over this time period and, in management’s judgment, is the best measure of progress towards satisfying the performance obligation. The research and development services related to this performance obligation are expected to be performed over an approximately three-year period expected to be completed in the first half of 2021. Amounts received prior to revenue recognition are recorded as deferred revenue. Amounts expected to be recognized as revenue within the 12 months following the balance sheet date are classified as current portion of deferred revenue in the accompanying consolidated balance sheets. Amounts not expected to be recognized as revenue within the 12 months following the balance sheet date are classified as deferred revenue, net of current portion. Amounts recognized as revenue, but not yet received or invoiced are generally recognized as contract assets.
| 54 |
Revenue
To date, we have not generated any revenues from the sales of products. We do not expect to generate revenue from product sales unless and until we successfully complete development and obtain regulatory approval for the marketing of lenabasum or other of our product candidates, which we expect will take a number of years and is subject to significant uncertainty.
We recognized approximately $3,937,000 and $9,144,000 of revenue from awards in the years ended December 31, 2020 and 2019, respectively.
Amounts recognized in revenue from awards for the years ended December 31, 2020 and 2019 were in connection with our entry on January 26, 2018 into the Cystic Fibrosis Program Related Investment Agreement (“Investment Agreement) with the Cystic Fibrosis Foundation (“CFF”), a non-profit drug discovery and development corporation, pursuant to which we received a development award for up to $25 million in funding (the “2018 CFF Award”) to support a Phase 2b Clinical Trial (the “Phase 2b Clinical Trial”) of lenabasum in patients with cystic fibrosis of which we received $6.25 million in the first quarter of 2018, $6.25 million in the second quarter of 2018, $5.0 million in the second quarter of 2019, and $5.0 million in the third quarter of 2020 upon our achievement of a milestone related to the progress of the Phase 2b Clinical Trial, as set forth in the Investment Agreement. The $2.5 million remainder of the 2018 CFF Award is payable to us incrementally upon the achievement of the remaining milestones related to the progress of the Phase 2b Clinical Trial, as set forth in the Investment Agreement and we expect to receive the remainder before the end of the first half of 2021.
Additionally, no revenue from licenses was recognized for the year ended December 31, 2020. Revenue from licenses for the year ended December 31, 2019 included the recognition of the $27,000,000 upfront payment received from Kaken in March 2019 for which we satisfied the combined performance obligation by June 30, 2019, upon which we recognized the $27,000,000 as revenue in the second quarter of 2019.
Research and Development
Research and development expenses are incurred for the development of lenabasum and other cannabinoid compounds and consist primarily of payroll and payments to contract research and development companies. To date, these costs are related to generating pre-clinical data and the cost of manufacturing drug product for clinical trials and conducting clinical trials. These costs are expected to decrease in 2021 as our RESOLVE-1 Study and our Phase 2b Study of lenabasum for the treatment of cystic fibrosis have completed. The reduction in workforce announced in October 2020 will also contribute to reduction of future operating expenses.
General and Administrative Expenses
General and administrative expenses consist primarily of payroll, rent and professional services such as accounting and legal services. We anticipate that our general and administrative expenses will decrease in the future as a result of the reduction in workforce announced in October 2020.
Other Income, Net
Other income, net consists primarily refundable research and development tax credits that were earned on certain research and development expenses we incurred primarily outside of the United States. Other income, net also consists of interest income we earn on interest-bearing accounts, interest expense incurred on our outstanding debt, and realized and unrealized foreign currency exchange gains and losses.
| 55 |
Critical Accounting Policies and Estimates
Our consolidated financial statements have been prepared in accordance with accounting principles generally accepted in the United States of America. The preparation of these financial statements requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period.
On an ongoing basis, we evaluate our estimates and judgments for all assets and liabilities, including those related to stock-based compensation expense, accrued research and development expense, and operating lease right of use assets and liabilities. We base our estimates and judgments on historical experience, current economic and industry conditions and on various other factors that are believed to be reasonable under the circumstances. This forms the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions.
We believe that full consideration has been given to all relevant circumstances that we may be subject to, and the consolidated financial statements accurately reflect our best estimate of the results of operations, financial position and cash flows for the periods presented.
Accrued Research and Development Expenses
As part of the process of preparing financial statements, we are required to estimate and accrue expenses, the largest of which are research and development expenses. This process involves: communicating with our applicable personnel to identify services that have been performed on our behalf and estimating the level of service performed and the associated cost incurred for the service when we have not yet been invoiced or otherwise notified of actual cost; estimating and accruing expenses in our financial statements as of each balance sheet date based on facts and circumstances known to us at the time; and periodically confirming the accuracy of our estimates with selected service providers and making adjustments, if necessary.
Examples of estimated research and development expenses that we accrue include:
| ● | fees paid to CROs in connection with nonclinical studies; | |
| ● | fees paid to contract manufacturers in connection with the production of lenabasum for clinical trials; | |
| ● | fees paid to CRO and research institutions in connection with conducting of clinical studies; and | |
| ● | professional service fees for consulting and related services. |
We base our expense accruals related to clinical studies on our estimates of the services performed pursuant to contracts with multiple research institutions and clinical research organizations that conduct and manage clinical studies on our behalf. The financial terms of these agreements vary from contract to contract and may result in uneven payment flows. Payments under some of these contracts depend on factors, such as the successful enrollment of patients and the completion of clinical study milestones. Our service providers invoice us monthly in arrears for services performed. In accruing service fees, we estimate the time period over which services will be performed and the level of effort to be expended in each period. If we do not identify costs that we have begun to incur or if we underestimate or overestimate the level of services performed or the costs of these services, our actual expenses could differ from our estimates.
To date, we have not experienced significant changes in our estimates of accrued research and development expenses following each applicable reporting period. However, due to the nature of estimates, we cannot assure you that we will not make changes to our estimates in the future as we become aware of additional information regarding the status or conduct of our clinical studies and other research activities.
| 56 |
Stock-Based Compensation
Stock options are granted with an exercise price at no less than fair market value at the date of the grant. The stock options normally expire ten years from the date of grant. Stock option awards vest upon terms determined by our board of directors.
We recognize compensation costs resulting from the issuance of stock-based awards to employees, members of our Board of directors and consultants. The fair value of each option grant was estimated as of the date of grant using the Black-Scholes option-pricing model. The fair value is amortized as compensation cost on a straight-line basis over the requisite service period of the awards, which is generally the vesting period. We estimate volatility by analyzing the volatility of the trading price of our common stock. We use historical data, as well as subsequent events occurring prior to the issuance of the consolidated financial statements, to estimate option exercise and employee forfeitures within the valuation model. The expected term of options granted to employees under our stock plans is based on the average of the contractual term (generally 10 years) and the vesting period (generally 48 months). The expected term of options granted under the 2014 Plan, all of which qualify as “plain vanilla” per SEC Staff Accounting Bulletin 107, is based on the average of the 6.25 years. For non-employee options, the expected term is the contractual term. The risk-free rate is based on the yield of a U.S. Treasury security with a term consistent with the option. We estimate the forfeiture rate at the time of grant and revise it, if necessary, in subsequent periods if actual forfeitures differ from those estimates. Forfeitures were estimated based on management’s expectation through industry knowledge and historical data. We have never paid dividends on our common stock and do not anticipate paying dividends on our common stock in the foreseeable future. Accordingly, we have assumed no dividend yield for purposes of estimating the fair value of our share-based compensation.
The following assumptions were used to estimate the fair value of stock options granted using the Black-Scholes option pricing model for the years ended December 31, 2020 and 2019 is as follows:
| 2020 | 2019 | |||||||
| Risk free interest rate | 0.59 | % | 2.33 | % | ||||
| Expected dividend yield | 0 | % | 0 | % | ||||
| Expected term in years | 6.25 | 6.25 | ||||||
| Expected volatility | 83.56 | % | 86.98 | % | ||||
| Estimated forfeiture rate | 6.02 | % | 4.85 | % | ||||
Results of Operations
Comparison of Year Ended 2020 to 2019
Revenue from Awards and Licenses. We have recognized approximately $3,937,000 and $36,144,000 of revenue from awards and licenses in the years ended December 31, 2020 and 2019, respectively.
Revenue from awards for the years ended December 31, 2020 and 2019 was approximately $3,937,000 and $9,144,000, respectively, recognized in accordance with ASC 606 and pertains only to the 2018 CFF Award. We received an aggregate of $12,500,000 during the year ended December 31, 2018 and an additional $5,000,000 during the year ended December 31, 2019, and $5,000,000 in the third quarter of 2020 upon our achievement of a milestone related to the progress of the Phase 2b Clinical Trial, as set forth in the Investment Agreement. The $2,500,000 remainder of the 2018 CFF Award is payable to us incrementally upon the achievement of the remaining milestones related to the progress of the Phase 2b Clinical Trial, as set forth in the Investment Agreement and we expect to receive the remainder before the end of the first half of 2021.
Revenue for the year ended December 31, 2019 also included the recognition of revenue from licenses for the $27,000,000 upfront payment received from Kaken in March 2019 for which we satisfied the combined performance obligation by June 30, 2019, upon which we recognized the $27,000,000 as revenue in the second quarter of 2019.
| 57 |
We assessed the 2018 CFF Award and the Kaken collaboration agreement for accounting under ASC 606. To determine revenue recognition for arrangements that an entity determines are within the scope of ASC 606, the entity performs the following five steps: (i) identify the contract(s) with a customer; (ii) identify the performance obligations in the contract; (iii) determine the transaction price; (iv) allocate the transaction price to the performance obligations in the contract; and (v) recognize revenue when (or as) the entity satisfies a performance obligation.
Research and Development. Research and development expenses for the year ended December 31, 2020 totaled approximately $98,267,000, an increase of $8,662,000 over the $89,605,000 recorded for the year ended December 31, 2019. The increase in fiscal 2020 as compared to fiscal 2019 was primarily attributable to increases of approximately $3,561,000 in clinical trial costs and $5,638,000 in compensation costs. These increases were partially offset by an approximate $537,000 decrease in stock-based compensation expense.
During 2018, the Company formed a subsidiary in each of the United Kingdom and Australia and approximately 44% and 46% of research and development expenses recorded for the year ended December 31, 2020 and December 31, 2019 respectively was recorded in these entities.
General and Administrative. General and Administrative expense for the year ended December 31, 2020 totaled approximately $28,480,000, an increase of $4,837,000 over the $23,643,000 recorded for the year ended December 31, 2019. The increase in fiscal 2020 as compared to fiscal 2019 was primarily attributable to increases of approximately $3,119,000 in compensation costs, $1,014,000 stock-based compensation, $473,000 in insurance costs, and $376,000 in temporary help and recruiting costs.
Other Income, Net. Other income, net for 2020 was approximately $11,541,000 as compared to approximately $5,651,000 recorded for 2019. The increase of $5,890,000 in 2020 as compared to 2019 was primarily attributable to approximately $9,574,000 increase in cash paid to us in 2020 from taxing authorities for refundable research and development tax credits that were earned on certain research and development expenses we incurred primarily outside of the United States, offset by $251,000 related to the derivative liability valuation associated with the Loan Agreement with K2HV and $850,000 related to a return of a state of Massachusetts research and development tax credit. In prior year we received approximately $472,000 for a refundable research and development tax credit and in 2020 approximately $378,000 became due back to the state of Massachusetts. The net increase was also offset by a $2,256,000 decrease to interest income. This was the result of approximately $1,100,000 lower interest income on excess cash and cash equivalents and $1,127,000 higher interest expense in 2020 as a result of entering into K2HV security and loan agreement.
Liquidity and Capital Resources
Since inception, we have experienced negative cash flows from operations. We have financed our operations primarily through sales of equity-related securities. In addition, the majority of the costs of the SLE clinical trial has been or is expected to be funded by NIH grants, and our phase 2b cystic fibrosis trial was supported by the 2018 CFF Award. At December 31, 2020, our accumulated deficit since inception was approximately $304,093,000.
At December 31, 2020, we had total current assets of approximately $92,075,000 and current liabilities of approximately $31,898,000 resulting in working capital of approximately $60,177,000. Of our total cash and cash equivalents of $85.4 million at December 31, 2020, $84.4 million was held within the United States.
Net cash used in operating activities for the year ended December 31, 2020 was approximately $99,686,000 which includes a net loss of approximately $111,269,000, adjusted for non-cash expenses of approximately $14,789,000, principally related to stock-based compensation expense of $12,458,000, depreciation and amortization expense of $1,124,000 and operating lease right of use asset amortization of $570,000, and approximately $3,205,000 of cash used by net working capital items, principally related to the decrease in accounts payable.
Cash used in investing activities for the year ended December 31, 2020 totaled approximately $484,000, which was largely related to payments for furniture and fixtures utilized in the build out of our office space in 2019.
| 58 |
Cash provided by financing activities for the year ended December 31, 2020 totaled approximately $154,875,000.
On February 11, 2020, we consummated an underwritten public offering of shares of our common stock pursuant to which we sold an aggregate of 7,666,667 shares of our common stock at a purchase price of $6.00 per share with gross proceeds to us totaling $46,000,000, less estimated issuance costs incurred of approximately $3,147,000.
During the year ended December 31, 2020 we sold an aggregate of 26,085,525 shares of our common stock under the April 2020 Sale Agreement and August 2020 Sale Agreement for gross proceeds of approximately $96,404,000, less issuance costs incurred of approximately $2,892,000.
On July 28, 2020, we entered into the Loan Agreement with K2HV pursuant to which K2HV may provide us with term loans in an aggregate principal amount of up to a $50,000,000 and we received the first tranche for $20,000,000 at closing. The second tranche for $20,000,000 and the third tranche for $10,000,000 will be made available at our option subject to the achievement of certain clinical and regulatory milestones. The loan matures on August 1, 2024 and we are obligated to make interest only payments for the first 24 months and then interest and equal principal payments for the next 24 months. Interest accrues at a variable annual rate equal to the greater of (i) 8.5% and (ii) the rate of interest noted in The Wall Street Journal, Money Rates section, as the “Prime Rate” plus 5.25%, in each case, subject to a step-down of 25 basis points upon the funding of the second tranche. K2HV may elect to convert up to $5,000,000 of the outstanding loan into common stock at a conversion price of $9.40 per share. At closing, we issued a Warrant to K2HV exercisable for 86,206 shares of the Company’s common stock at an exercise price of $6.96 per share. We granted registration rights to the lenders in connection with the Loan Agreement and the Warrant.
During the year ended December 31, 2020, we also received proceeds of approximately $756,000 from the issuance of 427,611 shares of our common stock upon the exercise of stock options to purchase common stock. Cash provided by financing activities for the year ended December 31, 2020 included proceeds from issuances of notes payable of approximately $909,000, offset by principal payments on notes payable of approximately $952,000 in connection with our loan agreements with financing companies to fund D&O insurance premiums. The terms of the loan that we entered into in November 2019 stipulated equal monthly payments of principal and interest payments of $109,413 over a nine-month period. Interest accrued on this loan at an annual rate of 5.25% and the loan was paid in full in August 2020. In November 2020, the Company entered into a loan agreement with a financing company for $909,375 to finance one of the Company’s insurance policies. The terms of the loan stipulate equal monthly payments of principal and interest payments of $103,112 over a nine-month period. Interest accrues on this loan at an annual rate of 4.89%.
We expect our cash and cash equivalents of approximately $85.4 million at December 31, 2020, combined with the $58.9 million of proceeds from the August 2020 Sale Agreement subsequent to December 31, 2020, and the expected final $2.5 million milestone payment from the CFF award will be sufficient to meet our operating and capital requirements into 2024 based on current planned expenditures.
We will need to raise significant additional capital to continue to fund operations and the clinical trials for lenabasum. If we are unable to raise sufficient capital in the future, we may be required to undertake cost-cutting measures, including delaying or discontinuing certain clinical activities. We may seek to sell common stock, preferred stock or convertible debt securities, enter into a credit facility or another form of third-party funding or seek other debt financing. In addition, we may seek to raise cash through collaborative agreements or from government grants. The sale of equity and convertible debt securities may result in dilution to our stockholders and certain of those securities may have rights senior to those of our common shares. If we raise additional funds through the issuance of preferred stock, convertible debt securities or other debt financing, these securities or other debt could contain covenants that would restrict our operations. Any other third-party funding arrangement could require us to relinquish valuable rights.
The source, timing and availability of any future financing will depend principally upon market conditions, and, more specifically, on the progress of our clinical development programs.
Funding may not be available when needed, at all, or on terms acceptable to us. Lack of necessary funds may require us, among other things, to delay, scale back or eliminate expenses including some or all of our planned clinical trials.
| 59 |
Contractual Obligations and Commitments
The following table presents information about our known contractual obligations as of December 31, 2020. It does not reflect contractual obligations that may have arisen or may arise after that date. Except for historical facts, the information in this section is forward-looking information.
| Payments due by period | ||||||||||||||||||||
| Contractual Obligations | Total | 2021 | 2022- 2023 | 2024- 2025 | After 2025 | |||||||||||||||
| Operating lease obligations | $ | 10,188,000 | $ | 1,605,000 | $ | 3,353,000 | $ | 3,542,000 | $ | 1,688,000 | ||||||||||
On February 26, 2019, we amended our lease (“February 2019 Lease Agreement”) pursuant to which an additional 30,023 square feet of office space (“New Premises”) will be leased by us in the same building for an aggregate total of 62,756 square feet of leased office space (“Total Premises”). The February 2019 Lease Agreement constitutes a modification as it extends the original lease term and increases the scope of the lease (additional space provided under the amendment), which requires evaluation of the remeasurement of the lease liability and corresponding right-of-use (“ROU”) asset. Accordingly, we reassessed the classification of the Leased Premises and remeasured the lease liability on the basis of the extended lease term using the 20 additional monthly rent payments and the incremental borrowing rate at the effective date of the modification of 9%. The remeasurement for the modification resulted in an increase to the lease liability and the ROU asset of approximately $855,000. We determined that the New Premises will be treated as a new standalone operating lease under U.S. GAAP and recorded a lease liability and a right-of-use asset of approximately $2.7 million for this lease.
Per the terms of the February 2019 Lease Agreement, the landlord agreed to reimburse us for $990,759 of leasehold improvements. The reimbursements are being recognized as a reduction of rent expense over the term of the lease. Additionally, the February 2019 Lease Agreement required a standby irrevocable letter of credit of $369,900, which may be reduced, if we are not in default under the February 2019 Lease Agreement, to $277,425 and $184,950 on the third and fourth anniversary of the commencement date, respectively.
On October 25, 2019, we amended our lease (“October 2019 Lease Amendment”) pursuant to which the term of the lease was extended through November 30, 2026 and the existing office space under lease was expanded by 500 square feet for an aggregate total of 63,256 square feet of leased office space (“Amended Total Premises”). The October 2019 Lease Amendment constitutes a modification as it extends the original lease term and increases the scope of the lease (additional space provided under the amendment), which requires evaluation of the remeasurement of the lease liability and corresponding ROU asset. The additional space did not result in a separate contract as the rent increase was determined not to be commensurate with the standalone price for the additional right of use. Accordingly, we reassessed the classification of the Amended Total Premises, which resulted in operating classification, and remeasured the lease liability on the basis of the extended lease term using the additional monthly rent payments and the incremental borrowing rate at the effective date of the modification of 8%. The remeasurement for the modification resulted in an increase to the lease liability and the ROU asset of approximately $381,000 that was recorded in the fourth quarter of 2019.
Pursuant to the terms of our non-cancelable lease agreements in effect at December 31, 2020, the following table summarizes our maturities of operating lease liabilities as of December 31, 2020:
| 2021 | $ | 1,605,121 | ||
| 2022 | 1,652,563 | |||
| 2023 | 1,700,005 | |||
| 2024 | 1,747,447 | |||
| 2025 | 1,794,889 | |||
| Thereafter | 1,688,145 | |||
| Total lease payments | $ | 10,188,170 | ||
| Less: imputed interest | (2,090,942 | ) | ||
| Total | $ | 8,097,228 |
We may enter into contracts in the normal course of business with clinical research organizations for clinical trials and clinical supply manufacturing and with vendors for pre-clinical research studies, research supplies and other services and products for operating purposes. These contracts generally provide for termination on notice, and therefore, we believe that our non-cancelable obligations under these agreements are not material. As of December 31, 2020, other than our leases in the table above, we had no material Contractual Obligations or Commitments that will affect our future liquidity.
Off-Balance Sheet Arrangements
We do not have any off-balance sheet arrangements that have or are reasonably likely to have a current or future effect on our financial condition, changes in financial condition, revenues or expenses, results of operations, liquidity, capital expenditures or capital resources that is material to investors, other than future royalty payments under development award agreements discussed as follows:
| 60 |
Collaboration Agreement with Kaken
Pursuant to the terms of the Kaken Agreement, we will bear the cost of, and be responsible for, among other things, conducting the clinical studies and other developmental activities for the Licensed Products in the Initial Indications in the Territory, and Kaken will bear the cost of, and be responsible for, among other things, preparing and filing applications for regulatory approval in the Territory and for commercializing Licensed Products in the Territory, and will use commercially reasonable efforts to commercialize Licensed Products and obtain pricing approval for Licensed Products in the Territory.
In consideration of the license and other rights granted by us, Kaken paid us a $27,000,000 upfront cash payment in March 2019 and is obligated to pay potential milestone payments to us totaling up to approximately $173,000,000 for the achievement of certain development, sales and regulatory milestones. In addition, during the Royalty Term (as defined below), Kaken is obligated to pay us royalties on sales of Licensed Products in the Territory, under certain conditions, in the double digits, which royalty shall be reduced in certain circumstances. In particular, for so long as we supply Licensed Products to Kaken pursuant to a supply agreement to be entered into by the parties, royalty payments shall be payable for each unit of Licensed Product that we supply as a percentage of the Japanese National Health Insurance price of the Licensed Product. During any time in which a supply agreement is not in effect, royalty payments shall be changed to a rate to be agreed upon by the parties in good faith.
The Kaken Agreement will remain in effect on a Licensed Product-by-Licensed product basis and will expire upon the expiration of the Royalty Term for the final Licensed Product. The “Royalty Term” means the period beginning on the date of the first commercial sale of the Licensed Product in Japan and ends on the latest of (i) the expiration of the last valid claim of the royalty patents covering such Licensed Product in Japan, (ii) the expiration of regulatory exclusivity for such Licensed Product for such Initial Indication in Japan, or (iii) ten (10) years after the first commercial sale of such Licensed Product for such Initial Indication in Japan. The Agreement may be terminated by either party for material breach, upon a party’s insolvency or bankruptcy or upon a challenge by one party of any patents of the other party, and Kaken may terminate in specified situations, including for a safety concern or clinical failure, or at its convenience following the second anniversary of the first commercial sale of a Licensed Product in either of the Initial Indications in the Territory, with 180 days’ notice.
License Agreement with Jenrin
Pursuant to the terms of the Jenrin Agreement, we are obligated to pay potential milestone payments to Jenrin totaling up to $18.4 million for each compound we elect to develop based upon the achievement of specified development and regulatory milestones. In addition, we are obligated to pay Jenrin royalties in the mid, single digits based on net sales of any Licensed Products, as defined in the Jenrin Agreement, subject to specified reductions.
The Jenrin Agreement terminates on a country-by-country basis and product-by-product basis upon the expiration of the royalty term for such product in such country. Each royalty term begins on the date of the first commercial sale of the licensed product in the applicable country and ends on the later of seven years from such first commercial sale or the expiration of the last to expire of the applicable patents in that country. The Jenrin Agreement may be terminated earlier in specified situations, including termination for uncured material breach of the Jenrin Agreement by either party, termination by Jenrin in specified circumstances, termination by Corbus with advance notice and termination upon a party’s insolvency or bankruptcy.
2018 CFF Award
Pursuant to the terms of the Investment Agreement, we are obligated to make certain royalty payments to CFF, including a royalty payment of one and one-half times the amount of the 2018 CFF Award, payable in cash within sixty days upon the first receipt of approval of lenabasum in the United States and a second royalty payment of one and one-half times the amount of the 2018 CFF Award upon approval in another major market, as set forth in the Investment Agreement (the “Approval Royalty”). At our election, we may satisfy the first of the two Approval Royalties in registered shares of our common stock. Additionally, we will owe to CFF a royalty payment equal to 10% of any amounts we receive as payment under the collaboration agreement with Kaken, provided that the total royalties that we will be required to pay under the Investment Agreement resulting from income from licenses or sales subject to the Investment Agreement are capped at five times the total amount of the 2018 CFF Award, and we may credit such royalties against any royalties on net sales otherwise owed to CFF under the Investment Agreement. Accordingly, we were required to pay CFF $2,700,000 in May 2019, which is within 60 days of our receipt of the $27,000,000 upfront cash payment from Kaken described below.
| 61 |
Additionally, we are obligated to make (i) royalty payments to CFF of two and one-half percent of net sales from lenabasum due within sixty days after any quarter in which such net sales occur in the Field, as defined in the Investment Agreement, (ii) royalty payments to CFF of one percent of net sales of Non-Field Products, as defined in the Investment Agreement due within sixty days after any quarter in which such net sales occur, and (iii) royalty payments to CFF of ten percent of any amount that we and our stockholders receive in connection with the license, sale, or other transfer to a third party of lenabasum, if indicated for the treatment or prevention of CF, or a change of control transaction, except that such payment shall not exceed five times the amount of the 2018 CFF Award, with such payments to be credited against any other net sales royalty payments due. Either CFF or we may terminate the Investment Agreement for cause, which includes our material failure to achieve certain commercialization and development milestones. Our payment obligations survive the termination of the Investment Agreement.
2015 CFFT Award
Pursuant to the terms of the 2015 CFFT Award agreement, we are obligated to make royalty payments to CFFT contingent upon commercialization of lenabasum in the Field of Use (as defined in the 2015 CFFT Award Agreement) as follows: (i) a royalty payment equal to five times the amount we receive under the 2015 CFFT Award Agreement, up to $25 million, payable in three equal annual installments following the first commercial sale of lenabasum, the first of which is due within 90 days following the first commercial sale of lenabasum, (ii) a royalty payment to CFFT equal to the amount we receive under the 2015 CFFT Award Agreement, up to $5 million, due in the first calendar year in which the aggregate cumulative net sales of lenabasum in the Field of Use exceed $500 million, and (iii) royalty payment(s) to CFFT of up to approximately $15 million if we transfer, sell or license lenabasum in the Field of Use other than for certain clinical or development purposes, or if we enter into a change of control transaction, with such payment(s) to be credited against the royalty payments due upon commercialization. The Field of Use is defined in the CFFT Award Agreement as the treatment in humans of CF, asbestosis, bronchiectasis, byssinosis, chronic bronchitis/COPD hypersensitivity pneumonitis, pneumoconiosis, primary ciliary dyskinesis, sarcoidosis and silicosis. Either CFFT or we may terminate the 2015 CFFT Award Agreement for cause, which includes our material failure to achieve certain commercialization and development milestones. Our payment obligations, if any, would survive the termination of the 2015 CFFT Award Agreement.
| Item 7A. | QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK |
Our exposure to market risk is limited to our cash and cash equivalents, all of which have maturities of three months or less. The primary objectives of our investment activities are to preserve principal, provide liquidity and maximize income without significantly increasing risk. Our primary exposure to market risk is interest income sensitivity, which is affected by changes in the general level of U.S. interest rates. However, because of the short-term nature of the instruments in our portfolio, a sudden change in market interest rates would not be expected to have a material impact on our financial condition and/or results of operation.
Foreign Exchange Risk
The majority of our operations are based in the United States and, accordingly our transactions are denominated in U.S. Dollars. However, we have foreign currency exposures related to our cash valued in the United Kingdom in British Pounds and Euros and our cash valued in Australia in Australian Dollars because our functional currency is the U.S. Dollar in our foreign-based subsidiaries. Our foreign denominated assets and liabilities are remeasured each reporting period with any exchange gains and losses recorded in our consolidated statements of operations.
| 62 |
| Item 8. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA |
See pages F-1 through F-23 following the Exhibit Index of this Annual Report on Form 10-K.
| Item 9. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
None.
| Item 9A. | CONTROLS AND PROCEDURES |
Evaluation of Our Disclosure Controls
We maintain disclosure controls and procedures that are designed to ensure that information required to be disclosed in the reports that we file or submit under the Securities and Exchange Act of 1934 as amended (the “Exchange Act”) is (1) recorded, processed, summarized, and reported within the time periods specified in the SEC’s rules and forms and (2) accumulated and communicated to our management, including our principal executive officer and our principal financial officer, or persons performing similar functions, to allow timely decisions regarding required disclosure.
As of December 31, 2020, our management, with the participation of our principal executive officer and principal financial officer, evaluated the effectiveness of our disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) of the Exchange Act). Our management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives, and management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Our principal executive officer and principal financial officer have concluded, based upon the evaluation described above, that our disclosure controls and procedures were effective as of December 31, 2020.
Management’s Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal controls over financial reporting, as such term is defined in Rule 13a-15(f) of the Exchange Act .
Our management conducted an assessment of the effectiveness of our internal control over financial reporting based on the criteria set forth in the “Internal Control-Integrated Framework (2013)” issued by the Committee of Sponsoring Organization of the Treadway Commission. Based on this assessment, management concluded that, as of December 31, 2020, our internal control over financial reporting was effective.
This annual report does not include an attestation report of our registered public accounting firm on internal control over financial reporting.
Remediation of Previously Reported Material Weaknesses
The material weaknesses related to our control environment and our information technology general controls governing user access over certain information technology (“IT”) systems that were previously reported in Item 9A of our Annual Report on Form 10-K for the fiscal year ended December 31, 2019 were remediated during our fiscal year ended December 31, 2020, and we determined that we maintained effective internal controls over our financial reporting as of December 31, 2020.
Management took significant steps to remediate the control deficiencies that led to the material weaknesses. We added experienced accounting personnel to our finance staff, implemented software to assist in monitoring internal controls and engaged an outside consulting firm to help us evaluate and test our internal controls. We successfully redesigned our IT control environment related to permissions and access to software applications and our financial control environment associated with the accrual of costs from research and development contracts.
Changes in Internal Controls over Financial Reporting
Other than the changes described above, there were no other changes in our internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f)) under the Exchange Act) that occurred during the fourth quarter ended December 31, 2020, that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
| Item 9B. | OTHER INFORMATION |
None
| 63 |
PART III
| Item 10. | DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE |
Information required by this item is incorporated by reference to our Proxy Statement for the 2021 Annual Meeting of Stockholders.
| Item 11. | EXECUTIVE COMPENSATION |
Information required by this item is incorporated herein by reference to our Proxy Statement for the 2021 Annual Meeting of Stockholders.
| Item 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
Information required by this item is incorporated by reference to our Proxy Statement for the 2021 Annual Meeting of Stockholders.
| Item 13. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
Information required by this item is incorporated by reference to our Proxy Statement for the 2021 Annual Meeting of Stockholders.
| Item 14. | PRINCIPAL ACCOUNTING FEES AND SERVICES |
Information required by this item is incorporated by reference to our Proxy Statement for the 2021 Annual Meeting of Stockholders.
| 64 |
PART IV
| Item 15. | EXHIBITS, FINANCIAL STATEMENT SCHEDULES |
(a) List of Documents filed as part of this Report
(1) Consolidated Financial Statements
The financial statements and related notes, together with the report of EisnerAmper LLP appear at pages F-1 through F-23 following the Exhibit List as required by Part II, Item 8 “Financial Statements and Supplementary Data” of this Form 10-K.
(2) Financial Statement Schedules.
Schedules are omitted because they are either not required, not applicable, or the information is otherwise included.
(3) Exhibits
The Company has filed with this report or incorporated by reference herein certain exhibits as specified below pursuant to Rule 12b-32 under the Exchange Act. See Exhibit Index following the signature page to this report for a complete list of documents filed with this report.
| 65 |
| 66 |
| 67 |
| 21.1 | List of Subsidiaries of the Company.* | |
| 23.1 | Consent of EisnerAmper LLP.* | |
| 31.1 | Certification of Chief Executive Officer pursuant to Rule 13a-14(a) or Rule 15d-14(a).* | |
| 31.2 | Certification of Chief Financial Officer pursuant to Rule 13a-14(a) or Rule 15d-14(a).* | |
| 32.1 | Certification of Chief Executive Officer pursuant to Rule 13a-14(b) or Rule 15d-14(b).** | |
| 32.2 | Certification of Chief Financial Officer pursuant to Rule 13a-14(b) or Rule 15d-14(b).** | |
| 101.INS | XBRL Instance Document.* – the instance document does not appear in the Interactive Data File because its XBRL tags are embedded within the Inline XBRL document. | |
| 101.SCH | XBRL Taxonomy Extension Schema Document.* | |
| 101.CAL | XBRL Taxonomy Extension Calculation Linkbase Document.* | |
| 101.DEF | XBRL Taxonomy Extension Definition Linkbase Document.* | |
| 101.LAB | XBRL Taxonomy Extension Label Linkbase Document.* | |
| 101.PRE | XBRL Taxonomy Extension Presentation Linkbase Document.* | |
| 104 | The cover page from the Company’s Annual Report on Form 10-K for the year ended December 31, 2020, has been formatted in Inline XBRL* |
| * | Filed herewith. |
| ** | Furnished, not filed. |
| # | Confidential treatment has been granted with respect to certain portions of this exhibit. Omitted portions have been submitted separately to the SEC. |
| † | Indicates a management contract or compensation plan, contract or arrangement. |
| Item 16. | FORM 10-K SUMMARY |
None.
| 68 |
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| CORBUS PHARMACEUTICALS HOLDINGS, INC. | ||
| Date: March 15, 2021 | By: | /s/ YUVAL COHEN |
| Name: | Yuval Cohen | |
| Title: | Chief Executive Officer | |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| Signature | Title | Date | ||
| /s/ YUVAL COHEN | Chief Executive Officer and Director (Principal Executive Officer) |
March 15, 2021 | ||
| Yuval Cohen | ||||
| /s/ SEAN MORAN | Chief Financial Officer (Principal Financial and Accounting Officer) | March 15, 2021 | ||
| Sean Moran | ||||
| /s/ ALAN HOLMER | Director | March 15, 2021 | ||
| Alan Holmer | ||||
| /s/ JOHN JENKINS | Director | March 15, 2021 | ||
| John Jenkins | ||||
| /s/ AVERY CATLIN | Director | March 15, 2021 | ||
| Avery Catlin | ||||
| /s/ RACHELLE JACQUES | Director | March 15, 2021 | ||
| Rachelle Jacques | ||||
| /s/ PETER SALZMANN | Director | March 15, 2021 | ||
| Peter Salzmann |
| 69 |
INDEX TO FINANCIAL STATEMENTS
| Page Number | ||
| Report of Independent Registered Public Accounting Firm | F-2 | |
| Corbus Pharmaceuticals Holdings, Inc. Financial Statements-December 31, 2020: | ||
| Consolidated Balance Sheets as of December 31, 2020 and December 31, 2019 | F-3 | |
| Consolidated Statements of Operations for the Years Ended December 31, 2020 and 2019 | F-4 | |
| Consolidated Statements of Stockholders’ Equity for the Years Ended December 31, 2020 and 2019 | F-5 | |
| Consolidated Statements of Cash Flows for the Years Ended December 31,2020 and 2019 | F-6 | |
| Notes to Consolidated Financial Statements | F-7 |
| F-1 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders of
Corbus Pharmaceuticals Holdings, Inc. and Subsidiaries
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Corbus Pharmaceuticals Holdings, Inc. and Subsidiaries (the “Company”) as of December 31, 2020 and 2019, and the related consolidated statements of operations, stockholders’ equity, and cash flows for each of the years then ended, and the related notes (collectively referred to as the “financial statements”). In our opinion, the financial statements present fairly, in all material respects, the consolidated financial position of the Company as of December 31, 2020 and 2019, and the consolidated results of their operations and their cash flows of the years then ended, in conformity with accounting principles generally accepted in the United States of America.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (“PCAOB”) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matter
The critical audit matter communicated below is a matter arising from the current period audit of the financial statements that was communicated or required to be communicated to the audit committee and that: (1) relates to accounts or disclosures that are material to the financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of the critical audit matter does not alter in any way our opinion on the financial statements, taken as a whole, and we are not, by communicating the critical audit matter below, providing separate opinions on the critical audit matter or on the accounts or disclosures to which it relates.
Accruals for Research and Development Expenses and Clinical Trials
As described in Note 3 to the consolidated financial statements, at each balance sheet date the Company estimates its accrued clinical expenses resulting from its obligations under contracts with vendors, clinical research organizations and consultants and under clinical site agreements in connection with conducting clinical trials, and may depend on factors such as successful enrollment of certain numbers of patients, site initiation, and the completion of clinical trial milestones. The Company accounts for trial expenses based on services that have been performed on the Company’s behalf and estimating the level of service performed and the associated cost incurred for the service when an invoice has not been received or the Company has not otherwise been notified of the actual cost. The Company estimates the time period over which services will be performed and the level of effort to be expended in each period. The Company’s accrual for clinical trial expenses of $16,322,000 is included in Accrued expenses on the December 31, 2020 consolidated balance sheet. The amounts recorded for clinical trial expenses represent the Company’s estimate of the unpaid clinical trial expenses based on the information available to the Company at that time. The estimation of clinical trial expenses was also identified as a critical accounting estimate by management.
We identified the accruals for research and development expenses and clinical trials as a critical audit matter due to the significant judgment and estimation required by management in determining progress or state of completion of trials or services completed. This in turn led to a high degree of auditor subjectivity and significant audit effort was required in performing our procedures and evaluating audit evidence relating to estimates made by management.
Addressing the matter involved performing procedures and evaluating audit evidence in connection with forming our overall opinion on the financial statements. We obtained an understanding and evaluated the design of controls over the Company’s estimation of clinical trial expenses, including the process of estimating the expenses incurred to date based on the status of the clinical trials. Our procedures also included, among others, reading agreements and contract amendment with vendors in connection with conducting clinical trials, and evaluating the significant assumptions described above and the methods used in developing the clinical trial estimates and calculating the amounts that were unpaid at the balance sheet date. We confirmed the assumptions directly with the third parties involved in performing the clinical trial services on behalf of the Company. We also made direct inquiries of financial and clinical client personnel regarding status and progress to completion of clinical trials and description of future commitments, and verified amounts paid to date under each contract by vouching to invoices and payment support. We also assessed the historical accuracy of management’s estimates, and compared the current estimate of expenses incurred to estimates previously made by management.
/s/ EisnerAmper LLP
We have served as the Company’s auditor since 2014.
EISNERAMPER LLP
Philadelphia, Pennsylvania
March 15, 2021
| F-2 |
Corbus Pharmaceuticals Holdings, Inc.
Consolidated Balance Sheets
| December 31, 2020 | December 31, 2019 | |||||||
| ASSETS | ||||||||
| Current assets: | ||||||||
| Cash and cash equivalents | $ | $ | ||||||
| Restricted cash | ||||||||
| Stock Subscriptions Receivable | ||||||||
| Prepaid expenses and other current assets | ||||||||
| Contract asset | ||||||||
| Total current assets | ||||||||
| Restricted cash | ||||||||
| Property and equipment, net | ||||||||
| Operating lease right of use assets | ||||||||
| Other assets | ||||||||
| Total assets | $ | $ | ||||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY | ||||||||
| Current liabilities: | ||||||||
| Notes payable | $ | $ | ||||||
| Accounts payable | ||||||||
| Accrued expenses | ||||||||
| Derivative liability | ||||||||
| Operating lease liabilities, current | ||||||||
| Total current liabilities | ||||||||
| Long-term debt, net of debt discount | ||||||||
| Operating lease liabilities, noncurrent | ||||||||
| Total liabilities | $ | $ | ||||||
| Stockholders’ equity | ||||||||
| Preferred stock, $ par value; shares authorized, shares issued and outstanding at December 31, 2020 and 2019 | ||||||||
| Common stock, $ par value; shares authorized, and shares issued and outstanding at December 31, 2020 and 2019, respectively | ||||||||
| Additional paid-in capital | ||||||||
| Accumulated deficit | ( | ) | ( | ) | ||||
| Total stockholders’ equity | ||||||||
| Total liabilities and stockholders’ equity | $ | $ | ||||||
The accompanying notes are an integral part of these Consolidated Financial Statements.
| F-3 |
Corbus Pharmaceuticals Holdings, Inc.
Consolidated Statements of Operations
For the Years Ended December 31, | ||||||||
| 2020 | 2019 | |||||||
| Revenue from awards and licenses | $ | $ | ||||||
| Operating expenses: | ||||||||
| Research and development | ||||||||
| General and administrative | ||||||||
| Total operating expenses | ||||||||
| Operating loss | ( | ) | ( | ) | ||||
| Other income (expense), net: | ||||||||
| Other income (expense), net | ||||||||
| Interest income (expense), net | ( | ) | ||||||
| Change in fair value of derivative liability | ( | ) | ||||||
| Foreign currency exchange gain (loss) | ( | ) | ( | ) | ||||
| Other income, net | ||||||||
| Net loss | $ | ( | ) | $ | ( | ) | ||
| Net loss per share, basic and diluted | $ | ( | ) | $ | ( | ) | ||
| Weighted average number of common shares outstanding, basic and diluted | ||||||||
The accompanying notes are an integral part of these Consolidated Financial Statements.
| F-4 |
Corbus Pharmaceuticals Holdings, Inc.
Consolidated Statements of Stockholders’ Equity
| Common Stock | Additional Paid-in | Accumulated | Total Stockholders’ | |||||||||||||||||
| Shares | Amount | Capital | Deficit | Equity | ||||||||||||||||
| Balance at December 31, 2018 | $ | $ | $ | ( | ) | $ | ||||||||||||||
| Stock-based compensation expense | — | |||||||||||||||||||
| Issuance of common stock, net of issuance costs of $ | ||||||||||||||||||||
| Issuance of common stock upon exercise of stock options | ||||||||||||||||||||
| Issuance of common stock upon exercise of warrants | ( | ) | ||||||||||||||||||
| Net Loss | ( | ) | ( | ) | ||||||||||||||||
| Balance at December 31, 2019 | $ | $ | $ | ( | ) | $ | ||||||||||||||
| Stock-based compensation expense | — | |||||||||||||||||||
| Issuance of common stock, net of issuance costs of $ | ||||||||||||||||||||
| Issuance of common stock upon exercise of stock options | ||||||||||||||||||||
| Fair value of warrants issued | — | |||||||||||||||||||
| Net Loss | ( | ) | ( | ) | ||||||||||||||||
| Balance at December 31, 2020 | $ | $ | $ | ( | ) | $ | ||||||||||||||
The accompanying notes are an integral part of these Consolidated Financial Statements.
| F-5 |
Corbus Pharmaceuticals Holdings, Inc.
Consolidated Statements of Cash Flows
| 2020 | 2019 | |||||||
| Cash flows from operating activities: | ||||||||
| Net loss | $ | ( | ) | $ | ( | ) | ||
| Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||
| Stock-based compensation expense | ||||||||
| Depreciation and amortization | ||||||||
| Loss on foreign exchange | ||||||||
| Operating lease right of use asset amortization | ||||||||
| Amortization of debt discount | ||||||||
| Change in fair value of derivative liability | ||||||||
| Changes in operating assets and liabilities: | ||||||||
| Decrease in customer receivable | ||||||||
| Decrease (increase) in prepaid expenses | ( | ) | ||||||
| Decrease (increase) contract asset | ( | ) | ||||||
| Increase in other assets | ( | ) | ( | ) | ||||
| Increase (decrease) in accounts payable | ( | ) | ||||||
| Increase (decrease) in accrued expenses | ( | ) | ||||||
| Decrease in deferred revenue | ( | ) | ||||||
| Increase (decrease) in operating lease liabilities | ( | ) | ||||||
| Net cash used in operating activities | ( | ) | ( | ) | ||||
| Cash flows from investing activities: | ||||||||
| Purchases of property and equipment | ( | ) | ( | ) | ||||
| Net cash used in investing activities | ( | ) | ( | ) | ||||
| Cash flows from financing activities: | ||||||||
| Proceeds from issuance of short-term borrowings | ||||||||
| Proceeds from issuance of long-term borrowings | ||||||||
| Repayment of short-term borrowings | ( | ) | ( | ) | ||||
| Proceeds from issuance of common stock | ||||||||
| Issuance costs paid for common stock financings | ( | ) | ( | ) | ||||
| Principal payments under capital lease obligations | ( | ) | ||||||
| Net cash provided by financing activities | ||||||||
| Net increase (decrease) in cash, cash equivalents, and restricted cash | ( | ) | ||||||
| Cash, cash equivalents, and restricted cash at beginning of the year | ||||||||
| Cash, cash equivalents and restricted cash at end of the year | $ | |||||||
| Supplemental disclosure of cash flow information and non cash transactions: | ||||||||
| Cash paid during the period for interest | $ | |||||||
| Fair value of warrants issued in loan agreement | ||||||||
| Fair value of warrants issued | ||||||||
| Write-off of fully depreciated property and equipment | ||||||||
| Purchases of property and equipment included in accounts payable or accrued expenses | ||||||||
| Right of use assets obtained in exchange for lease obligation upon adoption of ASU 2016-02, net of deferred rent | ||||||||
| Right of use assets obtained in exchange for lease obligation upon entry into lease agreements | ||||||||
| Stock subscription receivable | ||||||||
The accompanying notes are an integral part of these Consolidated Financial Statements.
| F-6 |
Corbus Pharmaceuticals Holdings, Inc.
Notes to Consolidated Financial Statements
December 31, 2020 and 2019
| 1. | NATURE OF OPERATIONS |
Business
Corbus Pharmaceuticals Holdings, Inc. (“the Company” or “Corbus”) is a clinical-stage pharmaceutical company focused on the development and commercialization of novel therapeutics that target the endocannabinoid or immune system. The Company intends to pursue indications for our novel therapeutics that are autoimmune, fibrotic, or metabolic diseases, or cancer. The Company is developing a diverse pipeline of drug candidates and plan to expand our pipeline through internal efforts and business development. Since its inception, the Company has devoted substantially all of its efforts to business planning, research and development, recruiting management and technical staff, acquiring operating assets and raising capital. The Company’s business is subject to significant risks and uncertainties and the Company will be dependent on raising substantial additional capital before it becomes profitable and it may never achieve profitability.
In response to the spread of COVID-19, the Company has taken temporary precautionary measures intended to help minimize the risk of the virus to its employees and community, including temporarily requiring employees to work remotely, implementing remote monitoring procedures for clinical data and suspending all non-essential travel worldwide for its employees.
The Company is continuing to monitor the impact of the COVID-19 pandemic on its business and operations.
| 2. | LIQUIDITY |
The
accompanying consolidated financial statements have been prepared assuming the Company will continue as a going concern, which
contemplates continuity of operations, realization of assets and the satisfaction of liabilities and commitments in the normal
course of business. The Company has incurred recurring losses since inception and as of December 31, 2020, had an accumulated
deficit of $
The source, timing and availability of any future financing will depend principally upon market conditions, and, more specifically, on the progress of the Company’s clinical development programs.
On February 11, 2020, the Company consummated an underwritten public offering of shares of its common stock (“February 2020 Offering”) (See Note 11).
On
April 7, 2020, the Company entered into an Open Market Sale AgreementSM (“April 2020 Sale Agreement”) with
Jefferies LLC (“Jefferies”) pursuant to which Jefferies is serving as the Company’s sales agent to sell up to
$ of shares of the Company’s common stock through an “at the market offering”. During the year ended
December 31, 2020, the Company sold shares of its common stock under the April 2020 Sale Agreement for which the Company
received gross proceeds of approximately $
In
June 2020, the Company became entitled to receive $
On
July 28, 2020, the Company entered into the Loan Agreement with its subsidiary, Corbus Pharmaceuticals, Inc., as borrower, the
Company, as guarantor, each lender party thereto (the “Lenders”), K2 HealthVentures LLC (“K2HV”), an unrelated
third party, as administrative agent for the Lenders, and Ankura Trust Company, LLC, an unrelated third party, as collateral agent
for the Lenders, pursuant to which K2HV may provide the Company with term loans in an aggregate principal amount of up to a $
On
August 7, 2020, the Company entered into an Open Market Sale AgreementSM (the “August 2020 Sale Agreement”)
with Jefferies LLC (“Jefferies”), as sales agent, pursuant to which the Company may issue and sell, from time to time,
through Jefferies, shares of its common stock, and pursuant to which Jefferies may sell its common stock by any method permitted
by law deemed to be an “at the market offering” as defined by Rule 415(a)(4) promulgated under the Securities Act
of 1933, as amended. The Company will pay Jefferies a commission of
| F-7 |
| 3. | SIGNIFICANT ACCOUNTING POLICIES |
A summary of the significant accounting policies followed by the Company in the preparation of the financial statements is as follows:
Consolidation
The consolidated financial statements include the accounts of the Company and its wholly-owned subsidiaries. All significant intercompany transactions and accounts have been eliminated in consolidation.
Use of Estimates
The process of preparing financial statements in conformity with accounting principles generally accepted in the United States of America (“U.S. GAAP”) requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates and changes in estimates may occur. The most significant estimates are related to stock-based compensation expense, the accrual of research, product development and clinical obligations, the recognition of revenue under the Investment Agreement (See Note 9), the valuation of the CFF and K2HV warrants discussed in Note 13 and Note 7, and the derivative liability associated with the K2 Security and Loan agreement (see Note 14).
Cash and Cash Equivalents
The
Company considers only those investments which are highly liquid, readily convertible to cash, and that mature within three months
from date of purchase to be cash equivalents. Marketable investments are those with original maturities in excess of three months.
At December 31, 2020 and 2019, cash equivalents were comprised of money market funds. The Company had
Restricted
cash as of December 31, 2020 included a collateral account for the Company’s corporate credit cards and is classified in
current assets in the amount of $
Cash and cash equivalents consists of the following :
| December 31, | ||||||||
| 2020 | 2019 | |||||||
| Cash | $ | $ | ||||||
| Money market fund | ||||||||
| Total cash and cash equivalents | $ | $ | ||||||
| Restricted cash, current | ||||||||
| Restricted cash, noncurrent | ||||||||
| Total restricted cash | ||||||||
| Total cash, cash equivalents, and restricted cash shown in the statement of cash flows | $ | $ | ||||||
As
of December 31, 2020, all of the Company’s cash and cash equivalents was held in the United States, except for approximately
$
Financial Instruments
The carrying values of the notes payable and debt approximate their fair value due to the fact that they are at market terms.
Fair Value Measurements
The valuation of the company’s debt and embedded derivatives are determined primarily by an income approach that considers the present value of net cash flows of the debt with and without prepayment and default features. In accordance with ASC 815 “Accounting for Derivative Instruments and Hedging Activities”, these embedded debt features which are determined to be classified as derivative liabilities are marked-to-market each reporting period, with a corresponding non-cash gain or loss charged to the current period. As such, fair value is a market-based measurement that should be determined based on assumptions that market participants would use in pricing an asset or liability. As a basis for considering such assumptions, there exists a three-tier fair value hierarchy, which prioritizes the inputs used in measuring fair value as follows:
Level 1 – Unadjusted quoted prices in active markets for identical assets or liabilities that the Company has the ability to access as of the measurement date
Level 2 – Inputs other than quoted prices included within Level 1 that are directly observable for the asset or liability or indirectly observable through corroboration with observable market data
Level 3 – Unobservable inputs for the asset or liability only used when there is little, if any, market activity for the asset or liability at the measurement date
To determine the fair value of our embedded derivatives, management evaluates assumptions regarding the probability of certain future events. Other factors used to determine fair value include the discount rate, risk free interest rate and derivative term. The fair value recorded for the derivative liability varies from period to period. This variability may result in the actual derivative liability for a period either above or below the estimates recorded on our consolidated financial statements, resulting in fluctuations in other income (expense) because of the corresponding non-cash gain or loss recorded.
Property and Equipment
Research and Development Expenses
Costs incurred for research and development are expensed as incurred.
| F-8 |
Nonrefundable advance payments for goods or services that have the characteristics that will be used or rendered for future research and development activities pursuant to executory contractual arrangements with third party research organizations are deferred and recognized as an expense as the related goods are delivered or the related services are performed.
Accruals for Research and Development Expenses and Clinical Trials
As part of the process of preparing its financial statements, the Company is required to estimate its expenses resulting from its obligations under contracts with vendors, clinical research organizations and consultants and under clinical site agreements in connection with conducting clinical trials. The financial terms of these contracts are subject to negotiations, which vary from contract to contract and may result in payment terms that do not match the periods over which materials or services are provided under such contracts. The Company’s objective is to reflect the appropriate expenses in its financial statements by matching those expenses with the period in which services are performed and efforts are expended. The Company accounts for these expenses according to the timing of various aspects of the expenses. The Company determines the accrual estimates by taking into account discussion with applicable personnel and outside service providers as to the progress of clinical trials, or the services completed. During the course of a clinical trial, the Company adjusts its clinical expense recognition if actual results differ from its estimates. The Company makes estimates of its accrued expenses as of each balance sheet date based on the facts and circumstances known to it at that time. The Company’s clinical trial accruals are dependent upon the timely and accurate reporting of contract research organizations and other third-party vendors. Although the Company does not expect its estimates to be materially different from amounts actually incurred, its understanding of the status and timing of services performed relative to the actual status and timing of services performed may vary and may result in it reporting amounts that are too high or too low for any particular period. For the years ended December 31, 2020 and 2019, there were no material adjustments to the Company’s prior period estimates of accrued expenses for clinical trials.
Leases
The Company determines if an arrangement is a lease at inception. Operating leases are included in operating lease right-of-use (“ROU”) assets, other current liabilities and operating lease liabilities in the Company’s consolidated balance sheets.
ROU assets represent the Company’s right to use an underlying asset for the lease term and lease liabilities represent its obligation to make lease payments arising from the lease. ROU assets and liabilities are recognized at commencement date based on the present value of lease payments over the lease term. As the Company’s leases do not provide an implicit rate, the Company uses an incremental borrowing rate based on the information available at commencement date in determining the present value of lease payments. This is the rate the Company would have to pay if borrowing on a collateralized basis over a similar term to each lease. The ROU asset also includes any lease payments made and excludes lease incentives. Lease expense for lease payments is recognized on a straight-line basis over the lease term.
Concentrations of Credit Risk
The Company has no significant off-balance-sheet concentration of credit risk such as foreign exchange contracts, option contracts or other hedging arrangements. The Company may from time to time have cash in banks in excess of Federal Deposit Insurance Corporation insurance limits. However, the Company believes the risk of loss is minimal as these banks are large financial institutions.
Segment Information
Operating
segments are identified as components of an enterprise about which separate discrete financial information is available for evaluation
by the chief operating decision maker, or decision-making group, in making decisions regarding resource allocation and assessing
performance. To date, the Company has viewed its operations and manages its business as principally one operating segment, which
is developing and commercializing therapeutics to treat rare life-threatening inflammatory and fibrotic diseases. As of December
31, 2020, all of the Company’s assets were located in the United States, except for approximately $
| F-9 |
Income Taxes
For
federal and state income taxes, deferred tax assets and liabilities are recognized based upon temporary differences between the
financial statement and the tax basis of assets and liabilities. Deferred income taxes are based upon prescribed rates and enacted
laws applicable to periods in which differences are expected to reverse. A valuation allowance is recorded to reduce a net deferred
tax benefit when it is not more likely than not that the tax benefit from the deferred tax assets will be realized. Accordingly,
given the cumulative losses since inception, the Company has provided a valuation allowance equal to
Tax
positions taken or expected to be taken in the course of preparing the Company’s tax returns are required to be evaluated
to determine whether the tax positions are “more-likely-than-not” of being sustained by the applicable tax authority.
Tax positions not deemed to meet a more-likely-than-not threshold, as well as accrued interest and penalties, if any, would be
recorded as a tax expense in the current year. There were
Impairment of Long-lived Assets
The
Company continually monitors events and changes in circumstances that could indicate that carrying amounts of long-lived assets
may not be recoverable. An impairment loss is recognized when expected undiscounted cash flows of an asset are less than an asset’s
carrying value. Accordingly, when indicators of impairment are present, the Company evaluates the carrying value of such assets
in relation to the operating performance and future undiscounted cash flows of the underlying assets. An impairment loss equal
to the excess of the fair value of the asset over its carrying amount, is recorded when it is determined that the carrying value
of the asset may not be recoverable.
The Company recognizes compensation costs resulting from the issuance of stock-based awards to employees, non-employees and directors as an expense in the statement of operations over the service period based on a measurement of fair value for each stock-based award. The fair value of each option grant to employees is estimated as of the date of grant using the Black-Scholes option-pricing model, net of estimated forfeitures. The fair value is amortized as compensation cost on a straight-line basis over the requisite service period of the awards, which is generally the vesting period.
| F-10 |
Foreign Currency
Transaction gains and losses arising from currency exchange rate fluctuations on transactions denominated in a currency other than the U.S. Dollar functional currency are recorded in the Company’s statement of operations. Such transaction gains and losses may be realized or unrealized depending upon whether the transaction settled during the period or remains outstanding at the balance sheet date.
Basic and diluted net loss per share of the Company’s common stock has been computed by dividing net loss by the weighted average number of shares outstanding during the period. For years in which there is a net loss, options and warrants are anti-dilutive and therefore excluded from diluted loss per share calculations. The following table sets forth the computation of basic and diluted earnings per share for the years ended December 31, 2020 and 2019:
| Years Ended December 31, | ||||||||
| 2020 | 2019 | |||||||
| Basic and diluted net loss per share of common stock: | ||||||||
| Net loss | $ | ( | ) | $ | ( | ) | ||
| Weighted average shares of common stock outstanding | ||||||||
| Net loss per share of common stock-basic and diluted | $ | ( | ) | $ | ( | ) | ||
| December 31, | ||||||||
| 2020 | 2019 | |||||||
| Warrants | ||||||||
| Stock options | ||||||||
Recent Accounting Pronouncements
The Company considers applicability and impact of all Accounting Standard Updates (“ASUs”). ASUs not discussed below were assessed and determined to be either not applicable or are expected to have minimal impact on the Company’s balance sheets or statements of operations.
| F-11 |
Collaborative Arrangements
In November 2018, the FASB issued ASU 2018-18, Collaborative Arrangements (Topic 808): Clarifying the Interaction between Topic 808 and Topic 606 (“ASU 2018-18”). ASU 2018-18 clarifies the interaction between the accounting guidance for collaborative arrangements and revenue from contracts with customers. ASU 2018-18 is effective for public business entities for fiscal years beginning after December 15, 2019, including interim periods within that fiscal year. The Company’s adoption of ASU 2018-18 as of January 1, 2019 had no impact on the Company’s financial statements and related disclosures.
Accounting for Income Taxes
In December 2019, the FASB issued ASU 2019-12, Income Taxes (Topic 740): Simplifying the Accounting for Income Taxes which is intended to simplify various aspects related to accounting for income taxes. The standard is effective for fiscal years, and interim periods within those years, beginning after December 15, 2020, with early adoption permitted. The standard will be adopted upon the effective date for us beginning January 1, 2021. The Company’s adoption of ASU 2019-12 as of January 1, 2021 will not have a material impact on the Company’s financial statements and related disclosures.
Accounting for Convertible Instruments and Contracts in an Entity’s Own Equity
In August 2020, the FASB issued ASU 2020-06, Debt—Debt with Conversion and Other Options (Subtopic 470-20) and Derivatives and Hedging—Contracts in Entity’s Own Equity (Subtopic 815-40): Accounting for Convertible Instruments and Contracts in an Entity’s Own Equity which is intended to simplify various aspects generally accepted accounting principles (GAAP) for certain financial instruments with characteristics of liabilities and equity. The standard is effective for public companies that meet definition of a Securities and Exchange Commission (SEC) filer, excluding entities to be smaller reporting companies as defined by the SEC, for fiscal years, and interim periods within those years, beginning after December 15, 2021. For all other entities, the amendments are effective for fiscal years beginning after December 15, 2023, including interim periods within those fiscal years. Early adoption is permitted, but no earlier than fiscal years beginning after December 15, 2020, including interim periods within those fiscal years. The Company is currently evaluating the timing of the adoption of ASU 2020-06 and the expected impact it could have on the Company’s financial statements and related disclosures.
| 4. | LICENSE AGREEMENT |
The Company entered into a License Agreement (the “Jenrin Agreement”) with Jenrin Discovery, LLC, a privately-held Delaware limited liability company (“Jenrin”), effective September 20, 2018. Pursuant to the Jenrin Agreement, Jenrin granted the Company exclusive worldwide rights to develop and commercialize the Licensed Products (as defined in the Jenrin Agreement) which includes the Jenrin library of over 600 compounds and multiple issued and pending patent filings. The compounds are designed to treat inflammatory and fibrotic diseases by targeting the endocannabinoid system.
In
consideration of the license and other rights granted by Jenrin, the Company paid Jenrin a $
In
January 2017, the FASB issued ASU 2017-01, Business Combinations (Topic 805): Clarifying the Definition of a Business (“ASU
2017-01”) which clarifies the definition of a business and determines when an integrated set of assets and activities is
not a business. ASU 2017-01 requires that if substantially all of the fair value of gross assets acquired or disposed of is concentrated
in a single asset or group of similar identifiable assets, the assets would not represent a business. The Company determined that
substantially all of the fair value of the Jenrin Agreement was attributable to a single in-process research and development asset
which did not constitute a business. The Company concluded that it did not have any alternative future use for the acquired in-process
research and development asset. Thus, the Company recorded the $
| F-12 |
| 5. | PROPERTY AND EQUIPMENT |
Property and Equipment consisted of the following:
| December 31, | ||||||||
| 2020 | 2019 | |||||||
| Computer hardware and software | $ | $ | ||||||
| Office furniture and equipment | ||||||||
| Leasehold improvements | ||||||||
| Property and equipment, gross | ||||||||
| Less: accumulated depreciation | ( | ) | ( | ) | ||||
| Property and equipment, net | $ | $ | ||||||
Depreciation
expense was approximately $
| 6. | COMMITMENTS AND CONTINGENCIES |
Operating Lease Commitment
On
August 21, 2017, the Company entered into a lease agreement (“August 2017 Lease Agreement”) for commercial lease of
office space, pursuant to which the Company agreed to lease
The
Company adopted ASU 2016-02, Leases (Topic 842), as amended (“ASU 2016-02”) using the effective date method
as of January 1, 2019 and recorded a lease liability of approximately $
ROU
assets represent the Company’s right to use an underlying asset for the lease term and lease liabilities represent its obligation
to make lease payments arising from the lease. ROU assets and liabilities are recognized at the date of adoption based on the
present value of lease payments over the lease term. As the Company’s leases do not provide an implicit rate, the Company
uses an incremental borrowing rate based on the information available at commencement date in determining the present value of
lease payments, which was
| F-13 |
On
February 26, 2019, the Company amended its lease (“February 2019 Lease Agreement”) pursuant to which an additional
Per
the terms of the February 2019 Lease Agreement, the landlord agreed to reimburse the Company for approximately $
On
October 25, 2019, the Company amended its lease (“October 2019 Lease Amendment”) pursuant to which the term of the
lease was extended through November 30, 2026 and the existing office space under lease was expanded by
The following table contains a summary of the lease costs recognized under ASC 842 and other information pertaining to the Company’s operating leases for the year ended December 31, 2020 and 2019:
| 2020 | 2019 | |||||||
| Lease cost | ||||||||
| Operating lease cost | $ | |||||||
| Total lease cost | $ | |||||||
| Other information | ||||||||
| Weighted average remaining lease term | ||||||||
| Weighted average discount rate | % | % | ||||||
Total
rent expense for the years ended December 31, 2020 and 2019 was $
Pursuant to the terms of the Company’s non-cancelable lease agreements in effect at December 31, 2020, the following table summarizes the Company’s maturities of operating lease liabilities as of December 31, 2020:
Year ending December 31, 2020:
| 2021 | $ | |||
| 2022 | ||||
| 2023 | ||||
| 2024 | ||||
| 2025 | ||||
| Thereafter | ||||
| Total lease payments | $ | |||
| Less: imputed interest | $ | ( | ) | |
| Total | $ |
| F-14 |
For commitments under the Company’s development award agreements- see Note 9.
| 7. | NOTES PAYABLE |
D&O Financing
In
November 2019, the Company entered into a loan agreement with a financing company for $
In
November 2020, the Company entered into a loan agreement with a financing company for $
Loan and Security Agreement with K2 HealthVentures LLC
On
July 28, 2020, the Company, with its subsidiary, Corbus Pharmaceuticals, Inc., as borrower, entered into a $
In
connection with the Loan Agreement, on July 28, 2020, the Company issued the Lenders a warrant to purchase up to common
shares (the “K2 Warrant”) at an exercise price of $
The
total principal amount of the loan under the Loan Agreement outstanding at December 31, 2020, including the $
Upon
the occurrence of an Event of Default (as defined in the Loan Agreement), and during the continuance of an Event of Default, the
applicable rate of interest, described above, will be increased by
The
total debt discount related to Lenders of approximately $
The net carrying amounts of the liability components consists of the following:
| December 31, 2020 | ||||
| Principal | $ | |||
| Less: debt discount | ( | ) | ||
| Accretion of Debt Discount | ||||
| Net Carrying amount | $ | |||
The following table summarizes the future principal payments due under long-term debt;
Principal Payments and final payment on Loan Agreement | ||||
| 2021 | $ | |||
| 2022 | ||||
| 2023 | ||||
| 2024 | ||||
| Total | $ | |||
| F-15 |
| 8. | ACCRUED EXPENSES |
Accrued expenses consisted of the following:
| December 31, | ||||||||
| 2020 | 2019 | |||||||
| Accrued clinical operations and trials costs | $ | $ | ||||||
| Accrued product development costs | ||||||||
| Accrued compensation | ||||||||
| Accrued other | ||||||||
| Total | $ | $ | ||||||
| 9. | DEVELOPMENT AWARDS AND DEFERRED REVENUE |
Collaboration with Kaken
On January 3, 2019, the Company entered into a Collaboration and License Agreement (the “Agreement”) with Kaken Pharmaceutical Co., Ltd., a company organized under the laws of Japan (“Kaken”). Pursuant to the Agreement, Corbus granted Kaken an exclusive license to commercialize pharmaceutical preparations containing lenabasum (the “Licensed Products”) for the prevention or treatment of dermatomyositis and systemic sclerosis (together, the “Initial Indications”) in Japan (the “Territory”).
Pursuant to the terms of the Agreement, Corbus will bear the cost of, and be responsible for, among other things, conducting the clinical studies and other developmental activities for the Licensed Products in the Initial Indications in the Territory, and Kaken will bear the cost of, and be responsible for, among other things, preparing and filing applications for regulatory approval in the Territory and for commercializing Licensed Products in the Territory, and will use commercially reasonable efforts to commercialize Licensed Products and obtain pricing approval for Licensed Products in the Territory.
In
consideration of the license and other rights granted by Corbus, Kaken paid to Corbus in March 2019 a $
The
Agreement will remain in effect on a Licensed Product-by-Licensed product basis and will expire upon the expiration of the Royalty
Term for the final Licensed Product.
Pursuant to the Agreement, the parties agreed to develop a joint steering committee to provide strategic oversight of the parties’ activities under the Agreement, as well as a joint development committee to coordinate the development of Licensed Products in Japan. Additionally, the parties will establish a joint commercialization committee to review and confirm commercialization activities with respect to Licensed Products in Japan upon regulatory approval of such Licensed Product.
The Agreement also contains customary representations, warranties and covenants by both parties, as well as customary provisions relating to indemnification, confidentiality and other matters.
| F-16 |
The Company assessed this arrangement in accordance with U.S. GAAP and concluded that the contract counterparty, Kaken, is a customer. The Company identified the following material promises under the arrangement: (1) the exclusive license to commercialize lenabasum; (2) the product’s initial know-how transfer; (3) election to use the product trademarks; (4) the sharing of data gathered through the execution of the Global Development Plan for the Initial Indications; and (5) Japanese Pharmaceuticals and Medical Devices Agency (“PMDA”)-required supplemental studies. The Company identified two performance obligations; (1) the combined performance obligation of the License, initial know-how transfer and license to the Company’s product trademarks; and (2) the sharing of data gathered through the execution of the Global Development Plan (as defined in the Agreement) for the Initial Indications. The Company determined that the license and initial know-how transfer were not distinct from another in the context of the contract, as initial know-how transfer is highly interrelated to the license and Kaken would incur significant costs to re-create the know-how of the Company. The Company determined that the election to use the product trademarks license contributes to the exclusivity of the license and, therefore, is combined with the license. The PMDA-required supplemental study is a contingent promise although not a performance obligation as the promise does not provide Kaken with a material right.
Under
the Agreement, in order to evaluate the appropriate transaction price, the Company determined that the upfront amount of $
The
Company estimated the stand-alone selling price of each performance obligation using a market approach and allocated the transaction
price on a relative basis. This allocation resulted in a de minimis value attributable to the obligation to sharing of
data gathered through the execution of the Global Development Plan for the Initial Indications and effectively all of the value
to the combined license, initial know-how transfer and license to product trademarks. Therefore, the full upfront payment of $
The
Company received the upfront payment of $
The
Company was required to make a $
2018 CFF Award
On
January 26, 2018, the Company entered into the Cystic Fibrosis Program Related Investment Agreement with the CFF (“Investment
Agreement”), a non-profit drug discovery and development corporation, pursuant to which the Company received an award for
up to $
Pursuant to the terms of the Investment Agreement, the Company is obligated to make certain royalty payments to CFF, including a royalty payment of one and one-half times the amount of the 2018 CFF Award, payable in cash within sixty days upon the first receipt of approval of lenabasum in the United States and a second royalty payment of one and one-half times the amount of the 2018 CFF Award upon approval in another major market, as set forth in the Investment Agreement (the “Approval Royalty”). At the Company’s election, the Company may satisfy the first of the two Approval Royalties in registered shares of the Company’s common stock.
| F-17 |
Additionally,
the Company is obligated to make (i) royalty payments to CFF of two and one-half percent of net sales from lenabasum due within
sixty days after any quarter in which such net sales occur in the Field, as defined in the Investment Agreement, (ii) royalty
payments to CFF of one percent of net sales of Non-Field Products, as defined in the Investment Agreement due within sixty days
after any quarter in which such net sales occur, and (iii) royalty payments to CFF of ten percent of any amount the Company and
its stockholders receive in connection with the license, sale, or other transfer to a third party of lenabasum, if indicated for
the treatment or prevention of CF, or a change of control transaction, except that such payment shall not exceed five times the
amount of the 2018 CFF Award, with such payments to be credited against any other net sales royalty payments due. Accordingly,
the Company will owe to CFF a royalty payment equal to
Either CFF or the Company may terminate the Investment Agreement for cause, which includes the Company’s material failure to achieve certain commercialization and development milestones. The Company’s payment obligations survive the termination of the Investment Agreement.
Pursuant
to the terms of the Investment Agreement, the Company issued a warrant to CFF to purchase an aggregate of
Under
the Investment Agreement, the Company recorded $
The Company assessed this arrangement in accordance with ASC 606 and concluded that the contract counterparty, CFF, is a customer. The Company identified the following material promise under the arrangement: research and development activities and related services under the Phase 2b Clinical Trial. Based on these assessments, the Company identified one performance obligation at the outset of the Investment Agreement, which consists of: Phase 2b Clinical Trial research and development activities and related services.
To
determine the transaction price, the Company included the total aggregate payments under the Investment Agreement which amount
to $
The
Company has invoiced and received $
| December 31, 2020 | ||||
| Beginning balance, December 31, 2019 | $ | |||
| Invoicing to CFF upon achievement of milestones | ||||
| Recognition of revenue | ( | ) | ||
| Reclassification to contract asset | ( | ) | ||
| Ending balance, December 31, 2020 | $ | |||
| F-18 |
The CFF Warrant is accounted for as a payment to the customer. See Note 13 for further information related to the CFF Warrant. The Company notes that the Investment Agreement contains an initial payment that was received upon contract execution and subsequent milestone payments, which are a form of variable consideration that require evaluation for constraint considerations. The Company concluded that the related performance milestones are generally within the Company’s control and as result are considered probable. Revenue associated with the performance obligation is being recognized as revenue as the research and development services are provided using an input method, according to the costs incurred as related to the research and development activities on each program and the costs expected to be incurred in the future to satisfy the performance obligation. The transfer of control occurs over this time period and, in management’s judgment, is the best measure of progress towards satisfying the performance obligation. The research and development services related to this performance obligation are expected to be performed over approximately and is expected to be completed in the first half of 2021. The amounts received that have not yet been recognized as revenue are recorded in deferred revenue and the amounts recognized as revenue, but not yet received or invoiced are generally recognized as a contract asset on the Company’s condensed consolidated balance sheet.
| 10. | INCOME TAXES |
No provision or benefit for federal or state income taxes has been recorded, as the Company has incurred a net loss for all of the periods presented, and the Company has provided a full valuation allowance against its deferred tax assets.
At
December 31, 2020 and 2019, the Company had federal net operating loss carryforwards of approximately $
In
the second half of 2020, the Company received from a foreign taxing authority, an approximate aggregate $
Significant components of the Company’s net deferred tax asset are as follows:
| December 31, | ||||||||
| 2020 | 2019 | |||||||
| NOL carryforward | $ | $ | ||||||
| Foreign net operating loss carryforward | ||||||||
| Tax credits | ||||||||
| Stock based compensation | ||||||||
| Accrued expenses | ||||||||
| Other temporary differences | ||||||||
| Subtotal | ||||||||
| Valuation allowance | ( | ) | ( | ) | ||||
| Net deferred tax asset | $ | $ | ||||||
The
Company has maintained a full valuation allowance against its deferred tax assets in all periods presented. A valuation allowance
is required to be recorded when it is not more likely than not that some portion or all of the net deferred tax assets will be
realized. Since the Company cannot determine that it is more likely than not that it will generate taxable income, and thereby
realize the net deferred tax assets, a full valuation allowance has been provided. The valuation allowance increased by $
| F-19 |
Income tax benefits computed using the federal statutory income tax rate differs from the Company’s effective tax rate primarily due to the following:
| December 31, | ||||||||
| 2020 | 2019 | |||||||
| Tax provision at statutory rate | % | % | ||||||
| State taxes, net of federal benefit | % | % | ||||||
| Permanent differences | - | % | - | % | ||||
| Foreign expected tax | % | % | ||||||
| Tax credits | % | % | ||||||
| Income tax rate change | % | % | ||||||
| Other | - | % | % | |||||
| Decrease in valuation reserve | - | % | - | % | ||||
| Total | % | % | ||||||
| 11. | COMMON STOCK |
The Company has authorized shares of common stock, $ par value per share, of which shares, and shares were issued and outstanding as of December 31, 2020, and 2019, respectively.
| F-20 |
On
January 30, 2019, the Company consummated an underwritten public offering of shares of its common stock pursuant to which the
Company sold an aggregate of shares of its common stock, including shares sold pursuant to the full exercise
of the underwriters’ option to purchase additional shares, at a purchase price of $ per share with gross proceeds to
the Company totaling approximately $
On
February 11, 2020, the Company consummated an underwritten public offering of shares of its common stock pursuant to which the
Company sold an aggregate of shares of its common stock, including shares sold pursuant to the full exercise
of the underwriters’ option to purchase additional shares, at a purchase price of $ per share with gross proceeds to
the Company totaling $
On
April 7, 2020, the Company entered into the April 2020 Sale Agreement with Jefferies pursuant to which Jefferies served as the
Company’s sales agent to sell up to $ of shares of the Company’s common stock through an “at the market
offering.” Sales of common stock under the April 2020 Sale Agreement were made pursuant to an effective registration statement
for an aggregate offering of up to $
On
August 7, 2020, the Company entered into the August 2020 Sale Agreement with Jefferies pursuant to which Jefferies is serving
as the Company’s sales agent to sell shares of the Company’s common stock through an “at the market offering.”
As of August 7, 2020, the company was authorized to sell up to $ of shares of the Company’s common stock pursuant
to the August 2020 Sale Agreement. During the year ended December 31, 2020. During the year ended December 31, 2020, the Company
sold shares of its common stock under the August 2020 Sale Agreement for which the Company received gross proceeds
of approximately $
During
the year ended December 31, 2020 and 2019, the Company issued and shares of common stock upon the exercise of
stock options to purchase common stock and the Company received proceeds of approximately $
warrants were exercised during the year ended December 31, 2020. During the year ended December 31, 2019, warrants to purchase shares of stock were exercised on a cashless basis resulting in the issuance of shares of common stock.
| 12. | STOCK OPTIONS |
In April 2014, the Company adopted the Corbus Pharmaceuticals Holdings, Inc. 2014 Equity Incentive Plan (the “2014 Plan”). Pursuant to the 2014 Plan, the Company’s Board of Directors may grant incentive and nonqualified stock options and restricted stock to employees, officers, directors, consultants and advisors. Pursuant to the terms of an annual evergreen provision in the 2014 Plan, the number of shares of common stock available for issuance under the 2014 Plan shall automatically increase on January 1 of each year by at least seven percent (%) of the total number of shares of common stock outstanding on December 31st of the preceding calendar year, or, pursuant to the terms of the 2014 Plan, in any year, the Board of Directors may determine that such increase will provide for a lesser number of shares. On January 1, 2020, pursuant to an annual evergreen provision contained in the 2014 Plan, the number of shares reserved for future grants was increased by shares, which was seven percent (%) of the outstanding shares of common stock on December 31, 2019. As of December 31, 2020, there was a total of shares reserved for issuance under the 2014 Plan and there were shares available for future grants. Options issued under the 2014 Plan generally vest over years from the date of grant in multiple tranches and are exercisable for up to years from the date of issuance.
In accordance with the terms of the 2014 Plan, effective as of January 1, 2021, the number of shares of common stock available for issuance under the 2014 Plan increased by shares, which was less than seven percent (%) of the outstanding shares of common stock on December 31, 2020 (see Note 15). As of January 1, 2021, the 2014 Plan had a total reserve of shares and there were shares available for future grants.
Share-based Compensation
For stock options issued and outstanding for the years ended December 31, 2020 and 2019, the Company recorded non-cash, stock-based compensation expense of $ and $, respectively, net of estimated forfeitures.
The fair value of each option award for employees is estimated on the date of grant and for non-employees is estimated at the end of each reporting period until vested using the Black-Scholes option pricing model that uses the assumptions noted in the following table. The Company uses historical data, as well as subsequent events occurring prior to the issuance of the financial statements, to estimate option exercises and employee terminations in order to estimate its forfeiture rate. The expected term of options granted under the 2014 Plan, all of which qualify as “plain vanilla” per SEC Staff Accounting Bulletin 107, is determined based on the simplified method due to the Company’s limited operating history, and is years based on the average between the vesting period and the contractual life of the option. For non-employee options, the expected term is the contractual term. The risk-free rate is based on the yield of a U.S. Treasury security with a term consistent with the option.
| F-21 |
| 2020 | 2019 | |||||||
| Risk free interest rate | % | % | ||||||
| Expected dividend yield | % | % | ||||||
| Expected term in years | ||||||||
| Expected volatility | % | % | ||||||
| Estimated forfeiture rate | % | % | ||||||
| Options | Shares | Weighted Average Exercise Price | Weighted Average Remaining Contractual Term in Years | Intrinsic Value | ||||||||||||
| Outstanding at December 31, 2018 | $ | |||||||||||||||
| Granted | $ | |||||||||||||||
| Exercised | ( | ) | $ | |||||||||||||
| Forfeited | ( | ) | $ | |||||||||||||
| Outstanding at December 31, 2019 | $ | |||||||||||||||
| Granted | $ | |||||||||||||||
| Exercised | ( | ) | $ | |||||||||||||
| Forfeited | ( | ) | $ | |||||||||||||
| Outstanding at December 31, 2020 | $ | $ | ||||||||||||||
| Exercisable at December 31, 2020 | $ | $ | ||||||||||||||
| Vested and expected to vest at December 31, 2020 | $ | $ | ||||||||||||||
The weighted average grant-date fair value of options granted during the years ended December 31, 2020 and 2019 was $ and $ per share, respectively. The aggregate intrinsic value of options exercised during the years ended December 31, 2020 and 2019 was approximately $ and $, respectively. As of December 31, 2020, there was approximately $ of total unrecognized compensation expense, related to non-vested share-based compensation arrangements. The unrecognized compensation expense is estimated to be recognized over a period of years at December 31, 2020.
As summary of non-vested stock options for the years ended December 31, 2020 and 2019 is presented below:
| Options | Shares | Weighted Average Fair Value | ||||||
| Non-vested at December 31, 2018 | $ | |||||||
| Granted | $ | |||||||
| Vested | ( | ) | $ | |||||
| Forfeited | ( | ) | $ | |||||
| Nonvested at December 31, 2019 | $ | |||||||
| Granted | $ | |||||||
| Vested | ( | ) | $ | |||||
| Forfeited | ( | ) | $ | |||||
| Non-vested at December 31, 2020 | $ | |||||||
| F-22 |
| 13. | WARRANTS |
warrants were exercised during the year ended December 31, 2020. During the year ended December 31, 2019, warrants to purchase shares of stock were exercised on a cashless basis resulting in the issuance of shares of common stock.
At
December 31, 2020, there were warrants outstanding to purchase
The
Company issued a warrant to CFF to purchase an aggregate of
| Risk free interest rate | % | |||
| Expected dividend yield | % | |||
| Expected term in years | ||||
| Expected volatility | % |
On
July 28, 2020, the Company entered into the Loan Agreement with K2HV pursuant to which K2HV may provide the Company with term
loans in an aggregate principal amount of up to $
| Risk free interest rate | % | |||
| Expected dividend yield | % | |||
| Expected term in years | ||||
| Expected volatility | % |
On
October 16, 2020, the Company entered into a professional services agreement with an investor relations service provider.
Pursuant to the agreement, the Company issued warrants exercisable for a total of
| Risk free interest rate | % | |||
| Expected dividend yield | % | |||
| Expected term in years | ||||
| Expected volatility | % |
| 14. | DERIVATIVE LIABILITY |
On
July 28, 2020, the Company, with its subsidiary, Corbus Pharmaceuticals, Inc., as borrower, entered into a $
The
value of these features are determined each reporting period by taking the present value of net cash flows with and without the
prepayment features. The significant assumption used to determine the fair value of the debt without any features is the discount
rate which has been estimated by using published market rates of triple CCC rated public companies. All other inputs are taken
from the Loan Agreement. The additional significant assumptions used when valuing the prepayment feature is the probability of
a change of control event. The Company has determined the probability increased from July 28, 2020 to December 31, 2020 as a result
of SSc-002 phase 3 and CF-002 phase 2 trial results. The additional significant assumption used when valuing the default feature
is the probability of defaulting on the repayment of loan. The Company has determined the probability increased from July 28,
2020 to December 30, 2020. As the probability of both features increased the fair value of the derivative liability has increased
at December 31, 2020. The value of these features was determined to be approximately $
A roll forward of the fair value of the derivative liability for the year ended December 31, 2020 is presented below.
| December 31, 2020 | ||||
| Beginning balance, December 31, 2019 | $ | |||
| Initial measurement of fair value | ||||
| Change in fair value of derivative liability | ||||
| Ending balance, December 31, 2020 | $ | |||
| 15. | SUBSEQUENT EVENTS
Evergreen Provision
Pursuant to the terms of an annual evergreen provision in the 2014 Plan, the number of shares of common stock available for issuance under the 2014 Plan shall automatically increase on January 1 of each year by at least seven percent (%) of the total number of shares of common stock outstanding on December 31st of the preceding calendar year, or, pursuant to the terms of the 2014 Plan, in any year, the Board of Directors may determine that such increase will provide for a lesser number of shares. In accordance with the terms of the 2014 Plan, effective as of January 1, 2021, the number of shares of common stock available for issuance under the 2014 Plan increased by shares, such amount being less than seven percent (%) of the outstanding shares of common stock on December 31, 2020. As of January 1, 2021, the 2014 Plan had a total reserve of shares and there were shares available for future grants. |
Sales of Stock
The
Company has sold an additional shares of our common stock under the
August 2020 Sale Agreement for net proceeds of approximately $
| F-23 |