Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended: December 31, 2015
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission file number: 001-36167
KARYOPHARM THERAPEUTICS INC.
(Exact name of registrant as specified in its charter)
| Delaware | 26-3931704 | |
| (State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification No.) |
85 Wells Avenue, 2nd Floor, Newton, Massachusetts 02459
(Address of principal executive offices) (zip code)
Registrant’s telephone number, including area code: (617) 658-0600
Securities registered pursuant to Section 12(b) of the Act:
| (Title of each class) |
(Name of each exchange on which listed) | |
| Common Stock, $0.0001 par value | NASDAQ Global Select Market |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See definitions of “large accelerated filer,” “accelerated filer,” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer | ¨ | Accelerated filer | x | |||
| Non-accelerated filer | ¨ (Do not check if a smaller reporting company) | Smaller reporting company | ¨ |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ¨ No x
The aggregate market value of the registrant’s voting and non-voting common stock held by non-affiliates of the registrant (without admitting that any person whose shares are not included in such calculation is an affiliate) computed by reference to the price at which the common stock was last sold on June 30, 2015 was approximately $628,259,799. Shares of common stock held by each executive officer, director, and holder of 10% or more of the outstanding common stock have been excluded in that such persons may be deemed to be affiliates. This determination of affiliate status is not necessarily a conclusive determination for other purposes.
Number of shares outstanding of the registrant’s Common Stock as of March 7, 2016: 35,881,173.
Documents incorporated by reference:
Portions of our definitive proxy statement to be filed with the Securities and Exchange Commission no later than April 29, 2016 in connection with our 2016 annual meeting of stockholders are incorporated by reference into Part III of this Annual Report on Form 10-K.
Table of Contents
2
Table of Contents
Forward-Looking Information
This Annual Report on Form 10-K contains forward-looking statements regarding the expectations of Karyopharm Therapeutics Inc., herein referred to as “Karyopharm,” the “company,” “we,”, or “our,” with respect to the possible achievement of discovery and development milestones in 2016, our future discovery and development efforts, our potential collaborations with third parties, our future operating results and financial position, our business strategy, and other objectives for future operations. We often use words such as “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,” “plan,” “predict,” “project,” “target,” “potential,” “will,” “would,” “could,” “should,” “continue,” and other words and terms of similar meaning to help identify forward-looking statements, although not all forward-looking statements contain these identifying words. You also can identify these forward-looking statements by the fact that they do not relate strictly to historical or current facts. There are a number of important risks and uncertainties that could cause actual results or events to differ materially from those indicated by forward-looking statements. These risks and uncertainties include those inherent in pharmaceutical research and development, such as adverse results in our drug discovery and clinical development activities, decisions made by the U.S. Food and Drug Administration and other regulatory authorities with respect to the development and commercialization of our drug candidates, our ability to obtain, maintain and enforce intellectual property rights for our drug candidates, dependence on any collaborators we may have in the future, competition, our ability to obtain any necessary financing to conduct our planned activities, and other risk factors. Please refer to the section entitled “Risk Factors” in Part I of this report for a description of these risks and uncertainties. Unless required by law, we do not undertake any obligation to update any forward-looking statements.
| Item 1. | Business |
Overview
We are a clinical-stage pharmaceutical company focused on the discovery, development and subsequent commercialization of novel, first-in-class drugs directed against nuclear transport and related targets for the treatment of cancer and other major diseases. Our scientific expertise is focused on understanding the regulation of intracellular communication between the nucleus and the cytoplasm. We have discovered and are developing wholly-owned, novel, small molecule Selective Inhibitor of Nuclear Export, or SINE™, compounds that inhibit the nuclear export protein XPO1. These SINE compounds represent a new class of drug candidates with a novel mechanism of action that have the potential to treat a variety of diseases in areas of unmet medical need. Our SINE compounds were the first oral XPO1 inhibitors in clinical development.
Our initial focus is on seeking the regulatory approval and commercialization of our lead drug candidate, selinexor (KPT-330), as an orally administered agent in cancer indications with significant unmet clinical need, initially for hematologic malignancies. We then plan to seek additional approvals for the use of selinexor in combination therapies to expand the patient populations that are eligible for selinexor, as well as to move selinexor further towards front-line cancer therapy. We are also advancing the clinical development of selinexor in multiple solid tumor indications. To date, we have initiated multiple later-phase clinical trials to evaluate selinexor in hematological cancers and solid tumors. We have also initiated a double-blinded, placebo-controlled, randomized Phase 2/3 study of single-agent selinexor in liposarcoma and expect to initiate in the middle of 2016 a double-blinded, randomized Phase 2/3 study of selinexor in combination with carfilzomib (Kyprolis®) and dexamethasone to treat multiple myeloma. We are preparing to establish the commercial infrastructure to support a potential launch of selinexor for hematologic indications in North America and Western Europe.
3
Table of Contents
Summary of Clinical Development
Oral selinexor is being evaluated in multiple later-phase clinical trials in patients with relapsed and/or refractory hematological and solid tumor malignancies. To date, selinexor has been administered to more than 1400 patients across company-sponsored and investigator-sponsored clinical trials. Evidence of single-agent anti-cancer activity has been observed in many patients and selinexor has been sufficiently well-tolerated to allow several of these patients to remain on therapy for prolonged periods. Over 20 patients have remained on study for over 12 months, with the longest patients on study for over 24 months.
During 2015, a diverse set of clinical data for selinexor was presented across a variety of indications. We presented an analysis of data from 266 patients with hematological malignancies who were treated with selinexor during our Phase 1 clinical trial. The primary objectives of the Phase 1 trial were to determine the safety, tolerability and recommended Phase 2 and Phase 3 dose of orally administered selinexor. Patients were dosed 3-80mg/m2 (equivalent to approximately 5-130mg) of selinexor orally over a four-week cycle, with lower doses initially given ten times per cycle and higher doses usually given twice weekly. Data indicate that significantly less weight loss was observed in patients who received selinexor dosed at 60mg or less, that patients treated with 60mg or less of selinexor remained on the study longer than patients treated with selinexor dosed at 65mg or higher and that selinexor dosed at approximately 60mg is associated with maximal overall response rates. Pharmacokinetics for selinexor based on flat dose was comparable to dosing based on body surface area. As a result of this analysis, we concluded that the recommended Phase 2 dose for selinexor in most cancer indications is 60mg given twice weekly and we believe that this dose optimizes the therapeutic window, response rates and duration of treatment.
Selinexor data were also presented showing preliminary safety and efficacy as a single agent in patients with solid tumors including glioblastoma, sarcoma and gynecological malignancies, in combination with carfilzomib and dexamethasone to treat patients with multiple myeloma and in combination with standard of care chemotherapy to treat patients with acute myeloid leukemia.
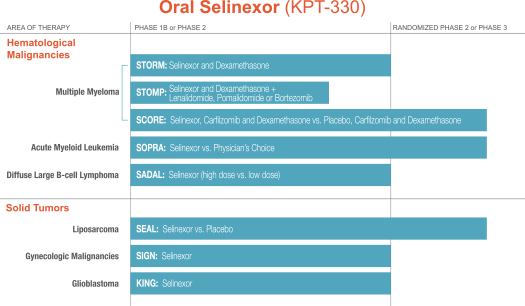
Our ongoing company-sponsored clinical trials of selinexor, along with anticipated timing of key data points, are summarized in the chart below. In addition, there are several ongoing investigator-sponsored clinical trials in a variety of hematological and solid tumor malignancies.
4
Table of Contents
We have previously announced data from the SIGN and KING studies and these data are further described herein. We currently expect to provide data related to the other studies of selinexor listed above as follows:
STORM: Phase 2b topline data (Overall Response Rate) in mid-2016
STOMP: Phase 1b topline data (Recommended Phase 2 Dose) in late 2016
SCORE: Phase 2 topline data (Overall Response Rate) in mid-2017
SOPRA: Phase 2 interim analysis in late 2016; Phase 2 topline data (Overall Survival) in mid-2017
SADAL: Phase 2b topline data (Overall Response Rate) in early 2017
SEAL: Phase 2 topline data (Progression Free Survival) in mid-2017
In addition to selinexor, we are also advancing a pipeline of novel drug candidates in both oncology and neurological, inflammatory, autoimmune and viral indications. We began clinical testing of KPT-8602, a second generation SINE compound, in December 2015 to treat patients with relapsed/refractory multiple myeloma and we expect to being clinical testing of KPT-9274, a dual PAK4/NAMPT inhibitor in the middle of 2016 in patients with lymphoma or solid tumors. KPT-350 is an investigational new drug application-ready oral compound with a preclinical data package supporting potential efficacy in a number of neurological, autoimmune and inflammatory conditions. We plan to partner with a collaborator to undertake the clinical development and potential commercialization of KPT-350 in one or more mutually agreed indications. We began clinical testing of verdinexor (KPT-335) in May 2015 in healthy human volunteers and we are preparing to advance verdinexor for certain viral indications with an initial focus on influenza. Preclinical data provide strong support for other potential indications for verdinexor, including human immunodeficiency virus, or HIV. Our pipeline of drug candidates is summarized in the chart below.

5
Table of Contents
Since our founding by Dr. Sharon Shacham in 2008, our goal has been to establish a leading, independent oncology business. We are led by Dr. Shacham, our President and Chief Scientific Officer, and Dr. Michael Kauffman, our Chief Executive Officer. Dr. Kauffman played a leadership role in the development and approval of Velcade® at Millennium Pharmaceuticals and of Kyprolis® while serving as Chief Medical Officer at Proteolix and then Onyx Pharmaceuticals. Dr. Shacham has played a leadership role in the discovery and development of many novel drug candidates, which have been or are being tested in human clinical trials, prior to her founding of Karyopharm and while at Karyopharm.
Since our inception, we have devoted substantially all of our efforts to research and development, and we have not generated any revenue to date from sales of any drugs. As of December 31, 2015, we had an accumulated deficit of $256.5 million. We had net losses of $118.2 million, $75.8 million and $33.9 million for the years ended December 31, 2015, 2014 and 2013, respectively. See our Consolidated Statements of Operations and Note 2 to our consolidated financial statements for further information regarding our research and development expenses and financial information regarding the geographic areas in which we operate.
6
Table of Contents
Summary of Mechanism of Action: Transient XPO1 Inhibition by SINE Compounds
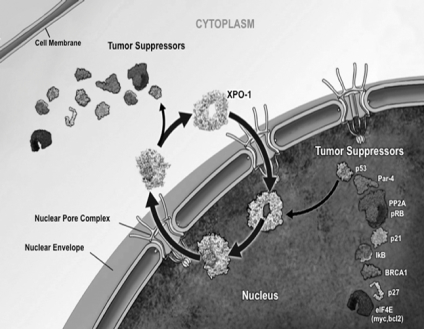
One of the ways in which a cell regulates the function of a particular protein is by controlling the protein’s location within the cell, as a specific function may only occur within a particular location in the cell. In healthy cells, nuclear transport, both into and out of the nucleus, is a normal and regular occurrence that is tightly regulated and requires specific carrier proteins to be present. XPO1 mediates the export of over 220 different mammalian cargo proteins, including the vast majority of tumor suppressor proteins, as well as the transport of certain growth-promoting mRNAs which, when transported into the cytoplasm, are translated into functional proteins at high levels. Moreover, XPO1 appears to be the only nuclear exporter for the majority of these tumor suppressor proteins and for particular growth-promoting mRNAs. Cancer cells have increased levels of XPO1, causing the increased export of these tumor suppressor proteins from the nucleus. Since the tumor suppressor proteins must be located in the nucleus to promote programmed cell death, or apoptosis, XPO1 overexpression in cancer cells counteracts the natural apoptotic process that protects the body from cancer. Due to XPO1 inhibition by our SINE compounds, the export of tumor suppressor proteins is prevented, which leads to their accumulation in the nucleus. This accumulation subsequently reinitiates and amplifies their natural apoptotic function in cancer cells with minimal effects on normal cells. Further, SINE compounds reduce the translation of certain growth-promoting proteins (including some cancer-causing proteins) by inhibiting the XPO1-mediated transport of their mRNAs to the cytoplasm. The figure below depicts the process by which our SINE compounds inhibit the XPO1 nuclear export of tumor suppressor proteins.

We believe that the XPO1-inhibiting SINE compounds that we have discovered and developed to date, including selinexor, have the potential to provide a novel, oral, targeted therapy that enables tumor suppressor proteins to remain in the nucleus and promote the apoptosis of potentially any type of cancer cell. Moreover, our SINE compounds spare normal cells, which, unlike cancer cells, do not have significant damage to their genetic material, and we believe this selectivity for cancer cells minimizes side effects. We believe that the novel mechanism of action and oral administration of selinexor and the lack of cumulative or major organ toxicities observed to date in patients treated with selinexor in clinical trials create the potential for selinexor’s broad use across many cancer types, including both hematological and solid tumor malignancies. Patient tumor biopsies have confirmed that selinexor treatment induces the nuclear localization of tumor suppressor proteins as well as cancer cell death, or apoptosis, in multiple different cancer types. We believe that no currently approved cancer treatments or current clinical-stage cancer drug candidates are selectively targeting the restoration and increase in
7
Table of Contents
the levels of multiple tumor suppressor proteins in the nucleus. Our SINE compounds were the first oral XPO1 inhibitors in clinical development. We own all intellectual property rights related to the compounds that we are developing, including composition of matter and method of use patents covering selinexor that were issued by the U.S. Patent and Trademark Office in 2015 and which provide patent protection through at least 2032, absent any adjustments or extensions.
Our Strategy
As a clinical-stage pharmaceutical company focused on the discovery and development of orally available, novel first-in-class drugs directed against nuclear transport targets for the treatment of cancer and other major diseases, the critical components of our business strategy are to:
| • | Develop and Seek Regulatory Approval of Selinexor, Our Lead Novel Drug Candidate, in North America and Western Europe. We plan to seek regulatory approvals of selinexor in North America and Western Europe in each indication with respect to which we receive positive clinical trial results in a trial with a survival endpoint that is designed to be registration-enabling. We may also seek regulatory approvals where a clinical trial demonstrates sufficiently significant data in a surrogate endpoint such as overall response rate that could allow for accelerated approval. We may seek full or conditional approvals in other geographies as well. |
| • | Maximize the Commercial Value of Selinexor. We currently have global development, marketing and commercialization rights for selinexor and we are positioned to develop selinexor and to seek regulatory approval for its use in oncology indications without a collaborator in North America and Western Europe. We will evaluate potential collaborations within these geographies that enable us to further extend the selinexor development program into additional tumor types, earlier lines of therapy and additional combination regimens. We intend to enter into collaborations for further development, marketing and commercialization of selinexor in particular geographies outside of North America and Europe at an appropriate time. |
| • | Maintain Our Competitive Advantage and Scientific Expertise in the Field of Nuclear Transport. We plan to continue to conduct research in the field of nuclear transport and related areas to further our understanding of the role it plays in the underlying biology of cancer, as well other major diseases, primarily by fostering relationships with top scientific advisors and physicians. We believe that investing in the recruitment of exceptional advisors, employees and management is critical to our continued leadership in the nuclear transport field. We are collaborating with leading patient advocacy groups to provide education on the science behind our SINE compounds and to support the development and execution of clinical trials. We have advanced the understanding and potential application of selinexor to treat cancer through a broad range of collaborations with leading institutions engaged in clinical trials evaluating selinexor in the United States, Canada, Europe and Israel. |
| • | Continue Developing our Pipeline of Novel Drug Candidates. To date, we have identified several drug candidates: our oral SINE compounds selinexor (KPT-330), verdinexor (KPT-335), KPT-350 and KPT-8602 and our oral dual PAK4/NAMPT inhibitor, KPT-9274. While we may identify or in-license novel drug candidates for development in oncology in the future, we are currently focused on the development of our existing pipeline of drug candidates. |
| • | Collaborate with Key Opinion Leaders to Conduct Investigator-Sponsored Trials of Selinexor. A significant part of our strategy for continuing to efficiently assess and confirm the breadth of activity of selinexor alone or in combination with other anti-cancer drugs includes the initiation of investigator-sponsored trials. We plan to continue to facilitate the investigation of the breadth of the clinical activity of selinexor through our established network of scientific advisors and physicians. |
| • | Maximize the Value of Our Other SINE Compounds in Non-Oncology Indications through Collaborations. We may seek to enter into global or regional development, marketing and commercialization collaboration arrangements for our other SINE compounds in non-oncology indications. |
8
Table of Contents
Our Focus: Nuclear Transport
A human cell is divided into various compartments, including the nucleus and the cytoplasm. The nucleus contains a cell’s genetic material, or DNA, and is the compartment where gene expression and consequently cellular function is regulated. The cytoplasm is the compartment around the nucleus where translation of gene transcripts, or mRNA, to proteins, assembly of proteins into cellular structural elements, and cellular metabolism of fats, carbohydrates, and proteins, occur. One of the ways in which the cell regulates the function of a particular protein is by controlling the protein’s location within the cell, as a specific function may only occur within a particular location. Certain proteins, including tumor suppressor proteins and other growth regulatory proteins, need to be transported from the cytoplasm, where they are made, into the nucleus where they need to be located for their primary functions to occur. The nuclear pore is a complex gate between the nucleus and cytoplasm, closely regulating the import and export of most large molecules, called macromolecules, including many proteins, into and out of the nucleus. In healthy cells, nuclear transport processes of macromolecules in either direction through the nuclear pore is tightly regulated and requires specific carrier proteins, including nuclear export proteins, to occur. There are eight known nuclear export proteins. The most well-characterized was discovered in 1999 and is called Exportin 1, or XPO1 (also called CRM1). XPO1 mediates the export of over 220 different mammalian cargo proteins, including some growth regulatory proteins and the vast majority of tumor suppressor proteins. Moreover, XPO1 appears to be the only nuclear exporter for the majority of these tumor suppressor proteins, including those generally referred to as p53, p73, FOXO, pRB, BRCA1, BRCA2, NPM1, IkB and PP2A.
Cancer is a disease characterized by unregulated cell growth. Cancer typically develops when DNA in normal cells begins to accumulate mutations or other abnormalities, causing genes that regulate cell growth to become disrupted. Tumor suppressor proteins are an integral part of the body’s natural defense mechanism to identify and prevent cancer. When DNA damage is detected, tumor suppressor proteins promote apoptosis. Tumor suppressor proteins can also have an anti-cancer effect by dampening unregulated cell growth and division. Because tumor suppressor proteins need to be located in the nucleus in order to carry out their anti-cancer activities, their nuclear export, or exit from the nucleus, leads to their being unavailable in the nucleus to identify cancer cells and initiate their death. As XPO1 levels have been shown to be elevated by two- to four-fold in nearly all cancer cells compared to their normal cell counterparts, it appears that cancer cells have co-opted XPO1 to move tumor suppressor proteins out of the nucleus, thereby adversely affecting their ability to identify and initiate the death of cancer cells. Increased levels of XPO1 in cancer cells also lead to excessive nuclear export of growth regulatory proteins as well as oncoprotein mRNAs. All of these XPO1 effects allow cancer cells to divide continuously and inappropriately. Higher levels of XPO1 expression are also generally correlated with poor prognosis and/or resistance to chemotherapies.
In addition to transporting tumor suppressor proteins, XPO1 is the sole transporter of the eukaryotic initiation factor 4E (eIF4E) protein, also called the “mRNA cap binding protein.” eIF4E carries the mRNAs for many growth promoting proteins, including certain growth-promoting oncoproteins such as c-myc, Pim1, Atk1, hDM2 and cyclin D from the nucleus into the cytoplasm (dependent on XPO1) followed by association with ribosomes for translation into proteins. Blockade of XPO1 leads to accumulation of eIF4E in the cell nucleus and concomitant nuclear trapping of bound growth-promoting mRNAs, leading to reduced translation of these mRNAs, and reductions in their protein levels.
XPO1 is also the only exporter of the anti-inflammatory protein IkB, the inhibitor of NF-kB. NF-kB is known to play a role in cancer metastasis and resistance to chemotherapy as well as in many inflammatory and autoimmune diseases. Blockade of XPO1 leads to accumulation of IkB in the cell nucleus where it binds to and inhibits NF-kB function. SINE-mediated inhibition of NF-kB may be beneficial in overcoming chemotherapy resistance and in treating autoimmune diseases.
9
Table of Contents
The figure below depicts the process by which XPO1 mediates the nuclear transport process.
XPO1 Mediation of Nuclear Transport
Our Approach: Targeting Nuclear Export with SINE Compounds
Since the discovery of XPO1, a growing body of research has documented that the high levels of XPO1 found in cancer cells are associated with the transport of tumor suppressor and other growth regulatory proteins from their site of action in the nucleus into the cytoplasm, where their anti-cancer activity is minimal. The inhibition of XPO1 cargo binding has been studied for over ten years. XPO1 inhibitors block the nuclear export of tumor suppressor and other cargo proteins, leading to accumulation of these proteins in the nucleus and enhancing their anti-cancer activity in the cell. The forced nuclear retention of these proteins can counteract a multitude of the oncogenic pathways that allow cancer cells with severe DNA damage to continue to grow and divide in an unrestrained fashion. XPO1 inhibitors also force the nuclear retention of eIF4E and its cargo growth-promoting protein mRNAs, preventing their transport to the cytoplasm for ribosomal translation, leading to reduced levels of oncoproteins. One naturally occurring XPO1 inhibitor called leptomycin B, which must be given intravenously, has been shown to have potent anti-cancer activity in vitro, but is toxic to normal cells. These toxicities to normal cells have been observed in both animals and humans, which we believe are most likely caused by the irreversible nature of leptomycin B binding to XPO1. Because of its observed toxicities in animals and humans, to our knowledge, leptomycin B is no longer being developed.
Our lead drug candidates are first-in-class, oral Selective Inhibitor of Nuclear Export, or SINE, compounds. We have discovered SINE compounds by applying our proprietary drug discovery and optimization expertise to the published X-ray structure of XPO1. SINE compounds inhibit XPO1-mediated nuclear-cytoplasmic transport by transiently binding to the XPO1 cargo binding site, meaning that they block XPO1 cargo binding over an extended period of time, but do not permanently do so. Transient XPO1 inhibition, or inhibition for approximately 12 to 24 hours, which corresponds to the inhibition period that we have observed to date with our SINE compounds, appears to be sufficient for nuclear retention and elevation of tumor suppressor protein levels in the nucleus. During this period, the inhibition of XPO1 cargo binding enables tumor suppressor proteins to accumulate in the nucleus of cancer cells and perform their normal role of detecting DNA damage, thereby inhibiting a cancer cell’s ability to divide and promoting apoptosis. Healthy cells also build up tumor
10
Table of Contents
suppressor proteins in the presence of a SINE compound, but are able to resume normal activity after transient XPO1 inhibition because they have an intact genome with minimal or no DNA damage. The figure below depicts the process by which SINE compounds inhibit the XPO1 nuclear export of tumor suppressor proteins.
Transient XPO1 Inhibition by SINE Compounds
The XPO1-inhibiting SINE compounds that we have discovered and developed to date, including selinexor, have the potential to provide a novel targeted therapy that force tumor suppressor proteins to remain in the nucleus and promote apoptosis of cancer cells. Moreover, our SINE compounds spare normal cells, which, unlike cancer cells, do not have significant damage to their genetic material, and we believe this selectivity for cancer cells minimizes side effects. We believe that novel mechanism of action and oral administration of selinexor and the lack of cumulative or major organ toxicities observed to date in patients treated with selinexor in our Phase 1 and Phase 2 clinical trials create the potential for its broad use across many cancer types, including both hematological and solid tumor malignancies. We believe that no currently approved cancer treatments are selectively targeting the restoration and increase in the levels of multiple tumor suppressor proteins in the nucleus.
In addition to cancer, our SINE compounds have the potential to provide therapeutic benefit in a number of additional indications. Specifically, we have discovered and are developing a pipeline of SINE compounds that have shown evidence of activity in preclinical models of viral infections and neurological disorders, inflammation and autoimmune diseases.
Verdinexor (KPT-335) is our lead compound in development for the treatment of viral indications. Several viruses exclusively utilize XPO1 to shuttle cargos necessary for virion assembly such as viral ribonucleoproteins, or vRNA, and proteins from the nucleus to the cytoplasm. Verdinexor has the potential to treat viral diseases through both inhibition of viral replication and suppression of inflammatory cytokine-mediated symptoms and shows significant anti-influenza activity in murine and ferret models. In 2015, we conducted a randomized, double-blind, placebo-controlled, dose-escalating Phase 1 clinical trial of verdinexor in healthy human volunteers in Australia. This study was designed to evaluate the safety and tolerability of verdinexor in healthy adult subjects. Verdinexor was found to be generally safe and well tolerated. Mild to moderate AEs of similar number
11
Table of Contents
and grade as placebo were reported, but no serious or severe adverse events. We plan to continue the clinical development of verdinexor as a treatment for influenza. Preclinical data also show efficacy of verdinexor and related SINE compounds in additional viral models, including HIV.
KPT-350 is our lead compound in development for the treatment of neurological disorders and inflammatory and autoimmune diseases. XPO1 mediates the nuclear export of multiple proteins that impact autoimmune, inflammatory and neurodegenerative processes. Consequently, inhibition of XPO1 by KPT-350 results in a reduction in autoimmunity and inflammation and an increase in anti-inflammatory and neuroprotective responses. KPT-350 penetrates the blood brain barrier to a greater degree than other SINE compounds. Preclinical data generated largely by external collaborators show efficacy of orally-administered KPT-350 and related SINE compounds in animal models of amyotrophic lateral sclerosis, or ALS, multiple sclerosis, or MS, systemic lupus erythematosus, or lupus, rheumatoid arthritis, or RA, and traumatic brain injury, or TBI.
Our Initial Indication: Cancer
Cancer is a leading cause of death worldwide, with approximately 8.2 million cancer deaths globally in 2012, according to the American Cancer Society. In the United States, the American Cancer Society estimates that in 2016, approximately 596,000 people will die of cancer and approximately 1.7 million new cancer cases will be diagnosed. The International Agency for Research on Cancer projects that in 2030, 21.6 million people will be diagnosed with cancer, and 13 million people will die of cancer worldwide, as compared to 14.1 million new cancer diagnoses and 8.2 million cancer deaths worldwide in 2012.
The most common methods of treating patients with cancer are surgery, radiation and drug therapy. A cancer patient often receives treatment with a combination of these methods. Surgery and radiation therapy are particularly effective in patients in whom the disease is localized. Physicians generally use systemic drug therapies in situations in which the cancer has spread beyond the primary site or cannot otherwise be treated through surgery. In many cases, drug therapy entails the administration of several different drugs in combination. An early approach to cancer treatment was to develop drugs, referred to as cytotoxic drugs, that kill rapidly proliferating cancer cells through non-specific mechanisms, such as disrupting cell metabolism or causing damage to cellular components required for survival and rapid growth. While these drugs have been effective in the treatment of some cancers, they act in an indiscriminate manner, killing healthy cells, as well as cancer cells. Due to their mechanism of action, many cytotoxic drugs have a narrow dose range above which the toxicity causes unacceptable or even fatal levels of damage and below which the drugs are not effective in promoting cancer cell death. A different approach to pharmacological cancer treatment has been to develop drugs, referred to as targeted therapeutics, that target specific biological molecules in the human body that play a role in rapid cell growth and the spread of cancer. Targeted therapeutics are designed to specifically enable the death of cancer cells and spare normal cells, to improve efficacy, and to minimize side effects. The drugs are designed to either attack a target that causes uncontrolled growth of cancer cells because of either a specific genetic alteration primarily found in cancer cells, but not in normal cells, or a target that cancer cells are more dependent on for their growth in comparison to normal cells.
Our SINE compounds are novel therapies specifically designed to force nuclear localization and elevation in the levels of multiple tumor suppressor and growth regulatory proteins. Tumor suppressor proteins assess a cell’s DNA and in cells, like most cancer cells, with heavily damaged DNA, these proteins induce cell death, or apoptosis. Unlike many other targeted therapeutic approaches which only work for a specific set of cancers or in a specific sub-group of patients, we believe that by restoring tumor suppressor proteins to the nucleus where they can assess a cell’s DNA, our SINE compounds have the potential to provide therapeutic benefits across a broad range of both hematological and solid tumor malignancies and benefit a wide range of patients. Additionally, and further supported by its mechanism of action and supported by preclinical and clinical data, we believe that selinexor has the potential to be additive or synergistic with approved and experimental therapies in treating many of these cancer patients. As a result, we believe that selinexor has the potential to serve as a backbone therapy across multiple hematological and solid tumor malignancies as part of a variety of combination therapies.
12
Table of Contents
Our Oncology Drug Candidates
Selinexor (KPT-330)
Selinexor is being evaluated in multiple later phase clinical trials in patients with relapsed and/or refractory hematological malignancies and solid tumors. Anti-cancer activity has been observed with tumor reductions and durable disease control across many hematologic malignancies and solid tumors. Over 20 patients have remained on single-agent oral selinexor for over 12 months with some patients on therapy for over 24 months. Adverse events observed in our most recent patient data are generally mild to moderate, responsive to standard supportive care, often decrease over time and are consistent with those previously reported in patients in our Phase 1 clinical trials.
We have determined that the recommended Phase 2 dose of selinexor in most settings is 60mg dosed twice weekly. In December 2015, we and our collaborators presented an analysis of our Phase 1 clinical data in hematological malignancies at the American Society of Hematology, or ASH, Annual Meeting. The analysis demonstrated that doses of selinexor from 45-65mg (median 60mg) were better tolerated than doses greater than 65mg and showed less weight loss, lower incidence of high grade adverse events and greater numbers of days on study. 266 heavily pretreated patients with multiple myeloma, or MM, non-Hodgkin’s lymphoma, or NHL, acute myeloid leukemia, or AML, and other hematological malignancies were included in the analysis and divided into three groups of evaluable patients: those that received 4-44mg (median 30mg), those that received 45-65mg (median 60mg) and those that received greater than 65mg (70-160mg; median 90mg) for comparison of safety and efficacy endpoints. Patients in the 4-44mg and 45-65mg groups remained on study longer than those receiving greater than 65mg, with average treatment duration of 120 days in the first two groups versus 90 days in the highest dose group, respectively. Overall efficacy was numerically superior in the 45-65mg dose group across multiple hematologic indications. The most common adverse events, or AEs, were nausea (63%), fatigue (62%), anorexia (57%), vomiting (38%), which were mostly grade 1/2, and thrombocytopenia (41%), which was mostly grade 3/4, but with very low incidents of bleeding. The incidence of certain selinexor-related high grade (3/4) AEs was lower in patients receiving 45-65mg selinexor as compared to those receiving greater than 65mg. These data from our extensive Phase 1 experience with selinexor are consistent with our belief that a flat dose of 60mg is the most appropriate selinexor dose for both efficacy and tolerability in most settings. However, as is the case for many other anti-cancer drugs, certain indications would likely be treated with different doses.
A preliminary analysis of safety and tolerability of selinexor was performed on unaudited AE data for 730 patients enrolled in our company-sponsored hematological malignancy and solid tumor clinical trials as of the data cutoff point of May 31, 2015. The most commonly reported AEs of all grades that were considered related to selinexor were gastrointestinal in nature: nausea (55%), fatigue (54%), anorexia (43%), and vomiting (35%). The most commonly reported AEs that were Grade 3 included nausea (4%), fatigue (12%), anorexia (4%), and vomiting (3%). Overall, the AE profiles for hematologic malignancy studies and solid tumor studies are similar. Rates of Grade 3 and Grade 4 thrombocytopenia were higher in patients with hematologic malignancies than with solid tumors (thrombocytopenia: 25% vs. 9%) and (neutropenia: 14% vs. 4%), respectively.
We describe below the key company- and investigator-sponsored studies evaluating selinexor in hematological malignancies and solid tumors, both as a single-agent and in combination. Additional data from company- and investigator-sponsored combination studies may be presented on an ongoing basis by us and/or our collaborators at scientific conferences or through other publications at various times. We expect such data will continue to inform our Phase 2 and Phase 3 dosing for selinexor in these combinations and allow us to evaluate the combinations with the greatest potential for durable responses and increased survival. Response data presented herein are interim unaudited data based on reports by physicians at the clinical trial sites. Responses in hematological trials are measured using commonly accepted evaluation criteria for the specific indication. Responses in solid tumor trials are evaluated using RECIST unless otherwise noted.
13
Table of Contents
Advanced Hematological Malignancies
Multiple Myeloma
MM is a hematological malignancy characterized by the accumulation of monoclonal plasma cells in the bone marrow, the presence of monoclonal immunoglobulin, or M protein, in the serum or urine, bone disease, kidney disease and immunodeficiency. It is more common in elderly patients, with a median age at diagnosis of 65-70 years. In the United States, the American Cancer Society estimates that there will be approximately 30,000 new cases of MM, with about 12,700 attributable deaths, in 2016. The World Health Organization estimated that approximately 114,000 new cases of MM were diagnosed worldwide in 2012.
The treatment of MM has improved in the last 20 years due to the use of high-dose chemotherapy and autologous stem cell transplantation, which is restricted to healthier, often younger patients, and the subsequent introduction of the immunomodulatory agents, or IMiDs, such as lenalidomide (Revlimid®) and pomalidomide (Pomalyst®) and the proteasome inhibitors, or PIs, bortezomib (Velcade®), carfilzomib (Kyprolis®), and ixazomib (Ninlaro®). Two monoclonal antibodies, daratumumab (Darzalex™) and elotuzumab (Empliciti™), have also recently been approved, as has the histone deacetylase inhibitor panobinostat (Farydak®). The introduction of non-chemotherapeutic agents has led to a significant increase in the survival of patients with MM. Although a wide variety of newly approved or experimental therapies are being used in relapsed and/or refractory patients, including new proteasome inhibitors (oprozomib and marizomib), monoclonal antibodies and cellular therapies like chimeric antigen receptor T-cell, or CAR-T, therapy, nearly all patients will eventually relapse and succumb to their disease. With around 37,000 deaths from MM in the United States and Europe expected, we believe that there remains a need for therapies for patients whose disease has relapsed after, or is refractory to, available therapy.
STORM: Phase 2b Clinical Trial of Selinexor and Low-Dose Dexamethasone in Multiple Myeloma
In May 2015, we initiated a Phase 2b clinical trial evaluating selinexor and low-dose dexamethasone, or low-dose dex, in patients with heavily pretreated MM. The Selinexor Treatment of Refractory Myeloma, or STORM, study is a single-arm study evaluating the treatment of relapsed/refractory MM with 80mg of selinexor and 20mg of dexamethasone, each dosed twice weekly. This 40mg per week dose of dexamethasone is considered “low dose” in the treatment of MM, compared with the “high dose” dexamethasone which uses three times more of the steroid. Under the latest protocol version, we are enrolling patients to STORM who (i) have been exposed to bortezomib and carfilzomib, each of which is a PI, and lenalidomide and pomalidomide, each of which is an immunomodulatory agent, or IMiD, and (ii) has disease refractory to at least one PI and one IMiD. Prior treatment regimens must have also included an alkylating agent, such as melphalan and/or cyclophosphamide, and a glucocorticoid, such as dexamethasone.
In November 2015, the U.S. Food and Drug Administration, or FDA, approved daratumumab (Darzalex™), an anti-CD38 monoclonal antibody to treat patients with MM who received at least three prior lines of therapy, including a PI and an IMiD or whose disease is double refractory to a PI and an IMiD. As a result, we are seeking to increase the proportion of patients enrolling on the STORM study whose disease is also refractory to an anti-CD38 monoclonal antibody like daratumumab. Patients enrolled under all protocol versions are evaluable for efficacy and will be included in the evaluation of the first cohort of 80 patients on the STORM study.
The primary endpoint of the STORM study is overall response rate, or ORR, meaning partial response, or PR, or better. The trial has several secondary endpoints, including ORR in patients whose disease is relapsed/refractory to an anti-CD38 monoclonal antibody and duration of response, or DOR. We expect data from the first 80 patients on the STORM study to be available in the middle of 2016, at which point we will evaluate whether to expand the study to an additional cohort of patients and whether such expansion, together with promising data, could potentially serve as the basis for an application seeking accelerated regulatory approval.
14
Table of Contents
SCORE: Phase 2/3 Clinical Trial of Selinexor, Carfilzomib and Low-Dose Dexamethasone vs. Carfilzomib and Low-Dose Dexamethasone in Multiple Myeloma
We expect to initiate a Phase 2/3 clinical trial in the middle of 2016 to evaluate oral selinexor in combination with carfilzomib and low-dose dex in refractory MM patients. The study, titled Selinexor, Carfilzomib, and Dexamethasone versus Placebo, Carfilzomib, and Dexamethasone in Relapsed/Refractory Multiple Myeloma, or SCORE, is a Phase 2/3 randomized, double-blinded clinical trial. Following FDA feedback, we have revised our clinical trial design for SCORE to evaluate patients with relapsed and/or refractory MM who are refractory to an IMiD. We will evaluate 60mg of selinexor twice weekly in combination with low-dose dex and carfilzomib compared to a control therapy of carfilzomib and low-dose dex in this patient population. We expect to dose selinexor twice weekly at 60mg during the first three weeks of each four-week cycle. Based on tolerability, the selinexor dose may be increased to 80mg on the same dosing schedule following at least one cycle at 60mg. Carfilzomib is expected to be administered intravenously twice weekly for the first three weeks of each four-week cycle and then twice every other week beginning on cycle 14 and successive cycles thereafter. Dexamethasone is expected to be dosed at 20mg twice weekly with patients having partial intolerance to glucocorticoids permitted to receive a reduced dose of 10mg twice weekly. We expect that patients who progress on the control arm of the SCORE study will be permitted to crossover to receive the selinexor, carfilzomib and low-dose dex regimen. Approximately 84 patients are expected to be enrolled in the Phase 2 portion of the SCORE study, which will have a primary endpoint of ORR. The primary endpoint of the Phase 3 portion of the study is to compare progression free survival, or PFS, in patients treated with selinexor, carfilzomib and low-dose dex versus patients treated with placebo, carfilzomib and low-dose dex. We expect top-line data from the Phase 2 portion of this study in the middle of 2017.
The clinical rationale and study design for SCORE are based in part on preliminary data from an ongoing Phase 1 investigator-sponsored study led by the University of Chicago and supported by a collaboration between Karyopharm, Onyx Pharmaceuticals (owned by Amgen Inc.) and the Multiple Myeloma Research Consortium. This study is evaluating the tolerability and efficacy of the combination of selinexor with carfilzomib and low-dose dex in patients with very heavily pretreated MM. The primary objectives of the study are to determine the maximum tolerated dose, or MTD, and recommended Phase 2 and Phase 3 doses for selinexor in these combination therapies in the dose-escalation phase and to assess preliminary efficacy through ORR, clinical benefit rate, or CBR, and duration of response, or DOR, in the expansion phase. The dose escalation phase in this clinical study is ongoing.
Preliminary data as of September 30, 2015 from nine evaluable study patients from a Phase 1 investigator-sponsored study were presented in December 2015 at the ASH Annual Meeting. These nine patients received a median of four prior treatment regimens and all patients received carfilzomib-based treatments to which their MM became refractory. Seven of the nine patients had MM that was refractory to a carfilzomib regimen as their last therapy prior to enrolling on the study. Eight patients received 30 mg/m2 (approximately 50mg) of selinexor in combination with either 20/27 mg/m2 or 20/36 mg/m2 of carfilzomib and one patient received a 60mg flat dose of selinexor in combination with 20/27 mg m2 of carfilzomib. Dexamethasone was dosed at either 20mg or 10mg twice weekly.
Six out of the nine evaluable patients (67%) achieved a PR or better and two of such responders (22%) achieved a very good partial response, or VGPR. Seven out of nine patients (78%) had at least a minor response, or MR. Responses occurred rapidly within the first one-to-two cycles. Five of the seven (71%) patients whose MM was refractory to carfilzomib in their last prior therapy responded with a PR or better. Median time on study was four months with a range of 0.5 to 13 months. Three patients, including the patient on study for 13 months, remained on study as of September 30, 2015. No unexpected toxicities were observed and no patients left the study due to AEs. Seven patients were evaluable for dose limiting toxicity, or DLT, and no DLTs were reported. A maximum tolerated dose, or MTD, has not yet been established, and none of the patients discontinued the study due to AEs. The AEs were reversible and manageable with supportive care. Grade 3/4 AEs were predominantly hematological and included thrombocytopenia (67%), neutropenia (44%),
15
Table of Contents
lymphopenia (22%) and anemia (22%). The most common grade 3/4 non-hematologic AE was fatigue (22%).The study continues to enroll to determine the MTD of selinexor in combination with carfilzomib and low-dose dex and to better understand tolerability and efficacy of the combination at the MTD.
STOMP: Phase 1b/2 Clinical Trial of Selinexor in Combination with Backbone Therapies in Multiple Myeloma
Based on preclinical synergy in animal models of MM, in October 2015, we initiated a Phase 1b/2 clinical study of selinexor in combination with backbone treatments for relapsed/refractory MM. In this multi-arm study, Selinexor and Backbone Treatments of Multiple Myeloma Patients, or STOMP, we are evaluating the combination of selinexor and low-dose dex with backbone therapies pomalidomide, bortezomib or lenalidomide in patients with previously treated MM. Each combination is evaluated on a separate arm of the STOMP study and within each combination, two treatment cohorts will evaluate once weekly versus twice weekly dosing of selinexor.
We plan to enroll up to 200 patients with MM in this study, with up to 85 patients on the Phase 1 dose-escalation portion of the study and approximately 115 patients on the Phase 2 expansion phase. The primary objectives of the Phase 1 portion are to determine the maximum tolerated dose and recommended Phase 2 and Phase 3 doses for selinexor in these combination therapies. The primary objectives of the Phase 2 portion are to assess preliminary efficacy through ORR, CBR and DOR. We expect to determine the recommended Phase 2 and Phase 3 trial doses for selinexor in the first of these three combinations in late 2016.
Investigator-Sponsored Clinical Trials
In addition to the investigator-sponsored trial of selinexor, carfilzomib and low-dose dex led by the University of Chicago, other investigator-sponsored studies are evaluating the safety and efficacy of selinexor in combination with existing therapies to treat MM: (i) pegylated liposomal doxorubicin and selinexor and (ii) bortezomib, low-dose dex and selinexor for induction and consolidation.
Company-Sponsored Phase 1 Clinical Trial Data
As part of our Phase 1 clinical trial of selinexor in patients with advanced hematological malignancies, patients with MM were treated with either single-agent selinexor or selinexor in combination with low-dose (20mg) dexamethasone, all dosed twice weekly. As of December 6, 2015, 12 evaluable patients were treated with 45mg/m2 of oral selinexor and 20mg of dexamethasone, each dosed twice weekly. This dose of selinexor, equivalent to approximately 80mg, was determined to be the recommended Phase 2 and Phase 3 dose for this combination therapy as higher doses like 60 mg/m2 were not well tolerated. While the recommended phase 2 dose of selinexor in most settings is 60mg twice weekly, the addition of a steroid like dexamethasone in the multiple myeloma setting allows for higher dosing of selinexor. Additionally, this dose of dexamethasone is the standard low-dose dexamethasone (40mg weekly or 20mg twice weekly) used with nearly all other anti-myeloma drugs. The patients enrolled in this study had received a median of seven prior lines of therapy, each line typically consisting of two to four separate anti-myeloma agents. All had received prior therapy with at least one PI, such as carfilzomib or bortezomib, and at least one IMiD, such as lenalidomide or pomalidomide, and steroids (typically two or more times).
As of December 6, 2015, the best responses among the 12 evaluable patients were one stringent complete response, or sCR (8%), seven PRs (58%), two MRs (17%) and two PD (17%). Two patients left the trial before disease assessment and were therefore not evaluable for response. The clinical benefit rate (sCR+PRs+MRs) was 83% and the ORR (sCR+PRs) was 67%. The median duration of response is approximately seven months and the longest response lasted over one year. AEs in patients receiving single-agent selinexor were generally low-grade, consistent with events observed in patients with other hematological malignancies and responsive to standard supportive care. Compared with selinexor given alone, fewer AEs in patients receiving selinexor in combination with low-dose dexamethasone were reported, particularly levels of nausea, vomiting and weight loss. These observations are consistent with dexamethasone’s expected reduction in nausea, anorexia and fatigue, which are selinexor’s primary constitutional side effects.
16
Table of Contents
Acute Myeloid Leukemia
AML in elderly populations remains a vexing clinical problem with little progress in the last decade. There are no treatment agents specifically approved for this population in the United States. AML is a cancer that starts in the bone marrow and in most cases quickly moves into the blood. The incidence of AML dramatically increases after the age of 55. The American Cancer Society estimates that approximately 20,000 new cases of AML, most of which will be in adults, will be diagnosed in the United States in 2016, with approximately 10,400 deaths from AML in the United States in 2016. Approximately 40% of AML patients are young enough with sufficient major organ function to undergo stem cell transplantation for their AML, and approximately 50% of these patients can be cured of their disease. Therefore, approximately 20% of adults with AML are currently curable. Those who are not cured, and those patients who are elderly or unfit for transplant, have a very poor prognosis with a median survival of less than one year. Moreover, prognosis worsens continuously with advancing age to a median survival of as low as one month for those who are older than 85 years of age.
Over the past two decades, many compounds have been evaluated in elderly patients with AML, but due to significant toxicities and/or lack of efficacy, none has been approved to date in the United States. Adults who are not transplant candidates, and cannot safely receive intensive chemotherapy, such as anthracyclines and cytosine arabinoside, or Ara-C (often referred to as the “7+3” regimen), are usually treated with best supportive care, or BSC, including blood transfusions, antibiotics and hydroxyurea if indicated, along with hypomethylating agents decitabine (Dacogen®) or azacytidine (Vidaza®). These hypomethylating agents are approved in certain AML populations in the European Union. Some patients are treated with “low dose” Ara-C. All of these agents are given parenterally (subcutaneously or intravenously) in the clinic or hospital, and none of these agents are associated with cures, meaning that all older patients unfit for chemotherapy will relapse and eventually succumb to their disease. Median survival following initial treatment with front-line therapy in these patients is reported to be less than three months.
SOPRA: Phase 2 Clinical Trial of Selinexor vs. Physician’s Choice in Elderly AML
Our Phase 2 study of selinexor in patients 60 years of age or older with relapsed or refractory AML continues to enroll patients who are ineligible for standard intensive chemotherapy and/or transplantation. In our Selinexor in Older Patient with Relapsed/Refractory AML, or SOPRA, study we are evaluating approximately 170 patients who have AML that has relapsed after, or was refractory to, first line therapy. Patients are randomized in a 2:1 fashion to selinexor provided orally twice weekly in a dose of 60mg plus BSC versus one of three physician choices. Patients must have received at least one prior line of AML therapy given at standard doses and must have progressed after their most recent therapy. Prior therapy must have included at least two cycles of a hypomethylating agent. Physician choices include (i) BSC alone, (ii) BSC plus either azacytidine or decitabine or (iii) BSC plus low-dose Ara-C. Overall survival is the primary endpoint. The SOPRA study was designed based on data from the Phase 1 study of selinexor in patients with advanced hematologic malignancies, including AML.
In July 2015, we lowered the dose of selinexor given on the SOPRA study to 60mg twice weekly after reviewing adverse event data that showed that the rate of sepsis in patients receiving 55 mg/m2 of selinexor (approximately 100mg) was eight cases in 70 patients (11%) as compared to two cases in 30 patients (6.7%) on the physician’s choice arm. Although this trend was not statistically significant, we reviewed all Phase 1 data across indications and found that doses of selinexor greater than 80mg were associated with increased sepsis rates only in patients with heavily pretreated AML. The Phase 1 and Phase 2 results across other hematologic malignancies and solid tumors showed no increase in sepsis. Unfortunately, patients with AML are more susceptible to sepsis due to severe immune compromise and existing therapies show similar rates of sepsis (between 12-25%) compared to high dose (100mg) selinexor. Importantly, doses of 60mg twice weekly do not appear to be associated with any increase in sepsis-related events in patients with AML. In addition, the majority of the patients with AML in the Phase 1 study who showed a response to selinexor treatment, including patients with complete remissions with full platelet and neutrophil recovery, received selinexor at doses of approximately
17
Table of Contents
60mg or below. Based on these observations, we believe that the dose reduction has been effective in reducing sepsis rates without compromising efficacy in the SOPRA study.
In August 2015, we elected to amend the protocol for the SOPRA study to reflect our decision to reduce the study dose. The protocol provides for an interim analysis following a defined number events, or deaths, of patients enrolled on that version or a subsequent version of the protocol. Following that number of events, the data are analyzed to allow the study’s data safety monitoring board, or DSMB, to review the results of the interim analysis and provide us with the recommendation of stopping the trial for significant efficacy or futility, continuing the study as currently planned or increasing the size of the study. We currently expect this interim analysis to occur in late 2016, but the timing of the analysis depends on the survival of patients. A predetermined number of events are required to analyze the primary efficacy endpoint of overall survival, or OS. The sample size of the study is designed to have 80% power to detect an improvement in the median OS of the selinexor arm of approximately 5.2 months versus the physician’s choice arm of approximately three months. We expect to report top-line data from the SOPRA study in the middle of 2017.
Investigator-Sponsored Trials
SAIL: Phase 2 Clinical Trial of Selinexor, Ara-C and Idarubicin in AML
In December 2015, Walter Fiedler, MD of the University Medical Center Hamburg-Eppendorf in Germany and his colleagues presented preliminary data from the SAIL study, an investigator-sponsored trial evaluating the combination of selinexor, Ara-C and idarubicin in patients with relapsed/refractory AML. Patients in this study had a range of one to six prior therapies and 35% had undergone a prior stem cell transplant or donor lymphocyte infusion. Data from 20 evaluable patients showed that 12 patients (60%) responded to therapy, with nine patients (45%) experiencing CR with neutrophil and platelet recovery, one patient (5%) experiencing CR without recovery, and two patients achieving PRs. Remissions ranged from 71 to 305 days with the median remission equal to 206 days.
The most frequent non-hematologic AEs were vomiting, diarrhea, nausea, fatigue, anorexia and neutropenic fever, which are commonly observed with standard Ara-C and idarubicin treatment itself. One treatment-related death occurred wherein a patient with grade 4 thrombocytopenia developed a subarachnoid hemorrhage, which is common in relapsed AML due to intensive chemotherapy and is a less frequent consequence of single-agent selinexor treatment. Other Ara-C-based combination therapies for AML have shown significantly lower response rates in patients with heavily pretreated AML: combination of Ara-C with gemtuzumab ozogamicin (Mylotarg®) – 11.5% ORR; combination of Ara-C with doxorubicin (Doxil®) – 6.9%. We believe the combination of selinexor with chemotherapy is a promising regimen, particularly in this difficult-to-treat patient population with poor prognoses. The majority of patients on the SAIL study were able to proceed to their first or second allogeneic stem cell translation. Ara-C and idarubicin represent the standard of care for AML patients who are candidates for intensive therapy and the SAIL study provides support for the tolerability of selinexor in combination with standard of care therapy. Accordingly, we believe these data support the continued development of selinexor with intensive chemotherapeutic regimens in AML, including in the relapsed/refractory or front-line setting.
Additional investigator-sponsored studies are evaluating the safety and efficacy of selinexor as a single agent and in combination with existing therapies: (i) daunorubicin, cytarabine and selinexor in patients with high risk, naïve AML, (ii) topoisomerase-II inhibition and selinexor in AML, (iii) sorafenib and selinexor in AML, (iv) cladribine and cytarabine, or CLAG, and selinexor in AML, (v) high dose cytarabine, or HiDAC, mitoxantrone chemotherapy and selinexor for remission induction in AML, (vi) decitabine and selinexor in AML, (vii) fludarabine, cytarabine and selinexor in pediatric patients with relapsed/refractory leukemia or myelodysplastic syndrome, or MDS, (viii) single-agent selinexor to eliminate minimal residual disease and maintain remission in patients with AML and high risk MDS after allogenic stem cell transplant and (ix) single-agent selinexor in MDS.
18
Table of Contents
Company-Sponsored Phase 1 Clinical Trial Data
In December 2015, we presented data, based on 95 patients with AML enrolled on our Phase 1 study as of December 6, 2015, of which 78 were evaluable for response. These patients were heavily pretreated with progressive, relapsed and/or refractory AML, most with three or more prior treatment regimens. These patients typically received between 16.8-70mg/m2 of selinexor in a four-week cycle, with lower doses initially given ten times per cycle and higher doses given twice weekly. Of these 78 evaluable patients, the complete response rate with or without full hematologic recovery was 10%. Forty-five patients (58%) experienced SD and the disease control rate across the evaluable patients was 68% (53 of 78 patients). Responses were observed across multiple genetic subtypes of AML. Higher doses of selinexor were associated with greater reductions in bone marrow blast counts, which were also observed across different AML subtypes.
Non-Hodgkin’s Lymphoma
Non-Hodgkin’s lymphoma, or NHL, is a cancer that starts in cells called lymphocytes, which are part of the body’s immune system. Lymphocytes are found in the lymph nodes and other lymphoid tissues, such as the spleen and bone marrow, as well as in the blood. The World Health Organization estimated that approximately 386,000 new cases of NHL would be diagnosed worldwide in 2012 and the American Cancer Society projects that approximately 72,600 patients will be diagnosed with NHL in the United States in 2016.
SADAL: Phase 2b Clinical Trial of Low vs. High Dose Selinexor in Diffuse Large B-Cell Lymphoma
Diffuse Large B-Cell Lymphoma, or DLBCL, is the most common of the aggressive NHLs. We estimate that approximately 22,000 patients are diagnosed with DLBCL in the United States each year, with approximately 10,000 deaths per year. The fundamental treatment of DLBCL has changed little in the past two decades, with no new or targeted agents approved for this indication. Initial therapy with multi-agent cytotoxic drugs in combination with the monoclonal antibody rituximab (Rituxan®), most often in a combination therapy known as “R-CHOP,” leads to cures in approximately 50% of patients. Patients who are not cured with initial immune-chemotherapy have a poor prognosis. Of the approximately 30% of patients who are less than 65 years old and have good organ function, high dose chemotherapy with stem cell transplantation can lead to cures in up to half. Older patients relapsing after initial chemotherapy, and those relapsing after stem cell transplantation, have a very poor prognosis, and the expected survival of such patients is less than one year. Newer targeted agents such as the BTK inhibitor ibrutinib (Imbruvica®) and the immunomodulatory drug lenalidomide (Revlimid®) have shown some activity in the immunoblastic (activated B-cell or ABC) type of DLBCL in clinical trials, but responses are generally short. Responses to these newer agents are much lower in the germinal center, or GCB, type of DLBCL. Therefore, with 10,000 deaths in United States each year due to DLBCL, we believe that novel, well-tolerated drugs are needed for the treatment of relapsed/refractory DLBCL.
Our Selinexor Against Diffuse Aggressive Lymphoma, or SADAL, study, a two-arm, open-label Phase 2b clinical trial, continues to enroll patients that have relapsed and/or refractory DLBCL, either de novo or transformed from a more indolent NHL such as follicular lymphoma, after two to five lines of therapy with at least 14 weeks since the last systemic anti-DLBCL therapy. There are two arms in the study: 100mg versus 60mg of selinexor, each given twice weekly, with about 200 patients randomized evenly between the two arms. At least 50% of patients on SADAL will have the GCB subtype of DLBCL, which represents a particularly high unmet medical need given the lack of available therapies for patients with this relapsed/refractory subtype. The primary endpoint of this trial is ORR on each arm, with the goal of determining the more optimal dose for patients with heavily pretreated DLBCL. We currently expect to report top-line data from this study in early 2017.
In November 2014, we initiated a Phase 2 clinical trial known as Selinexor in Relapsed/Refractory Richter’s Transformation, or SIRRT. This is a single-arm, open-label trial in patients who experienced Richter’s transformation, a transformation from chronic lymphocytic leukemia, or CLL, to a type of NHL that is
19
Table of Contents
similar to DLBCL and is characterized by a distinct worsening of symptoms. SIRRT was initially open only to patients who relapsed after being treated with chemotherapy for Richter’s transformation. The inclusion criteria were subsequently expanded to enroll patients who had not received a prior therapy after experiencing Richter’s transformation. Nonetheless, enrollment in the study remains very slow, due in large part to the very rapid progression of the disease following the diagnosis of Richter’s transformation. Many patients were not able to survive long enough to complete screening for the study. In light of the enrollment difficulties and the low incidence of Richter’s transformation, we have decided to reduce the number of active clinical sites on the SIRRT study. We intend to keep the study open in order to allow patients with Richter’s transformation an avenue for selinexor treatment, but will reallocate most of the resources designated for the SIRRT study to other clinical priorities.
Future clinical studies for selinexor in NHL may include randomized studies comparing selinexor to standard of care chemotherapy regimens.
Investigator-Sponsored Trials
Investigator-sponsored clinical trials are evaluating the safety and efficacy of selinexor in combination with existing therapies to treat various lymphomas: (i) rituximab, ifosfamide, carboplatin and etoposide, or R-ICE, and selinexor to treat DLBCL and (ii) ibrutinib and selinexor to treat CLL or NHL.
Company-Sponsored Phase 1 Clinical Trial Data
As of June 1, 2015, 77 heavily pretreated patients with relapsed and/or refractory NHL were enrolled in our Phase 1 clinical trial for selinexor. Of this group, 67 patients were evaluable for response. The DCR was 67% across all doses of selinexor and the ORR was 33%. Responses were observed across all subtypes of NHL, independent of genetic abnormalities, with durable cancer control observed across several patients who remained on study for longer than nine months, with the longest remaining on study for over 24 months.
Among the 41 patients with heavily pretreated DLBCL who were evaluable as of June 1, 2015, ORR and DCR were similar across the two major subtypes of DLBCL, namely GCB and ABC, also called non-GCB. Many targeted therapies such as ibrutinib or lenalidomide show activity primarily against the ABC subtype (although all patients relapse), but there are no viable treatment options for patients with relapsed/refractory GCB. However, consistent with the broadly applicable mechanism of action of selinexor, selinexor showed activity across both major subtypes of DLBCL with DCR equal to 60% and 40% between the GCB and non-GCB subtypes, respectively, and ORR equal to 35% and 20% between the GCB and non-GCB subtypes, respectively.
In addition, a minority of DLBCL patients have “double-hit” disease because these tumors over-express the two oncogenes MYC and BCL2 (or BCL6). Double-hit DLBCL is particularly difficult to treat due in part to its resistance to multi-agent immunochemotherapy and many targeted agents. Essentially all patients with double-hit DLBCL will relapse after initial therapy, or have tumors that fail to respond (i.e., are refractory) to initial and subsequent therapies. Of five patients with double-hit DLBCL as of June 1, 2015, there was one patient with a CR (on study 589 days), two patients with PRs, one on study for 214 days and the other on study for 91 days before going to transplant, and two patients who progressed. We believe that these data and the consistent data across DLBCL subtypes indicate that selinexor has the potential to treat a broad range of subtypes of DLBCL, largely independent of the cell of origin or oncogenic drivers.
Advanced or Metastatic Solid Tumor Malignancies
Solid tumors represent the vast majority of cancer incidences. The International Agency for Research on Cancer estimates that approximately 13.1 million adults were diagnosed with solid tumor malignancies worldwide in 2012. Given this large patient population and the mechanistic activity of selinexor that makes it potentially suitable for treating any type of cancer, we are developing selinexor to potentially play a meaningful
20
Table of Contents
role across multiple solid tumor indications, either alone or in combination as a backbone therapy. We have seen encouraging single agent data for selinexor in a variety of solid tumors including PRs and durable SD with disease control greater than three months. Our Phase 1b study in patients with liposarcoma and other sarcomas demonstrated durable stable disease with single-agent selinexor and our Phase 2 studies of selinexor in gynecological malignancies and glioblastoma multiforme, or GBM, also demonstrated anti-cancer activity and disease control. Given the promising single-agent activity in difficult-to-treat indications and the potential to enhance activity in combination with existing therapies, we plan to seek opportunities in unmet needs like endometrial cancer, GBM and KRAS gene mutated colorectal cancer, and to advance combination therapy development with both standard of care and emerging therapies like immune checkpoint inhibitors.
SEAL: Phase 2/3 Clinical Trial of Selinexor vs. Placebo in Liposarcoma
Liposarcoma represents an area of high unmet need with limited treatment options. Liposarcoma arises from fat cells or their precursors and, according to the nonprofit organization the Sarcoma Alliance for Research through Collaboration (SARC), represents 18% of all soft tissue sarcoma, or an estimated 2,500 new cases per year in the United Sates. We estimate that approximately 18,000 people in the United States suffer from liposarcoma. Liposarcoma most commonly occurs in the thigh, behind the knee, the groin, the gluteal area or behind the abdominal cavity. Soft tissue sarcomas can invade surrounding tissue and can spread to other organs of the body. Dedifferentiated liposarcoma is an aggressive form of soft tissue sarcoma that is resistant to both standard chemotherapy and radiation. Liposarcoma has a particularly high rate of recurrence following surgery, especially in cases involving the abdomen. Except for cases that are cured with surgery, most patients with liposarcoma will succumb to this disease, and novel therapies are needed.
In our Phase 1b trial to evaluate the effects of food and formulation on selinexor pharmacokinetics in patients with soft-tissue or bone sarcoma, 31 of 54 sarcoma patients (57%) experienced SD with single-agent selinexor treatment. Of the 18 patients with liposarcoma, 14 (78%) experienced SD and eight (44%) experienced SD of four months or longer. Fifteen of these 18 patients with liposarcoma had dedifferentiated liposarcoma. Of these 15 patients with dedifferentiated liposarcoma, 13 (87%) experienced SD and seven (47%) experienced SD of four months or longer. In addition, in patients with previously treated liposarcoma, progression free survival, or PFS, on selinexor was longer than the patient’s most recent anti-cancer regimen.
In light of the Phase 1b data, we designed the Selinexor in Advanced Liposarcoma, or SEAL, study, a multi-center, randomized, double-blind, placebo-controlled Phase 2/3 clinical trial evaluating single-agent oral selinexor in patients with advanced unresectable dedifferentiated liposarcoma who received at least one line of prior systemic therapy. Patients will be randomized to receive either 60mg of selinexor or placebo given twice weekly until progression or intolerability. Fifty patients are expected to be enrolled in the Phase 2 portion of the study, with the potential to increase enrollment in the Phase 3 portion following an interim analysis. The study design including the primary endpoint of PFS was acceptable to the FDA and will be evaluated for futility in an interim analysis of the Phase 2 portion of this study, which we expect to occur during the middle of 2017.
SIGN: Phase 2 Clinical Trial of Selinexor in Gynecological Malignancies
The SIGN study is a Phase 2, open-label study of efficacy and safety of selinexor in patients with heavily pre-treated, progressive gynecological cancers. In May 2015, we presented data at the American Society of Clinical Oncology (ASCO) Annual Meeting that showed selinexor’s promising anti-tumor activity and disease control across various heavily pretreated gynecological malignancies. As of May 10, 2015, selinexor demonstrated single-agent anti-cancer activity in patients with ovarian and endometrial cancers with disease control rates, meaning the percentage of patients experiencing (i) an objective response, meaning CR or PR, of 12% in patients with ovarian cancers and 17% in patients with endometrial cancers or (ii) at least 12 weeks of SD, of 55% in patients with ovarian cancers and 62% in patients with endometrial cancers. Several patients remained on study for 6 to 11 months without clinically significant cumulative toxicities as of May 10, 2015 and the patients on for the longest duration remained on study as of such date. Median PFS were approximately
21
Table of Contents
177 days for endometrial cancers, 84 days for ovarian cancer and 66 days for cervical cancer. Patients with ovarian cancer had a median of five prior therapeutic regimens and patients with endometrial cancer had a median of two prior therapeutic regimens. The most common AEs, including nausea, anorexia, fatigue and thrombocytopenia, were typically Grades 1 or 2 and attenuated over time and/or responded to supportive care.
KING: Phase 2 Clinical Trial of Selinexor in Glioblastoma Multiforme
The KING study is a Phase 2 study evaluating the efficacy and safety of selinexor in patients with recurrent GBM. In June 2015, we presented data at the ASCO Annual Meeting where we showed that single-agent oral selinexor demonstrated anti-tumor activity in patients with glioblastoma that recurred after temozolomide and radiation therapy, including selinexor brain penetration at clinically relevant levels, leading to durable anti-cancer activity and disease control of up to 6 months. Specifically, data as of May 10, 2015 showed that selinexor dosed twice weekly at 50 mg/m2 demonstrated anti-tumor activity with a 13% overall response rate (PR or better) and a 38% disease control rate (SD or better) with durability of up to six months in 16 surgically ineligible patients with GBM that progressed after treatment with temozolomide and radiation. The most common AEs were thrombocytopenia, fatigue, anorexia, and hyponatremia.
Investigator-Sponsored Trials
Investigator-sponsored clinical trials are evaluating the safety and efficacy of selinexor as a single agent and in combination with existing therapies: (i) selinexor and standard capecitabine-based chemoradiation as a neoadjuvant treatment in locally advanced rectal cancer, (ii) selinexor, paclitaxel and carboplatin in ovarian or endometrial malignancies, (iii) selinexor and mFOLFOX6 in metastatic colorectal cancer, (iv) selinexor and standard chemotherapy agents in advanced solid tumors, (v) selinexor in metastatic castration resistant prostate cancer, (vi) selinexor in unresectable melanoma, (vii) selinexor in metastatic triple negative breast cancer, (viii) selinexor in poorly differentiated lung and gastroenteropancreatic neuroendocrine tumors (ix) selinexor in genomic profiling and matched therapy for recurrent or metastatic salivary gland neoplasms, (x) selinexor in Asian patients with advanced malignancies and (xi) selinexor in recurrent refractory pediatric solid tumors.
Company-Sponsored Phase 1 Clinical Trial Data
The primary objectives of our Phase 1 dose escalation trial in solids tumors were to determine the safety, tolerability and recommended Phase 2 dose of orally administered selinexor. All patients entered the study with advanced or metastatic solid tumor cancers relapsed or refractory after multiple previous treatments and objectively progressing on study entry. These patients were dosed 3-85mg/m2 (equivalent to approximately 5-145mg) of oral selinexor over a four-week cycle, with lower doses initially given ten times per cycle and higher doses given twice weekly. Response evaluation was done every two cycles in accordance with RECIST criteria.
As of September 15, 2015, 189 patients were enrolled in this Phase 1 clinical trial. Enrolled patients had received a median of three prior therapeutic regimens. Of these patients, 157 were evaluable for response and the DCR was 47%. PRs were observed in six patients, one each with colorectal cancer (KRAS mutant), melanoma, prostate cancer, ovarian adenocarcinoma, thymoma and cervical cancer, and one CR was observed in a patient with melanoma whose disease progressed on immunotherapy. SD was noted in 67 patients, with 27 patients (17%) experiencing SD for four months or longer, which we believe is an indication of clinically significant anti-tumor activity. In February 2016, data from this Phase 1 clinical trial were published in the Journal of Clinical Oncology.
KPT-8602
KPT-8602 is a second generation SINE compound that, like selinexor, selectively blocks the nuclear export protein XPO1. Most of the key tumor suppressor proteins, or TSPs, are cargos of XPO1 and inhibition of XPO1 by KPT-8602 sequesters TSPs in the nucleus where they can carry out their normal functions. As KPT-8602 acts through induction of TSPs, it is selectively cytotoxic for cells with genomic damage, i.e., for tumor cells, both in
22
Table of Contents
vitro and in vivo. KPT-8602 and other SINE compounds are not intrinsically cytotoxic. Rather, they can restore the highly effective tumor suppressing pathways that lead to selective elimination of genomically damaged, or neoplastic, cells. Cancer cells with damaged genomes are induced to undergo apoptosis. Normal cells, with an intact genome, remain in a transient, reversible cell cycle arrest until the export block is relieved. Tumors of hematopoietic lineage are particularly susceptible to apoptosis induction by XPO1 inhibition; normal hematopoietic cells and their functions are largely spared.
In preclinical models, KPT-8602 has a broad therapeutic window with minimal penetration of the blood brain barrier and, therefore, has the potential to serve as a second generation SINE compound for cancer indications. Following oral administration, animals treated with KPT-8602 show lower percentage of body weight loss and improved food consumption than animals similarly treated with selinexor. This allows more frequent dosing of KPT-8602, enabling a longer period of exposure at higher levels than is possible with selinexor. As a result, we believe that KPT-8602 represents a second generation SINE compound and are evaluating safety, tolerability and efficacy in humans.
Following the completion of toxicology studies, we filed an investigational new drug, or IND, application for KPT-8602 with the FDA in November 2015. Our first-in-humans clinical trial for KPT-8602 is a Phase 1/2 study in patients with relapsed/refractory multiple myeloma. The first patient in the Phase 1 dose escalation portion of the study was dosed in January 2016. We expect to determine the recommended Phase 2 dose for KPT-8602 by the end of 2016.
KPT-9274
In addition to our SINE compounds, we also investigate XPO1 cargo proteins and their role in the cell cycle and cell division. As part of this investigation, we have identified several XPO1 cargo proteins whose inhibition leads to the selective death of cancer cells. One of the XPO1 cargo proteins that we identified was p21-activated kinase 4, or PAK4. PAK4 is member of the PAK family of kinases that includes 6 proteins, PAK1-6. PAK4-6 belong to a growth-promoting sub-family. PAK4 is a signaling protein regulating numerous fundamental cellular processes, including intracellular transport, cellular division, cell shape and motility, cell survival, immune defense and the development of cancer. PAK4 interacts with many key signaling molecules involved in cancer such as beta-catenin, CDC42, Raf-1, BAD and myosin light chain. Based on this biology, we used our drug discovery and optimization expertise to identify small molecule modulators of PAK4. Our PAK4 allosteric modulators have shown broad evidence of anti-cancer activity against hematological and solid tumor malignant cells while showing minimal toxicity to normal cells in vitro. In mouse and rat xenograft studies, our PAK4 inhibitors given orally have shown evidence of anti-cancer activity and tolerability. To our knowledge, we are the only company with a pre-IND allosteric, PAK4 specific inhibitor.
Recently, we identified an additional target for our clinical candidate KPT-9274 known as NAMPT (Nicotinamide phosphoribosyltransferase; also known as PBEF or Visfatin). NAMPT is a pleiotropic protein with intra- and extra-cellular functions as an enzyme, cytokine, growth factor, and hormone that can be found in complex with PAK4 in the cell. NAMPT is of interest as an oncology target because it catalyzes the rate-limiting step in one of the two intracellular salvage pathways that generate nicotinamide adenine dinucleotide, or NAD. NAD is a universal energy- and signal-carrying molecule involved in mitochondrial function, energy metabolism, calcium homeostasis, antioxidation, and paradoxically generation of oxidative stress, gene expression, immunological functions, aging, and cell death.
KPT-9274 is a first-in-class orally bioavailable small molecule that is a non-competitive dual modulator of PAK4 and NAMPT. Co-inhibition of these targets leads to synergistic anti-tumor effects through energy depletion, inhibition of DNA repair, cell cycle arrest, inhibition of proliferation, and ultimately apoptosis. Normal cells are more resistant to inhibition by KPT-9274 due in part to their relative genomic stability and lower metabolic rates. Hematologic and solid tumor cells become dependent on both PAK4 and NAMPT pathways and are therefore susceptible to single-agent cytotoxicity by KPT-9274. We are planning to develop
23
Table of Contents
KPT-9274 for a variety of neoplastic disease indications. We have completed IND-enabling toxicology studies and filed an IND in February 2016 to facilitate a first-in-humans open-label Phase 1 clinical trial of the safety, tolerability, and efficacy of KPT-9274 in patients with advanced solid malignancies or non-Hodgkin’s lymphoma. We expect to dose the first patient with KPT-9274 during the middle of 2016.
Verdinexor (KPT-335): Oral SINE Compound for Lymphoma in Companion Canines
We have used spontaneously occurring canine cancers as a surrogate model for human malignancies. It is widely known that canine lymphomas display a comparable genetic profile and respond to chemotherapy in a fashion similar to their human counterparts (human NHL, most closely DLBCL). Lymphomas are one of the most common tumors in pet dogs. Lymphoma in dogs is very aggressive and, without treatment, the tumors are often fatal within weeks. The majority of dog lymphomas are DLBCL and most of the others are T-cell lymphomas. Given the similarities of dog and human lymphomas, prior to initiating clinical trials of selinexor in humans, we investigated verdinexor (KPT-335), a closely-related, orally available SINE compound in pet dogs with lymphomas. We have received a Minor Use / Minor Species, or MUMS, designation from the FDA’s Center for Veterinary Medicine, or CVM, for the treatment of newly-diagnosed or first relapse after chemotherapy lymphomas in pet dogs with verdinexor.
Several different dog tumor cell lines including those derived from lymphomas exhibited growth inhibition and apoptosis in vitro upon exposure to nanomolar concentrations of verdinexor. A Phase 1 clinical trial of verdinexor was performed in pet dogs with cancer, primarily with lymphoma. The maximum tolerated dose was 35mg/m2 (approximately 60mg) twice per week although biological activity was observed at 20mg/m2 (approximately 35mg). PR or SD, in each case for at least four weeks, was observed in nine out of 14 dogs (64%) with lymphoma with a median time to disease progression of 66 days (range of 35 to 256 days). We performed a dose expansion study in six dogs with lymphoma who were given 30mg/m2 of verdinexor three times per week; PR or SD was observed in four of the six dogs (67%) with a median time to disease progression of 83 days (range of 35 to 250 days). Side effects included anorexia, weight loss, vomiting and diarrhea and were manageable with dose modulation and supportive care. We conducted an owner observation-based survey and the data indicated that the overall quality of life did not change significantly in dogs treated with verdinexor. Based on these findings, a Phase 2b clinical trial, intended to support regulatory approval under the MUMS designation in the United States, was performed in 58 pet dogs with either newly-diagnosed or first relapse after chemotherapy lymphomas. Verdinexor was administered initially at doses ranging from 25mg/m2 to 30mg/m2 two or three days per week. Minimal or no supportive care was given. The total CRs and PRs of the 58 dogs was 34%, with one CR and 19 PRs. An additional 33 of 58 dogs (57%) experienced SD for at least four weeks. The median time to disease progression was approximately five weeks, with 20 dogs (34%) remaining on study for longer than eight weeks. A few dogs that received verdinexor in the Phase 1 or 2b studies remained on therapy for longer than eight months.
We submitted the safety and effectiveness sections of a New Animal Drug Application, or NADA, for verdinexor to the CVM in December 2013. We expect to seek to enter into a collaboration with a third party for the commercialization of verdinexor for dog lymphoma, if we obtain regulatory approval. We believe that verdinexor, if approved, would represent the first oral, targeted therapy for the treatment of dog lymphoma.
Our Non-Oncology Drug Candidates
Verdinexor (KPT-335): Oral SINE Compound for Viral Indications
Verdinexor (KPT-335) is an oral SINE compound and our lead compound that is being evaluated as a potential therapy for viral indications in addition to the canine lymphoma indication described above. Several viruses exclusively utilize XPO1 to shuttle cargos necessary for virion assembly such as viral ribonucleoproteins, or vRNA, and proteins from the nucleus to the cytoplasm. We have observed that SINE compounds mediate the inhibition of the nuclear export of influenza vRNP, leading to suppression of in vitro and in vivo replication of
24
Table of Contents
both A and B influenza strains. We have also observed potent activity of verdinexor across a broad panel of strains, including avian influenzas H5N1 and H7N9, consistent with the expectation that SINE compounds will suppress influenza viral replication independent of the origin of the virus as SINE compounds target the host protein. Orally administered verdinexor showed activity in a therapeutic regimen against an H1N1 influenza strain in ferrets and mice with a reduction in lung viral titer to a similar extent as neuraminidase inhibitors such as oseltamivir (Tamiflu®). In contrast to existing anti-influenza agents, however, verdinexor also reduced the expression of the pro-inflammatory cytokines IFN-g, IL-1b, IL-6 and TNF-a in H1N1-infected mouse lungs, allowing for the possibility that verdinexor could reduce “flu-like symptoms” and potentially severe inflammatory reactions, which can be fatal in human infections.
Based upon the anti-influenza activity of verdinexor in animal models, we believe that verdinexor has the potential to serve as an effective antiviral and anti-inflammatory therapy for influenza. In 2015, we conducted a randomized, double-blind, placebo-controlled, dose-escalating Phase 1 clinical trial of verdinexor in healthy human volunteers in Australia. This study was designed to evaluate the safety and tolerability of verdinexor in healthy adult subjects. Verdinexor was found to be generally safe and well tolerated. Mild to moderate AEs of similar number and grade as placebo were reported, but no serious or severe AEs were observed. We plan to continue the clinical development of verdinexor as a treatment for influenza. In addition, preclinical data also show efficacy of verdinexor and related SINE compounds in models of multiple additional viruses that utilize XPO1, including HIV.
KPT-350: Oral SINE Compound for Neurological, Inflammatory and Autoimmune Indications
KPT-350 is an IND-ready oral SINE compound with a preclinical data package supporting potential efficacy across a number of neurological, autoimmune and inflammatory conditions. XPO1 mediates the nuclear export of multiple proteins that impact neurological, autoimmune and inflammatory processes. Consequently, inhibition of XPO1 by KPT-350 results in a reduction in autoimmunity and inflammation and an increase in anti-inflammatory and neuroprotective responses. KPT-350 penetrates the blood brain barrier, or BBB, to a greater degree than other SINE compounds. Preclinical data generated largely by external collaborators show efficacy of orally-administered KPT-350 and related SINE compounds in animal models of amyotrophic lateral sclerosis, or ALS; traumatic brain injury, or TBI; multiple sclerosis, or MS; systemic lupus erythematosus, or lupus; and rheumatoid arthritis, or RA.
The ability of KPT-350 to affect TBI outcome was evaluated in three different rat models of TBI that are designed to mimic the heterogeneity of TBI observed in clinical practice: unilateral cortical injury, bilateral cortical injury, and fluid percussion injury models. In these studies, KPT-350 was administered orally with various dosing regimens from two to 72 hours post-injury. Efficacy was observed in each of the models, involving amelioration of TBI-induced cognitive and motor deficits. This functional activity was accompanied by KPT-350-mediated reduction of TBI lesion size, enhanced neuronal survival and suppression of inflammatory markers. We believe this indicates KPT-350 exerted a neuroprotective effect to prevent permanent neuronal loss due to the blunt force injury and subsequent inflammatory and neurotoxic effects. KPT-350 was effective even when treatment was initiated at 72 hours post injury. KPT-350 was also found to ameliorate BBB leakage associated with TBI, which has anti-inflammatory consequences independent of the other mechanisms of KPT-350 activity.
The neuroprotective effect of KPT-350 was further evaluated in a MS model of TNFalpha- and glutamate-induced neurotoxicity in primary rat cortical neurons. Treatment with KPT-350 prevented reductions in mitochondrial velocity and length, prevented reductions in spare respiratory capacity, a measure of neuron capacity, and prevented neurite beading, an overall indicator of neuronal dysfunction. KPT-350 treatment also reversed hind-limb paralysis and spinal cord inflammatory lesions in a murine EAE model of MS. We also tested KPT-350 in a TDP-43 adeno-associated virus or AAV rat model of ALS to determine if the compound could protect against TDP-43-induced neuro-toxicity and motor impairments. KPT-350 (7 mg/kg) or vehicle solution was administered orally twice weekly for three weeks followed by evaluation by the hang test, an assessment of
25
Table of Contents
grip strength Animals in the TDP/KPT-350 group had improved grip strength on the hang test, similar to healthy animals and higher than animals in the vehicle control group.
Our SINE compounds have also shown broad evidence of anti-inflammatory activity across various preclinical models suggesting that SINE compounds have multiple anti-inflammatory effects. Nuclear factor kB, or NF-kB, is a protein found in the nucleus that binds DNA and drives the expression of genes involved in many types of inflammation. In cells, NF-kB can be inhibited by another protein called IkB, or Inhibitor of NF-kB, that binds to NF-kB and prevents NF-kB from binding to DNA and activating inflammatory effects. When inflammation occurs, XPO1 transports IkB out of the nucleus into the cytoplasm where it cannot inhibit NF-kB activity. When KPT-350 or a similar SINE compound inhibits XPO1, IkB export to the cytoplasm is blocked and IkB accumulates in the nucleus. The IkB in the nucleus binds to NF-kB and blocks its inflammatory (transcriptional) activity. KPT-350 or a similar SINE compound also increase the concentration of other normal inhibitors of NF-kB in the nucleus including FOXO3a and COMMD1 proteins. Thus, XPO1 inhibition leads to potent, multifaceted inhibition of the potent inflammatory mediator NF-kB in a unique fashion.
We plan to partner with a collaborator to undertake the clinical development and potential commercialization of KPT-350 in one or more mutually agreed indications.
Intellectual Property
Our commercial success depends in part on our ability to obtain and maintain proprietary or intellectual property protection for our drug candidates, our core technologies, and other know-how, to operate without infringing on the proprietary rights of others and to prevent others from infringing our proprietary or intellectual property rights. Our policy is to seek to protect our proprietary and intellectual property position by, among other methods, filing patent applications in the United States and in foreign jurisdictions related to our proprietary technology and drug candidates. We also rely on trade secrets, know-how and continuing technological innovation to develop and maintain our proprietary and intellectual property position.
We file patent applications directed to the composition of matter and methods of use and manufacture for our drug candidates. As of March 1, 2016 , we were the sole owner of six patents in the United States and we had 18 pending patent applications in the United States, one of which is co-owned with a third party, three pending international applications filed under the Patent Cooperation Treaty (PCT), three granted patents and 134 pending patent applications in foreign jurisdictions. The PCT is an international patent law treaty that provides a unified procedure for filing a single initial patent application to seek patent protection for an invention simultaneously in each of the member states. Although a PCT application is not itself examined and cannot issue as a patent, it allows the applicant to seek protection in any of the member states through national-phase applications. The technology underlying such pending patent applications has been developed by us and was not acquired from any in-licensing agreement.
The intellectual property portfolios for our key drug candidates as of March 1, 2016 are summarized below.
| • | Selinexor (KPT-330): Our selinexor patent portfolio covers the composition of matter and methods of use of selinexor, as well as methods of making selinexor, and consists of two issued U.S. patents (one patent is specific to selinexor, and the other patent covers both selinexor and verdinexor), one issued foreign application, 32pending foreign patent applications, one pending U.S. non-provisional application and one pending PCT application directed to polymorphs of selinexor. The PCT application provides the opportunity for seeking protection in all PCT member states. Any patents that may issue in the United States as part of our selinexor patent portfolio, with the exception of a patent based on the pending PCT application, will expire in 2032, absent any terminal disclaimer, patent term adjustment due to administrative delays by the United States Patent and Trademark Office, or USPTO, or patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984, commonly referred to as the Hatch-Waxman Act. Any patents that may issue in foreign jurisdictions will likewise |
26
Table of Contents
| expire in 2032. Any patents that may issue in the United States based on the pending PCT application will expire in 2035, absent any terminal disclaimer, patent term adjustment due to administrative delays by the USPTO or patent term extension under the Hatch-Waxman Act. Any patent issued in foreign jurisdictions will likewise expire in 2035. |
| • | Selinexor (Wound Healing): Our patent portfolio covering selinexor for wound healing, including acute and chronic wounds, burns and scars, covers methods of using selinexor or verdinexor for wound healing, including systemic and topical uses, and consists of one pending U.S. application and one pending European application. Any patents that may issue in the United States will expire in 2034, absent any terminal disclaimer, patent term adjustment due to administrative delay by the USPTO or patent term extension under the Hatch-Waxman Act. Any patents issued in Europe will likewise expire in 2034. |
| • | Verdinexor (KPT-335): Our selinexor patent portfolio described above, with the exception of the pending PCT application, also covers both the composition of matter and methods of use of verdinexor, as well as methods of making verdinexor. There are two issued U.S. Patents that cover verdinexor. One patent is specific to verdinexor and the other patent covers both verdinexor and selinexor (also referenced above with respect to selinexor). |
| • | KPT-350: Our KPT-350 patent portfolio covers both the composition of matter and methods of use of KPT-350, and consists of two issued U.S. patents, two pending non-provisional U.S. patent applications and 24 pending foreign patent applications. Any patents that may issue in the United States as part of our KPT-350 patent portfolio will expire in 2033, absent any terminal disclaimer, patent term adjustment due to administrative delays by the USPTO or patent term extension under the Hatch-Waxman Act. Any patents issued in foreign jurisdictions will likewise expire in 2033. |
| • | KPT-8602: Our KPT-8602 patent portfolio covers both the composition of matter and methods of use of KPT-8602, and consists of one pending non-provisional U.S. patent application and 20 pending foreign patent applications. Any patents that may issue in the United States as part of our KPT-8602 patent portfolio will expire in 2034, absent any terminal disclaimer, patent term adjustment due to administrative delays by the USPTO or patent term extension under the Hatch-Waxman Act. Any patents issued in foreign jurisdictions will likewise expire in 2034. |
| • | PAK4/NAMPT Inhibitors: Our PAK4/NAMPT Inhibitors patent portfolio covers both the composition of matter and methods of use of the PAK4/NAMPT inhibitors described therein, such as KPT-9274, and consists of nine patent families with five pending U.S. provisional patent applications, two pending U.S. non-provisional patent applications, 21 pending foreign patent applications and two pending PCT applications in total. The PCT Applications provide the opportunity for seeking protection in all PCT member states. Any patents that may issue in the United States based on the pending U.S. non-provisional applications will expire in 2033 for the earliest filed application and 2034 for the remaining application, which covers the composition of matter and methods of use of KPT-9274, absent any terminal disclaimer, patent term adjustment due to administrative delays by the USPTO or patent term extension under the Hatch-Waxman Act. Any patents that may issue based on the pending foreign patent applications will likewise expire in 2033 and 2034. Foreign patent applications covering the composition of matter and methods of use of KPT-9274 have been filed in 20 countries/regions. Any patents that may issue in the United States based on the pending PCT applications will expire in 2034 for the earliest filed application and 2035 for the remaining application, absent any terminal disclaimer, patent term adjustment due to administrative delays by the USPTO or patent term extension under the Hatch-Waxman Act. Any patents issued in foreign jurisdictions will likewise expire in 2034 and 2035, respectively. We expect to file non-provisional patent applications claiming the benefit of the pending provisional applications in the second half of 2016. Any patents that may issue from such applications will expire no earlier than 2036. |
In addition to the patent portfolios covering our key drug candidates, as of March 1, 2016, our patent portfolio also includes one patent that was issued August 20, 2013 as U.S. Patent No. 8,513,230, two granted
27
Table of Contents
foreign patents and pending patent applications in both the U.S. and foreign jurisdictions relating to other XPO1 inhibitors and their use in targeted therapeutics. We also filed three Intent to Use Trademark Applications on August 29, 2013 covering our name, our logo and the two used together. Marks for the name and name and logo together were registered on January 20, 2015 as Registration Nos. 4,676,255 and 4,676,226. The mark for our logo was registered February 24, 2015 as Registration No. 4,693,100. We also have seven pending Intent to Use Trademark Applications that we filed in 2014 and 2015, five for drug names for selinexor, one for the term “SINE” and another for the term “PORE.” The five drug names for selinexor have been allowed and the other two applications are under examination. We also filed applications for the five drug names outside the United States. From these filings there are five registrations in the European Union. Two of the drug names were filed in 14 other jurisdictions some of which have also proceeded to registration.
The term of individual patents depends upon the legal term for patents in the countries in which they are obtained. In most countries, including the United States, the patent term is 20 years from the earliest filing date of a non-provisional patent application. In the United States, a patent’s term may be lengthened by patent term adjustment, which compensates a patentee for administrative delays by the USPTO in examining and granting a patent, or may be shortened if a patent is terminally disclaimed over an earlier filed patent. The term of a patent that covers a drug may also be eligible for patent term extension when FDA approval is granted, provided statutory and regulatory requirements are met. See “—Government Regulation—Patent Term Restoration and Extension” below for additional information on such extensions. In the future, if and when our drug candidates receive approval by the FDA or foreign regulatory authorities, we expect to apply for patent term extensions on issued patents covering those drugs, depending upon the length of the clinical trials for each drug candidate and other factors. There can be no assurance that any of our pending patent applications will issue or that we will benefit from any patent term extension or favorable adjustment to the term of any of our patents.
As with other biotechnology and pharmaceutical companies, our ability to maintain and solidify our proprietary and intellectual property position for our drug candidates and technologies will depend on our success in obtaining effective patent claims and enforcing those claims if granted. However, patent applications that we may file or license from third parties may not result in the issuance of patents. We also cannot predict the breadth of claims that may be allowed or enforced in our patents. Our issued patents and any issued patents that we may receive in the future may be challenged, invalidated or circumvented. For example, we cannot be certain of the priority of inventions covered by pending third-party patent applications. If third parties prepare and file patent applications that also claim technology or therapeutics to which we have rights, we may have to participate in interference proceedings to determine priority of invention, which could result in substantial costs to us, even if the eventual outcome is favorable to us. In addition, because of the extensive time required for clinical development and regulatory review of a drug candidate we may develop, it is possible that, before any of our drug candidates can be commercialized, any related patent may expire or remain in force for only a short period following commercialization, thereby reducing any advantage of any such patent.
In addition to patents, we rely upon unpatented trade secrets and know-how and continuing technological innovation to develop and maintain our competitive position. We seek to protect our proprietary information, in part, using confidentiality agreements with our collaborators, scientific advisors, employees and consultants, and invention assignment agreements with our employees. We also have agreements with selected consultants, scientific advisors and collaborators requiring assignment of inventions. The confidentiality agreements are designed to protect our proprietary information and, in the case of agreements or clauses requiring invention assignment, to grant us ownership of technologies that are developed through our relationship with a third party.
With respect to our proprietary drug discovery and optimization platform, we consider trade secrets and know-how to be our primary intellectual property. Trade secrets and know-how can be difficult to protect. We anticipate that with respect to this technology platform, these trade secrets and know-how may over time be disseminated within the industry through independent development, the publication of journal articles describing the methodology, and the movement of personnel skilled in the art from academic to industry scientific positions.
28
Table of Contents
Competition
The biotechnology and pharmaceutical industries are characterized by rapidly advancing technologies, intense competition and a strong emphasis on proprietary products. While we believe that our technology, knowledge, experience and scientific resources provide us with competitive advantages, we face potential competition from many different sources, including major pharmaceutical, specialty pharmaceutical and biotechnology companies, academic institutions and governmental agencies and public and private research institutions. Any drug candidates that we successfully develop and commercialize will compete with existing therapies and new therapies that may become available in the future.
There are several companies developing or marketing treatments for cancer and the other indications on which we currently plan to focus, including many major pharmaceutical and biotechnology companies. To our knowledge, no other company has an XPO1 inhibitor has enrolled patients in clinical trials at the present time. However, Stemline Therapeutics, Inc. announced in January 2015 that it had exclusively licensed the rights to develop and commercialize SL-801, an oral XPO1 inhibitor, from CanBas Co., Ltd. In December 2015, Stemline announced the opening of its investigational new drug, or IND, application and planned initiation of a clinical development program in multiple cancer types.
Many of the companies against which we are competing or against which we may compete in the future have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals and marketing approved products than we do. Mergers and acquisitions in the pharmaceutical and biotechnology industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel and establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or that may be necessary for, our programs.
The key competitive factors affecting the success of all of our drug candidates, if approved, are likely to be their efficacy, safety, convenience, price, the availability of generic chemotherapy and other cancer therapies and the availability of reimbursement from government and other third-party payors.
Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize drugs that are safer, more effective, have fewer or less severe side effects, are more convenient or are less expensive than any drugs that we may develop. Our competitors also may obtain FDA or other regulatory approval for their drugs more rapidly than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we are able to enter the market. In addition, our ability to compete may be affected in many cases by insurers or other third-party payors seeking to encourage the use of generic drugs. Generic drugs for the treatment of cancer and the other indications on which we currently plan to initially focus are currently on the market, and additional drugs are expected to become available on a generic basis over the coming years. If we obtain marketing approval for our drug candidates, we expect that they will be priced at a significant premium over generic versions of older chemotherapy agents and other cancer therapies.
The most common methods of treating patients with cancer are surgery, radiation and drug therapy. There are a variety of available drug therapies marketed for cancer. In many cases, these drugs are administered in combination to enhance efficacy. While our drug candidates may compete with many existing drugs and other therapies, to the extent they are ultimately used in combination with or as an adjunct to these therapies, our drug candidates will be complimentary with them. Some of the currently-approved drug therapies are branded and subject to patent protection, and others are available on a generic basis. Many of these approved drugs are well-established therapies and are widely-accepted by physicians, patients and third-party payors.
In addition to currently-marketed therapies, there are also a number of drugs in late stage clinical development to treat cancer and the other indications on which we plan to initially focus. These drugs in
29
Table of Contents
development may provide efficacy, safety, convenience and other benefits that are not provided by currently-marketed therapies. As a result, they may provide significant competition for any of our drug candidates for which we obtain marketing approval.
If our lead drug candidates are approved for the indications of our initial focus, they may compete with the investigational therapies and currently marketed drugs discussed below.
Multiple Myeloma (MM)
Over the past 12 years, ten agents have been approved in the U.S. for the treatment of patients with MM: bortezomib (Velcade®, Takeda), lenalidomide (Revlimid®, Celgene), thalidomide (Thalomid®, Celgene), liposomal doxorubicin (Doxil® , Janssen), carfilzomib (Kyprolis®, Amgen), pomalidomide (Pomalyst®, Celgene), panobinostat (Farydak®, Novartis), daratumumab (Darzalex®, Janssen), elotuzumab (Empliciti®, BMS), and ixazomib (Ninlaro®, Takeda). Approved indications range from the treatment of newly diagnosed patients to those with relapsed and/or refractory MM.
Several other anti-cancer agents are in late-stage development for the treatment of patients with MM such as vorinistat (Zolinza®, Merck), plitidepsin (PharMar), masitinib (AB Sciences), pembrolizumab (Keytruda® Merck), nivolumab (Opdivo® BMS), filanesib (Array Biopharma), and ricolinostat (Acetylon).
Acute Myeloid Leukemia (AML)
Patients with AML typically are treated with intensive multi-agent chemotherapy and high risk patients who enter remission and have a matched donor often receive an allogeneic stem cell transplant. Because these chemotherapy regimens have marked toxicities, elderly patients with AML are often treated with less intensive chemotherapy regimens or drugs called hypomethylating agents such as decitabine (Dacogen®, Otsuka) or azacitadine (Vidaza®, Celgene). Once elderly patients with AML experience disease progression on their initial treatment, their expected survival is very poor. Because of their advanced age, multiple other medical conditions and requirements for multiple other drugs, the treatment of relapsed and/or refractory AML in elderly persons is complicated. A number of anti-cancer agents (often in combination) are being investigated in this population, including but not limited to, midostaurin (Novartis), quizartinib (Daiichi Sankyo), volasertib (Boehringer Ingelheim), SGI-110 (Otsuka/Astex),AG-221 (Agios), venetoclax (Abbvie), SGN-CD33A (Seattle Genetics).
Non-Hodgkin’s Lymphoma (NHL)
The initial therapy for DLBCL typically consists of multi-agent cytotoxic drugs in combination with the monoclonal antibody rituximab (Rituxan®, Roche). In patients with DLBCL who are not elderly and who have good organ function, high dose chemotherapy with stem cell transplantation is often used. Newer targeted agents such as the BTK inhibitor ibrutinib (Imbruvica®, Pharmacyclics) the immunomodulatory drug lenalidomide (Revlimid®, Celgene) and bortezomib (Velcade® Takeda)have shown activity in DLBCL. There are also a number of other widely used anti-cancer agents that have broad labels which include NHL, and some of these are being evaluated alone or in combination for the treatment of patients with DLBCL that have relapsed after treatment with chemotherapy. Other anti-cancer agents are also being evaluated in the treatment of DLBCL, including but not limited to, obinutuzumab (Gazyva®, Roche) everolimus (Afinitor®, Novartis), lenalidomide (Revlimid®, Celgene), ofatumumab (Arzerra®, GSK), ibrutinib (Imbruvica®, Pharmacyclics), venetoclax (Abbvie), acalabrutinib (Acerta Pharma), nivolumab (Opdivo®, BMS) and brentuximab vedotin (Adcetris®, Seattle Genetics). In addition, chimeric antigen receptor T-cell therapies or CAR-T therapies, are currently in clinical development for the treatment of DLBCL by companies including Novartis, Juno and Kite, and may present future competition.
Competition with XPO1 Inhibitors
Drug compounds currently in preclinical studies, if developed and approved, could also be competitive with our drug candidates, if approved. In January 2015, Stemline Therapeutics, Inc. announced that it had exclusively
30
Table of Contents
licensed the rights to develop and commercialize SL-801, an XPO1 inhibitor, from CanBas Co., Ltd. In December 2015, Stemline announced the opening of its IND application and planned initiation of a clinical development program in multiple cancer types. Additionally, Kosan Biosciences Inc. (acquired by Bristol-Myers Squibb Company) has evaluated compounds derived from leptomycin B in preclinical studies. To our knowledge, the Kosan compounds are not currently being developed and have never entered human studies.
With respect to indications other than cancer, there are many currently-marketed therapies and drugs in late-stage clinical development to treat non-oncology indications on which we plan to initially focus development of our XPO1 inhibitors. However, to our knowledge, as in cancer, there are no other XPO1 inhibitors in clinical development for the treatment of any other diseases, including indications like autoimmune and inflammatory diseases or wound healing. There is no published information on the use of the preclinical compounds that have been developed by Kosan Biosciences or CanBas Co. in models other than cancer.
Competition with PAK4/NAMPT Dual Inhibitors
Our first-in-class PAK4/NAMPT dual inhibitor KPT-9274, if developed and approved, would compete with currently-marketed therapies and drugs in clinical development to treat cancer. However, there are currently no marketed therapies that selectively target PAK4 and/or NAMPT (Nicotinamide phosphoribosyltransferase, also known as PBEF or Visfatin). Pfizer Inc. developed PF-03758309, a non-selective PAK inhibitor, meaning that this compound inhibited several of the PAK family members, and not solely PAK4, through Phase 1 clinical development, but that compound had poor oral bioavailability in both animals and humans and, to our knowledge, development has been discontinued. We are aware that PAK4 biology is being evaluated preclinically by AstraZeneca plc and Genentech, Inc. (acquired by Roche Holding AG). We are not aware of any PAK4 inhibitors that are in clinical development at the present time.
To date, three NAMPT inhibitors have advanced into human clinical trials. These compounds include GMX1778 (also known as CHS-828), GMX1777 (water-soluble derivative of GMX1778), and APO866 (also known as FK866 and WK175). To our knowledge development of these inhibitors were discontinued. We are aware that NAMPT biology is being evaluated by Genentech, Lilly, Millennium/Takeda Pharmaceuticals, OncoTartis, Inc., Aurigene, and at some academic institutions. We are not aware of any other NAMPT inhibitors in clinical development.
Manufacturing
We do not have any manufacturing facilities or personnel. We currently rely, and expect to continue to rely, on third parties for the manufacture of our drug candidates for preclinical and clinical testing, as well as for commercial manufacture if our drug candidates receive marketing approval. We have engaged one third party manufacturer to obtain the active pharmaceutical ingredient for selinexor for preclinical and clinical testing. We have engaged a separate third-party manufacturer for fill-and-finish services. We obtain our selinexor supplies from these manufacturers on a purchase order basis and do not have a long-term supply arrangement in place at this time. We do not currently have arrangements in place for redundant supply. For all of our drug candidates, we intend to identify and qualify additional manufacturers to provide the active pharmaceutical ingredient and fill-and-finish services as a part of our commercialization plans.
All of our drug candidates are small molecules and are manufactured in reliable and reproducible synthetic processes from readily available starting materials. The chemistry is amenable to scale up and does not require unusual equipment in the manufacturing process. We expect to continue to develop drug candidates that can be produced cost-effectively at contract manufacturing facilities.
Government Regulation
Government authorities in the United States, at the federal, state and local level, and in other countries and jurisdictions, including the European Union, extensively regulate, among other things, the research, development,
31
Table of Contents
testing, manufacture, quality control, approval, packaging, storage, recordkeeping, labeling, advertising, promotion, distribution, marketing, post-approval monitoring and reporting, and import and export of pharmaceutical products. The processes for obtaining regulatory approvals in the United States and in foreign countries and jurisdictions, along with subsequent compliance with applicable statutes and regulations and other regulatory authorities, require the expenditure of substantial time and financial resources.
Review and Approval of Drugs in the United States
In the United States, the FDA approves and regulates drugs under the Federal Food, Drug, and Cosmetic Act, or FDCA, and implementing regulations. The failure to comply with the FDCA and other applicable laws at any time during the product development process, approval process or after approval may subject an applicant and/or sponsor to a variety of administrative or judicial sanctions, including refusal by the FDA to approve pending applications, withdrawal of an approval, imposition of a clinical hold, issuance of warning letters and other types of letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement of profits, or civil or criminal investigations and penalties brought by the FDA and the Department of Justice, or DOJ, or other governmental entities.
An applicant seeking approval to market and distribute a new drug product in the United States must typically undertake the following:
| • | completion of preclinical laboratory tests, animal studies and formulation studies in compliance with the FDA’s good laboratory practice, or GLP, regulations; |
| • | submission to the FDA of an investigational new drug application, or IND, which must take effect before human clinical trials may begin; |
| • | approval by an independent institutional review board, or IRB, representing each clinical site before each clinical trial may be initiated; |
| • | performance of adequate and well-controlled human clinical trials in accordance with good clinical practices, or GCP, to establish the safety and efficacy of the proposed drug product for each indication; |
| • | preparation and submission to the FDA of a new drug application, or NDA, requesting marketing for one or more proposed indications; |
| • | review of the product candidate by an FDA advisory committee, where appropriate or if applicable; |
| • | satisfactory completion of one or more FDA inspections of the manufacturing facility or facilities at which the product, or components thereof, are produced to assess compliance with current Good Manufacturing Practices, or cGMP, requirements and to assure that the facilities, methods and controls are adequate to preserve the product’s identity, strength, quality and purity; |
| • | satisfactory completion of FDA audits of clinical trial sites to assure compliance with GCPs and the integrity of the clinical data; |
| • | payment of user fees and securing FDA approval of the NDA; and |
| • | compliance with any post-approval requirements, including Risk Evaluation and Mitigation Strategies, or REMS, and post-approval studies required by the FDA. |
Preclinical Studies
Before an applicant begins testing a compound with potential therapeutic value in humans, the drug candidate enters the preclinical testing stage. Preclinical studies include laboratory evaluation of product chemistry, toxicity and formulation, and the purity and stability of the drug substance, as well as in vitro and animal studies to assess the potential safety and activity of the drug for initial testing in humans and to establish a
32
Table of Contents
rationale for therapeutic use. The conduct of preclinical studies is subject to federal regulations and requirements, including GLP regulations. Applicants usually must complete some long-term nonclinical testing, such as animal tests of reproductive adverse events and carcinogenicity, and must also develop additional information about the chemistry and physical characteristics of the drug and finalize a process for manufacturing the drug in commercial quantities in accordance with cGMP requirements.
The IND and IRB Processes
An IND is an exemption from the FDCA that allows an unapproved drug to be shipped in interstate commerce for use in an investigational clinical trial and a request for FDA authorization to administer an investigational drug to humans. Such authorization must be secured prior to interstate shipment and administration of any new drug that is not the subject of an approved NDA. In support of a request for an IND, applicants must submit a protocol for each clinical trial and any subsequent protocol amendments must be submitted to the FDA as part of the IND. In addition, the results of the preclinical tests, together with manufacturing information, analytical data, any available clinical data or literature and plans for clinical trials, among other things, are submitted to the FDA as part of an IND. The FDA requires a 30-day waiting period after the filing of each IND before clinical trials may begin. This waiting period is designed to allow the FDA to review the IND to determine whether human research subjects will be exposed to unreasonable health risks. At any time during this 30-day period, or thereafter, the FDA may raise concerns or questions about the conduct of the trials as outlined in the IND and impose a clinical hold or partial clinical hold. In this case, the IND sponsor and the FDA must resolve any outstanding concerns before clinical trials can begin.
In addition to the foregoing IND requirements, an IRB representing each institution participating in the clinical trial must review and approve the plan for any clinical trial before it commences at that institution, and the IRB must conduct continuing review and reapprove the study at least annually. The IRB must review and approve, among other things, the study protocol and informed consent information to be provided to study subjects. An IRB must operate in compliance with FDA regulations. Information about certain clinical trials must be submitted within specific timeframes to the National Institutes of Health, or NIH, for public dissemination on its ClinicalTrials.gov website. An IRB can suspend or terminate approval of a clinical trial at its institution, or an institution it represents, if the clinical trial is not being conducted in accordance with the IRB’s requirements or if the drug has been associated with unexpected serious harm to patients
Human Clinical Studies in Support of an NDA
Clinical trials involve the administration of the investigational product to human subjects under the supervision of qualified investigators in accordance with GCP requirements, which include, among other things, the requirement that all research subjects provide their informed consent in writing before their participation in any clinical trial. Clinical trials are conducted under written study protocols detailing, among other things, the objectives of the study, inclusion and exclusion criteria, the parameters to be used in monitoring safety and the effectiveness criteria to be evaluated.
Human clinical trials are typically conducted in four sequential phases, which may overlap or be combined:
| Phase 1: | The drug is initially introduced into a small number of healthy human subjects or patients with the target disease (e.g. cancer) or condition and tested for safety, dosage tolerance, absorption, metabolism, distribution, excretion and, if possible, to gain an early indication of its effectiveness and to determine optimal dosage. |
| Phase 2: | The drug is administered to a limited patient population to identify possible adverse effects and safety risks, to preliminarily evaluate the efficacy of the product for specific targeted diseases and to determine dosage tolerance and optimal dosage. |
33
Table of Contents
| Phase 3: | The drug is administered to an expanded patient population, generally at geographically dispersed clinical trial sites, in well-controlled clinical trials to generate enough data to statistically evaluate the efficacy and safety of the product for approval, to establish the overall risk-benefit profile of the product, and to provide adequate information for the labeling of the product. These clinical trials are commonly referred to as “pivotal” studies, which denotes a study that presents the data that the FDA or other relevant regulatory agency will use to determine whether or not to approve a drug. |
| Phase 4: | Post-approval studies may be conducted after initial marketing approval. These studies are used to gain additional experience from the treatment of patients in the intended therapeutic indication. |
Progress reports detailing the results of the clinical trials must be submitted at least annually to the FDA and more frequently if serious adverse events occur. In addition, IND safety reports must be submitted to the FDA for any of the following: serious and unexpected suspected adverse reactions; findings from other studies or animal or in vitro testing that suggest a significant risk in humans exposed to the drug; and any clinically important increase in the case of a serious suspected adverse reaction over that listed in the protocol or investigator brochure Phase 1, Phase 2 and Phase 3 clinical trials may not be completed successfully within any specified period, or at all. Furthermore, the FDA or the sponsor or the data monitoring committee may suspend or terminate a clinical trial at any time on various grounds, including a finding that the research subjects are being exposed to an unacceptable health risk. The FDA will typically inspect one or more clinical sites to assure compliance with GCP and the integrity of the clinical data submitted.
Review of an NDA by the FDA
Assuming successful completion of required clinical testing and other requirements, the results of the preclinical and clinical studies, together with detailed information relating to the product’s chemistry, manufacture, controls and proposed labeling, among other things, are submitted to FDA as part of an NDA requesting approval to market the drug product for one or more indications. The NDA must contain a description of the manufacturing process and quality control methods, as well as results of preclinical tests, toxicology studies, clinical trials and proposed labeling, among other things. Every new drug must be the subject of an approved NDA before it may be commercialized in the United States. Under federal law, the submission of most NDAs is subject to an application user fee, currently exceeding $2.3 million, and the sponsor of an approved NDA is also subject to annual product and establishment user fees, currently exceeding $114,000 per product and $585,000 per establishment. These fees are typically increased annually. Certain exceptions and waivers are available for some of these fees, such as an exception from the application fee for drugs with orphan designation and a waiver for certain small businesses, an exception from the establishment fee when the establishment does not engage in manufacturing the drug during a particular fiscal year, and an exception from the product fee for a drug that is the same as another drug approved under an abbreviated pathway.
Following submission of an NDA, the FDA conducts a preliminary review of an NDA within 60 calendar days of its receipt and strives to inform the sponsor by the 74th day after FDA’s receipt of the submission to determine whether the application is sufficiently complete to permit substantive review. The FDA may request additional information rather than accept an NDA for filing. In this event, the application must be resubmitted with the additional information. The resubmitted application is also subject to review before FDA accepts it for filing. Once the submission is accepted for filing, FDA begins an in-depth substantive review. The FDA has agreed to specified performance goals in the review process of NDAs. Under that agreement, 90% of applications seeking approval of New Molecular Entities, or NMEs, are meant to be reviewed within ten months from the date on which FDA accepts the NDA for filing, and 90% of applications for NMEs that have been designated for “priority review” are meant to be reviewed within six months of the filing date. For applications seeking approval of drugs that are not NMEs, the ten-month and six-month review periods run from the date that FDA receives the application. The review process and the Prescription Drug User Fee Act goal date may be extended by the FDA for three additional months to consider new information or clarification provided by the applicant to address an outstanding deficiency identified by the FDA following the original submission.
34
Table of Contents
Before approving an NDA, the FDA typically will inspect the facility or facilities where the product is or will be manufactured. These pre-approval inspections may cover all facilities associated with an NDA submission, including drug component manufacturing (such as active pharmaceutical ingredients), finished drug product manufacturing, and control testing laboratories. The FDA will not approve an application unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required specifications. Additionally, before approving an NDA, the FDA will typically inspect one or more clinical sites to assure compliance with GCP.
In addition, as a condition of approval, the FDA may require an applicant to develop a REMS. REMS use risk minimization strategies beyond the professional labeling to ensure that the benefits of the product outweigh the potential risks. To determine whether a REMS is needed, the FDA will consider the size of the population likely to use the product, seriousness of the disease, expected benefit of the product, expected duration of treatment, seriousness of known or potential adverse events, and whether the product is a new molecular entity. REMS can include medication guides, physician communication plans for healthcare professionals, and elements to assure safe use, or ETASU. ETASU may include, but are not limited to, special training or certification for prescribing or dispensing, dispensing only under certain circumstances, special monitoring, and the use of patient registries. The FDA may require a REMS before approval or post-approval if it becomes aware of a serious risk associated with use of the product. The requirement for a REMS can materially affect the potential market and profitability of a product.
The FDA is required to refer an application for a novel drug to an advisory committee or explain why such referral was not made. Typically, an advisory committee is a panel of independent experts, including clinicians and other scientific experts, that reviews, evaluates and provides a recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendations of an advisory committee, but it considers such recommendations carefully when making decisions.
Fast Track, Breakthrough Therapy and Priority Review Designations
The FDA is authorized to designate certain products for expedited review if they are intended to address an unmet medical need in the treatment of a serious or life-threatening disease or condition. These programs are fast track designation, breakthrough therapy designation and priority review designation.
Specifically, the FDA may designate a product for fast track review if it is intended, whether alone or in combination with one or more other drugs, for the treatment of a serious or life-threatening disease or condition, and it demonstrates the potential to address unmet medical needs for such a disease or condition. For fast track products, sponsors may have greater interactions with the FDA and the FDA may initiate review of sections of a fast track product’s NDA before the application is complete. This rolling review may be available if the FDA determines, after preliminary evaluation of clinical data submitted by the sponsor, that a fast track product may be effective. The sponsor must also provide, and the FDA must approve, a schedule for the submission of the remaining information and the sponsor must pay applicable user fees. However, the FDA’s time period goal for reviewing a fast track application does not begin until the last section of the NDA is submitted. In addition, the fast track designation may be withdrawn by the FDA if the FDA believes that the designation is no longer supported by data emerging in the clinical trial process.
Second, in 2012, Congress enacted the Food and Drug Administration Safety and Innovation Act, or FDASIA. This law established a new regulatory scheme allowing for expedited review of products designated as “breakthrough therapies.” A product may be designated as a breakthrough therapy if it is intended, either alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or condition and preliminary clinical evidence indicates that the product may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. The FDA may take certain actions with respect to breakthrough therapies, including holding meetings with the sponsor throughout the development process; providing timely advice to the product
35
Table of Contents
sponsor regarding development and approval; involving more senior staff in the review process; assigning a cross-disciplinary project lead for the review team; and taking other steps to design the clinical trials in an efficient manner.
Third, the FDA may designate a product for priority review if it is a drug that treats a serious condition and, if approved, would provide a significant improvement in safety or effectiveness. The FDA determines, on a case-by-case basis, whether the proposed drug represents a significant improvement when compared with other available therapies. Significant improvement may be illustrated by evidence of increased effectiveness in the treatment of a condition, elimination or substantial reduction of a treatment-limiting drug reaction, documented enhancement of patient compliance that may lead to improvement in serious outcomes, and evidence of safety and effectiveness in a new subpopulation. A priority designation is intended to direct overall attention and resources to the evaluation of such applications, and to shorten the FDA’s goal for taking action on a marketing application from ten months to six months.
Accelerated Approval Pathway
The FDA may grant accelerated approval to a drug for a serious or life-threatening condition that provides meaningful therapeutic advantage to patients over existing treatments based upon a determination that the drug has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit. The FDA may also grant accelerated approval for such a condition when the product has an effect on an intermediate clinical endpoint that can be measured earlier than an effect on irreversible morbidity or mortality, or IMM, and that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity, or prevalence of the condition and the availability or lack of alternative treatments. Drugs granted accelerated approval must meet the same statutory standards for safety and effectiveness as those granted traditional approval.
For the purposes of accelerated approval, a surrogate endpoint is a marker, such as a laboratory measurement, radiographic image, physical sign, or other measure that is thought to predict clinical benefit, but is not itself a measure of clinical benefit. Surrogate endpoints can often be measured more easily or more rapidly than clinical endpoints. An intermediate clinical endpoint is a measurement of a therapeutic effect that is considered reasonably likely to predict the clinical benefit of a drug, such as an effect on IMM. The FDA has limited experience with accelerated approvals based on intermediate clinical endpoints, but has indicated that such endpoints generally may support accelerated approval where the therapeutic effect measured by the endpoint is not itself a clinical benefit and basis for traditional approval, if there is a basis for concluding that the therapeutic effect is reasonably likely to predict the ultimate clinical benefit of a drug.
The accelerated approval pathway is most often used in settings in which the course of a disease is long and an extended period of time is required to measure the intended clinical benefit of a drug, even if the effect on the surrogate or intermediate clinical endpoint occurs rapidly. Thus, accelerated approval has been used extensively in the development and approval of drugs for treatment of a variety of cancers in which the goal of therapy is generally to improve survival or decrease morbidity and the duration of the typical disease course requires lengthy and sometimes large trials to demonstrate a clinical or survival benefit.
The accelerated approval pathway is usually contingent on a sponsor’s agreement to conduct, in a diligent manner, additional post-approval confirmatory studies to verify and describe the drug’s clinical benefit. As a result, a drug candidate approved on this basis is subject to rigorous post-marketing compliance requirements, including the completion of Phase 4 or post-approval clinical trials to confirm the effect on the clinical endpoint. Failure to conduct required post-approval studies, or confirm a clinical benefit during post-marketing studies, would allow the FDA to withdraw the drug from the market on an expedited basis. All promotional materials for drug candidates approved under accelerated regulations are subject to prior review by the FDA.
36
Table of Contents
The FDA’s Decision on an NDA
On the basis of the FDA’s evaluation of the NDA and accompanying information, including the results of the inspection of the manufacturing facilities, the FDA may issue an approval letter or a complete response letter. An approval letter authorizes commercial marketing of the product with specific prescribing information for specific indications. A complete response letter generally outlines the deficiencies in the submission and may require substantial additional testing or information in order for the FDA to reconsider the application. If and when those deficiencies have been addressed to the FDA’s satisfaction in a resubmission of the NDA, the FDA will issue an approval letter. The FDA has committed to reviewing such resubmissions in two or six months depending on the type of information included. Even with submission of this additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval.
If the FDA approves a product, it may limit the approved indications for use for the product, require that contraindications, warnings or precautions be included in the product labeling, require that post-approval studies, including Phase 4 clinical trials, be conducted to further assess the drug’s safety after approval, require testing and surveillance programs to monitor the product after commercialization, or impose other conditions, including distribution restrictions or other risk management mechanisms, including REMS, which can materially affect the potential market and profitability of the product. The FDA may prevent or limit further marketing of a product based on the results of post-market studies or surveillance programs. After approval, many types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further testing requirements and FDA review and approval.
Post-Approval Requirements
Drugs manufactured or distributed pursuant to FDA approvals are subject to pervasive and continuing regulation by the FDA, including, among other things, requirements relating to recordkeeping, periodic reporting, product sampling and distribution, advertising and promotion and reporting of adverse experiences with the product. After approval, most changes to the approved product, such as adding new indications or other labeling claims, are subject to prior FDA review and approval. There also are continuing, annual user fee requirements for any marketed products and the establishments at which such products are manufactured, as well as new application fees for supplemental applications with clinical data.
In addition, drug manufacturers and other entities involved in the manufacture and distribution of approved drugs are required to register their establishments with the FDA and state agencies, and are subject to periodic unannounced inspections by the FDA and these state agencies for compliance with cGMP requirements. Changes to the manufacturing process are strictly regulated and often require prior FDA approval before being implemented. FDA regulations also require investigation and correction of any deviations from cGMP and impose reporting and documentation requirements upon the sponsor and any third-party manufacturers that the sponsor may decide to use. Accordingly, manufacturers must continue to expend time, money, and effort in the area of production and quality control to maintain cGMP compliance.
Once an approval is granted, the FDA may withdraw the approval if compliance with regulatory requirements and standards is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with manufacturing processes, or failure to comply with regulatory requirements, may result in revisions to the approved labeling to add new safety information; imposition of post-market studies or clinical trials to assess new safety risks; or imposition of distribution or other restrictions under a REMS program. Other potential consequences include, among other things:
| • | restrictions on the marketing or manufacturing of the product, suspension of the approval, complete withdrawal of the product from the market or product recalls; |
| • | fines, warning letters or holds on post-approval clinical trials; |
37
Table of Contents
| • | refusal of the FDA to approve pending NDAs or supplements to approved NDAs, or suspension or revocation of product license approvals; |
| • | product seizure or detention, or refusal to permit the import or export of products; or |
| • | injunctions or the imposition of civil or criminal penalties. |
The FDA strictly regulates marketing, labeling, advertising and promotion of products that are placed on the market. Drugs may be promoted only for the approved indications and in accordance with the provisions of the approved label. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is found to have improperly promoted off-label uses may be subject to significant liability.
In addition, the distribution of prescription pharmaceutical products is subject to the Prescription Drug Marketing Act, or PDMA, and its implementing regulations, as well as the Drug Supply Chain Security Act, or DSCA, which regulate the distribution and tracing of prescription drugs and prescription drug samples at the federal level, and set minimum standards for the regulation of drug distributors by the states. The PDMA, its implementing regulations and state laws limit the distribution of prescription pharmaceutical product samples, and the DSCA imposes requirements to ensure accountability in distribution and to identify and remove counterfeit and other illegitimate products from the market.
Section 505(b)(2) NDAs
NDAs for most new drug products are based on two full clinical studies which must contain substantial evidence of the safety and efficacy of the proposed new product. These applications are submitted under Section 505(b)(1) of the FDCA. The FDA is, however, authorized to approve an alternative type of NDA under Section 505(b)(2) of the FDCA. This type of application allows the applicant to rely, in part, on the FDA’s previous findings of safety and efficacy for a similar product, or published literature. Specifically, Section 505(b)(2) applies to NDAs for a drug for which the investigations made to show whether or not the drug is safe for use and effective in use and relied upon by the applicant for approval of the application “were not conducted by or for the applicant and for which the applicant has not obtained a right of reference or use from the person by or for whom the investigations were conducted.”
Thus, Section 505(b)(2) authorizes the FDA to approve an NDA based on safety and effectiveness data that were not developed by the applicant. NDAs filed under Section 505(b)(2) may provide an alternate and potentially more expeditious pathway to FDA approval for new or improved formulations or new uses of previously approved products. If the 505(b)(2) applicant can establish that reliance on the FDA’s previous approval is scientifically appropriate, the applicant may eliminate the need to conduct certain preclinical or clinical studies of the new product. The FDA may also require companies to perform additional studies or measurements to support the change from the approved product. The FDA may then approve the new drug candidate for all or some of the label indications for which the referenced product has been approved, as well as for any new indication sought by the Section 505(b)(2) applicant.
Abbreviated New Drug Applications for Generic Drugs
In 1984, with passage of the Hatch-Waxman Amendments to the FDCA, Congress established an abbreviated regulatory scheme authorizing the FDA to approve generic drugs that are shown to contain the same active ingredients as, and to be bioequivalent to, drugs previously approved by the FDA pursuant to NDAs. To obtain approval of a generic drug, an applicant must submit an abbreviated new drug application, or ANDA, to the agency. An ANDA is a comprehensive submission that contains, among other things, data and information pertaining to the active pharmaceutical ingredient, bioequivalence, drug product formulation, specifications and stability of the generic drug, as well as analytical methods, manufacturing process validation data and quality control procedures. ANDAs are “abbreviated” because they generally do not include preclinical and clinical data
38
Table of Contents
to demonstrate safety and effectiveness. Instead, in support of such applications, a generic manufacturer may rely on the preclinical and clinical testing previously conducted for a drug product previously approved under an NDA, known as the reference-listed drug, or RLD.
Specifically, in order for an ANDA to be approved, the FDA must find that the generic version is identical to the RLD with respect to the active ingredients, the route of administration, the dosage form, the strength of the drug and the conditions of use of the drug. At the same time, the FDA must also determine that the generic drug is “bioequivalent” to the innovator drug. Under the statute, a generic drug is bioequivalent to a RLD if “the rate and extent of absorption of the drug do not show a significant difference from the rate and extent of absorption of the listed drug.” Upon approval of an ANDA, the FDA indicates whether the generic product is “therapeutically equivalent” to the RLD in its publication “Approved Drug Products with Therapeutic Equivalence Evaluations,” also referred to as the “Orange Book.” Physicians and pharmacists consider a therapeutic equivalent generic drug to be fully substitutable for the RLD. In addition, by operation of certain state laws and numerous health insurance programs, the FDA’s designation of therapeutic equivalence often results in substitution of the generic drug without the knowledge or consent of either the prescribing physician or patient.
Under the Hatch-Waxman Amendments, the FDA may not approve an ANDA until any applicable period of non-patent exclusivity for the RLD has expired. The FDCA provides a period of five years of non-patent data exclusivity for a new drug containing a new chemical entity. For the purposes of this provision, a new chemical entity, or NCE, is a drug that contains no active moiety that has previously been approved by the FDA in any other NDA. An active moiety is the molecule or ion responsible for the physiological or pharmacological action of the drug substance. In cases where such NCE exclusivity has been granted, an ANDA may not be filed with the FDA until the expiration of five years unless the submission is accompanied by a Paragraph IV certification, in which case the applicant may submit its application four years following the original product approval. The FDCA also provides for a period of three years of exclusivity if the NDA includes reports of one or more new clinical investigations, other than bioavailability or bioequivalence studies, that were conducted by or for the applicant and are essential to the approval of the application.
Hatch-Waxman Patent Certification and the 30-Month Stay
Upon approval of an NDA or a supplement thereto, NDA sponsors are required to list with the FDA each patent with claims that cover the applicant’s product or an approved method of using the product. Each of the patents listed by the NDA sponsor is published in the Orange Book. When an ANDA or 505(b)(2) applicant files its application with the FDA, the applicant is required to certify to the FDA concerning any patents listed for the reference product in the Orange Book, except for patents covering methods of use for which the ANDA applicant is not seeking approval. Specifically, the applicant must certify with respect to each patent that:
| • | the required patent information has not been filed; |
| • | the listed patent has expired; |
| • | the listed patent has not expired, but will expire on a particular date and approval is sought after patent expiration; or |
| • | the listed patent is invalid, unenforceable or will not be infringed by the new product. |
A certification that the new product will not infringe the already approved product’s listed patents or that such patents are invalid or unenforceable is called a Paragraph IV certification. If the applicant does not challenge the listed patents or indicates that it is not seeking approval of a patented method of use, the application will not be approved until all the listed patents claiming the referenced product have expired (other than method of use patents involving indications for which the applicant is not seeking approval).
If the ANDA or 505(b)(2) applicant has provided a Paragraph IV certification to the FDA, the applicant must also send notice of the Paragraph IV certification to the NDA and patent holders once the ANDA or the
39
Table of Contents
505(b)(2) application has been accepted for filing by the FDA. The NDA and patent holders may then initiate a patent infringement lawsuit in response to the notice of the Paragraph IV certification. The filing of a patent infringement lawsuit within 45 days after the receipt of a Paragraph IV certification automatically prevents the FDA from approving the ANDA or 505(b)(2) application until the earlier of 30 months after the receipt of the Paragraph IV notice, expiration of the patent, or a decision in the infringement case that is favorable to the applicant. The ANDA or 505(b)(2) application also will not be approved until any applicable non-patent exclusivity listed in the Orange Book for the branded reference drug has expired.
Patent Term Restoration and Extension
A patent claiming a new drug product or its method of use may be eligible for a limited patent term extension, also known as patent term restoration, under the Hatch-Waxman Act, which permits a patent restoration of up to five years for patent term lost during product development and the FDA regulatory review. Patent term extension is generally available only for drug products whose active ingredient has not previously been approved by the FDA. The restoration period granted is typically one-half the time between the effective date of an IND and the submission date of an NDA, plus the time between the submission date of an NDA and the ultimate approval date. Patent term extension cannot be used to extend the remaining term of a patent past a total of 14 years from the product’s approval date. Only one patent applicable to an approved drug product is eligible for the extension, and the application for the extension must be submitted prior to the expiration of the patent in question. A patent that covers multiple drugs for which approval is sought can only be extended in connection with one of the approvals. The United States PTO reviews and approves the application for any patent term extension in consultation with the FDA.
Pediatric Studies and Exclusivity
Under the Pediatric Research Equity Act of 2003, a NDA or supplement thereto must contain data that are adequate to assess the safety and effectiveness of the drug product for the claimed indications in all relevant pediatric subpopulations, and to support dosing and administration for each pediatric subpopulation for which the product is safe and effective. With enactment of the Food and Drug Administration Safety and Innovation Act, or FDASIA, in 2012, sponsors must also submit pediatric study plans prior to the assessment data. Those plans must contain an outline of the proposed pediatric study or studies the applicant plans to conduct, including study objectives and design, any deferral or waiver requests, and other information required by regulation. The applicant, FDA, and FDA’s internal review committee must then review the information submitted, consult with each other, and agree upon a final plan. The FDA or the applicant may request an amendment to the plan at any time.
The FDA may, on its own initiative or at the request of the applicant, grant deferrals for submission of some or all pediatric data until after approval of the product for use in adults, or full or partial waivers from the pediatric data requirements. Additional requirements and procedures relating to deferral requests and requests for extension of deferrals are contained in FDASIA. Unless otherwise required by regulation, the pediatric data requirements do not apply to products with orphan designation.
Pediatric exclusivity is another type of non-patent marketing exclusivity in the United States and, if granted, provides for the attachment of an additional six months of marketing protection to the term of any existing regulatory exclusivity, including the non-patent and orphan exclusivity. This six-month exclusivity may be granted if an NDA sponsor submits pediatric data that fairly respond to a written request from the FDA for such data. The data do not need to show the product to be effective in the pediatric population studied; rather, if the clinical trial is deemed to fairly respond to the FDA’s request, the additional protection is granted. If reports of requested pediatric studies are submitted to and accepted by the FDA within the statutory time limits, whatever statutory or regulatory periods of exclusivity or patent protection cover the product are extended by six months. This is not a patent term extension, but it effectively extends the regulatory period during which the FDA cannot accept or approve another application.
40
Table of Contents
Orphan Drug Designation and Exclusivity
Under the Orphan Drug Act, FDA may designate a drug product as an “orphan drug” if it is intended to treat a rare disease or condition (generally meaning that it affects fewer than 200,000 individuals in the United States, or more in cases in which there is no reasonable expectation that the cost of developing and making a drug product available in the United States for treatment of the disease or condition will be recovered from sales of the product). A company must request orphan product designation before submitting a NDA. If the request is granted, FDA will disclose the identity of the therapeutic agent and its potential use. Orphan product designation does not convey any advantage in or shorten the duration of the regulatory review and approval process.
If a product with orphan status receives the first FDA approval for the disease or condition for which it has such designation or for a select indication or use within the rare disease or condition for which it was designated, the product generally will be entitled to orphan product exclusivity. Orphan product exclusivity means that FDA may not approve any other applications for the same product for the same indication for seven years, except in certain limited circumstances. Competitors may receive approval of different products for the indication for which the orphan product has exclusivity and may obtain approval for the same product but for a different indication. If a drug or drug product designated as an orphan product ultimately receives marketing approval for an indication broader than what was designated in its orphan product application, it may not be entitled to exclusivity.
Review and Approval of Drug Products in the European Union
In addition to regulations in the United States, a manufacturer is subject to a variety of regulations in foreign jurisdictions to the extent it chooses to sell any drug products in those foreign countries. Even if a manufacturer obtains FDA approval of a product, it must still obtain the requisite approvals from regulatory authorities in foreign countries prior to the commencement of clinical trials or marketing of the product in those countries. To obtain regulatory approval of an investigational drug in the European Union (EU), a manufacturer must submit a marketing authorization application, or MAA, to the European Medicines Agency, or EMA.
Clinical Trial Approval in the EU
Pursuant to the currently applicable Clinical Trials Directives, an applicant must obtain approval from the competent national authority of the EU Member State in which the clinical trial is to be conducted. If the clinical trial is conducted in different EU Member States, the competent authorities in each of these EU Member States must provide their approval for the conduct of the clinical trial. Furthermore, the applicant may only start a clinical trial at a specific study site after the competent ethics committee has issued a favorable opinion. In April 2014, the EU adopted a new Clinical Trials Regulation, which is set to replace the current Clinical Trials Directive. The new Clinical Trials Regulation will be directly applicable to and binding in all 28 EU Member States without the need for any national implementing legislation, and will become applicable no earlier than 28 May 2016. Under the new coordinated procedure for the approval of clinical trials, the sponsor of a clinical trial will be required to submit a single application for approval of a clinical trial to a reporting EU Member State (RMS) through an EU Portal. The submission procedure will be the same irrespective of whether the clinical trial is to be conducted in a single EU Member State or in more than one EU Member State. The Clinical Trials Regulation also aims to streamline and simplify the rules on safety reporting for clinical trials.
Marketing Authorization
In the EU, marketing authorizations for medicinal products may be obtained through several different procedures founded on the same basic regulatory process.
The centralized procedure provides for the grant of a single marketing authorization that is valid for all EU Member States. The centralized procedure is compulsory for medicinal products produced by certain
41
Table of Contents
biotechnological processes, products designated as orphan medicinal products, and products with a new active substance indicated for the treatment of certain diseases,. It is optional for those products that are highly innovative or for which a centralized process is in the interest of patients. Under the centralized procedure in the EU, the maximum timeframe for the evaluation of a MAA is 210 days, excluding clock stops, when additional written or oral information is to be provided by the applicant in response to questions asked by the Committee for Medicinal Products for Human use or CHMP. Accelerated evaluation may be granted by the CHMP in exceptional cases. These are defined as circumstances in which a medicinal product is expected to be of a “major public health interest.” Three cumulative criteria must be fulfilled in such circumstances: the seriousness of the disease, such as severely disabling or life-threatening diseases, to be treated; the absence or insufficiency of an appropriate alternative therapeutic approach; and anticipation of high therapeutic benefit. In these circumstances, the EMA ensures that the opinion of the CHMP is given within 150 days.
The decentralized procedure provides for approval by one or more other concerned EU Member States of an assessment of an application for marketing authorization conducted by one EU Member State, known as the reference EU Member State. In accordance with this procedure, an applicant submits an application for marketing authorization to the reference EU Member State and the concerned EU Member States. This application is identical to the application that would be submitted to the EMA for authorization through the centralized procedure. The reference EU Member State prepares a draft assessment and drafts of the related materials within 120 days after receipt of a valid application. The resulting assessment report is submitted to the concerned EU Member States which, within 90 days of receipt, must decide whether to approve the assessment report and related materials. If a concerned EU Member State cannot approve the assessment report and related materials due to concerns relating to a potential serious risk to public health, disputed elements may be referred to the European Commission, whose decision is binding on all EU Member States. In accordance with the mutual recognition procedure, the sponsor applies for national marketing authorization in one EU Member State. Upon receipt of this authorization the sponsor can then seek the recognition of this authorization by other EU Member States. Authorization in accordance with either of these procedures will result in authorization of the medicinal product only in the reference EU Member State and in the other concerned EU Member States.
Periods of Authorization and Renewals in the EU
A marketing authorization is valid for five years, in principle, and it may be renewed after five years on the basis of a reevaluation of the risk-benefit balance by the EMA or by the competent authority of the relevant EU Member State. To that end, the marketing authorization holder must provide the EMA or the relevant competent authority of the EU Member State with a consolidated version of the file in respect of quality, safety and efficacy, including all variations introduced since the marketing authorization was granted, at least six months before the marketing authorization ceases to be valid. Once renewed, the marketing authorization is valid for an unlimited period, unless the European Commission or the relevant competent authority of the EU Member State decides, on justified grounds relating to pharmacovigilance, to proceed with one additional five-year renewal period. Any marketing authorization that is not followed by the marketing of the medicinal product on the EU market (in the case of the centralized procedure) or on the market of the EU Member State which delivered the marketing authorization within three years after authorization ceases to be valid.
Data and Market Exclusivity in the European Union
In the European Union, new chemical entities qualify for eight years of data exclusivity upon marketing authorization and an additional two years of market exclusivity. This data exclusivity, if granted, prevents regulatory authorities in the European Union from referencing the innovator’s data to assess a generic (abbreviated) application for eight years, after which generic marketing authorization can be submitted, and the innovator’s data may be referenced, but not approved for two years. The overall ten-year period will be extended to a maximum of eleven years if, during the first eight years of those ten years, the marketing authorization holder obtains an authorization for one or more new therapeutic indications which, during the scientific evaluation prior to their authorization, are held to bring a significant clinical benefit in comparison with existing
42
Table of Contents
therapies. Even if a compound is considered to be a new chemical entity and the sponsor is able to gain the prescribed period of data exclusivity, another company nevertheless could also market another version of the drug if such company can complete a full MAA with a complete database of pharmaceutical test, preclinical tests and clinical trials and obtain marketing approval of its product.
Orphan Drug Designation and Exclusivity in the EU
In the EU, a product may be designated as an orphan medicinal product by the European Commission if its sponsor can establish that the product is intended for the diagnosis, prevention or treatment of: (1) a life-threatening or chronically debilitating condition affecting not more than five in ten thousand persons in the EU when the application is made, or (2) a life-threatening, seriously debilitating or serious and chronic condition in the EU and that without incentives the medicinal product is unlikely to be developed. For either of these conditions, the applicant must demonstrate that there exists no satisfactory method of diagnosis, prevention or treatment of the condition in question that has been authorized in the EU or, if such method exists, the medicinal product will be of significant benefit to those affected by that condition.
Once authorized, orphan medicinal products are entitled to ten years of market exclusivity in all EU Member States and, in addition, a range of other benefits during the development and regulatory review process. However, marketing authorization may be granted to a similar medicinal product with the same orphan indication during the ten year period with the consent of the marketing authorization holder for the original orphan medicinal product or if the manufacturer of the original orphan medicinal product is unable to supply sufficient quantities. Marketing authorization may also be granted to a similar medicinal product with the same orphan indication if the product is safer, more effective or otherwise clinically superior to the original orphan medicinal product. The period of market exclusivity may, in addition, be reduced to six years if it can be demonstrated on the basis of available evidence that the original orphan medicinal product is sufficiently profitable not to justify maintenance of market exclusivity.
Pharmaceutical Coverage, Pricing and Reimbursement
In the United States and markets in other countries, patients who are prescribed treatments for their conditions and providers performing the prescribed services generally rely on third-party payors to reimburse all or part of the associated healthcare costs. Significant uncertainty exists as to the coverage and reimbursement status of products approved by the FDA and other government authorities. Thus, even if a product candidate is approved, sales of the product will depend, in part, on the extent to which third-party payors, including government health programs in the United States such as Medicare and Medicaid, commercial health insurers and managed care organizations, provide coverage, and establish adequate reimbursement levels for, the product. The process for determining whether a payor will provide coverage for a product may be separate from the process for setting the price or reimbursement rate that the payor will pay for the product once coverage is approved. Third-party payors are increasingly challenging the prices charged, examining the medical necessity, and reviewing the cost-effectiveness of medical products and services and imposing controls to manage costs. Third-party payors may limit coverage to specific products on an approved list, also known as a formulary, which might not include all of the approved products for a particular indication.
In order to secure coverage and reimbursement for any product that might be approved for sale, a company may need to conduct expensive pharmacoeconomic studies in order to demonstrate the medical necessity and cost-effectiveness of the product, in addition to the costs required to obtain FDA or other comparable marketing approvals. Nonetheless, product candidates may not be considered medically necessary or cost effective. A decision by a third-party payor not to cover a product candidate could reduce physician utilization once the product is approved and have a material adverse effect on sales, results of operations and financial condition. Additionally, a payor’s decision to provide coverage for a product does not imply that an adequate reimbursement rate will be approved. Further, one payor’s determination to provide coverage for a drug product does not assure that other payors will also provide coverage and reimbursement for the product, and the level of coverage and reimbursement can differ significantly from payor to payor.
43
Table of Contents
The containment of healthcare costs also has become a priority of federal, state and foreign governments and the prices of drugs have been a focus in this effort. Governments have shown significant interest in implementing cost-containment programs, including price controls, restrictions on reimbursement and requirements for substitution of generic products. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could further limit a company’s revenue generated from the sale of any approved products. Coverage policies and third-party reimbursement rates may change at any time. Even if favorable coverage and reimbursement status is attained for one or more products for which a company or its collaborators receive marketing approval, less favorable coverage policies and reimbursement rates may be implemented in the future.
Outside the United States, ensuring adequate coverage and payment for a product also involves challenges. Pricing of prescription pharmaceuticals is subject to governmental control in many countries. Pricing negotiations with governmental authorities can extend well beyond the receipt of regulatory marketing approval for a product and may require a clinical trial that compares the cost effectiveness of a product to other available therapies. The conduct of such a clinical trial could be expensive and result in delays in commercialization.
In the European Union, pricing and reimbursement schemes vary widely from country to country. Some countries provide that products may be marketed only after a reimbursement price has been agreed. Some countries may require the completion of additional studies that compare the cost-effectiveness of a particular drug candidate to currently available therapies or so called health technology assessments, in order to obtain reimbursement or pricing approval. For example, the European Union provides options for its member states to restrict the range of products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. European Union member states may approve a specific price for a product or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the product on the market. Other member states allow companies to fix their own prices for products, but monitor and control prescription volumes and issue guidance to physicians to limit prescriptions. Recently, many countries in the European Union have increased the amount of discounts required on pharmaceuticals and these efforts could continue as countries attempt to manage healthcare expenditures, especially in light of the severe fiscal and debt crises experienced by many countries in the European Union. The downward pressure on health care costs in general, particularly prescription drugs, has become intense. As a result, increasingly high barriers are being erected to the entry of new products. Political, economic and regulatory developments may further complicate pricing negotiations, and pricing negotiations may continue after reimbursement has been obtained. Reference pricing used by various European Union member states, and parallel trade, i.e., arbitrage between low-priced and high-priced member states, can further reduce prices. There can be no assurance that any country that has price controls or reimbursement limitations for pharmaceutical products will allow favorable reimbursement and pricing arrangements for any products, if approved in those countries.
Healthcare Law and Regulation
Healthcare providers and third-party payors play a primary role in the recommendation and prescription of drug products that are granted marketing approval. Arrangements with providers, consultants, third-party payors and customers are subject to broadly applicable fraud and abuse, anti-kickback, false claims laws, reporting of payments to physicians and teaching physicians and patient privacy laws and regulations and other healthcare laws and regulations that may constrain business and/or financial arrangements. Restrictions under applicable federal and state healthcare laws and regulations, include the following:
| • | the federal Anti-Kickback Statute, which prohibits, among other things, persons and entities from knowingly and willfully soliciting, offering, paying, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made, in whole or in part, under a federal healthcare program such as Medicare and Medicaid; |
44
Table of Contents
| • | the federal civil and criminal false claims laws, including the civil False Claims Act, and civil monetary penalties laws, which prohibit individuals or entities from, among other things, knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false, fictitious or fraudulent or knowingly making, using or causing to made or used a false record or statement to avoid, decrease or conceal an obligation to pay money to the federal government. |
| • | the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, which created additional federal criminal laws that prohibit, among other things, knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters; |
| • | HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, and their respective implementing regulations, including the Final Omnibus Rule published in January 2013, which impose obligations, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information; |
| • | the federal false statements statute, which prohibits knowingly and willfully falsifying, concealing ·or covering up a material fact or making any materially false statement in connection with the delivery of or payment for healthcare benefits, items or services; |
| • | the federal transparency requirements known as the federal Physician Payments Sunshine Act, under the Patient Protection and Affordable Care Act, as amended by the Health Care Education Reconciliation Act, or the Affordable Care Act, which requires certain manufacturers of drugs, devices, biologics and medical supplies to report annually to the Centers for Medicare & Medicaid Services, or CMS, within the United States Department of Health and Human Services, information related to payments and other transfers of value made by that entity to physicians and teaching hospitals, as well as ownership and investment interests held by physicians and their immediate family members; and |
| • | analogous state and foreign laws and regulations, such as state anti-kickback and false claims laws, which may apply to healthcare items or services that are reimbursed by non-governmental third-party payors, including private insurers. |
Some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government in addition to requiring drug manufacturers to report information related to payments to physicians and other health care providers or marketing expenditures. State and foreign laws also govern the privacy and security of health information in some circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
Healthcare Reform
A primary trend in the United States healthcare industry and elsewhere is cost containment. There have been a number of federal and state proposals during the last few years regarding the pricing of pharmaceutical and biopharmaceutical products, limiting coverage and reimbursement for drugs and other medical products, government control and other changes to the healthcare system in the United States.
By way of example, the United States and state governments continue to propose and pass legislation designed to reduce the cost of healthcare. In March 2010, the United States Congress enacted the Affordable Care Act, which, among other things, includes changes to the coverage and payment for products under government health care programs. Among the provisions of the Affordable Care Act of importance to potential drug candidates are:
| • | an annual, nondeductible fee on any entity that manufactures or imports specified branded prescription drugs and biologic agents, apportioned among these entities according to their market share in certain government healthcare programs, although this fee would not apply to sales of certain products approved exclusively for orphan indications; |
45
Table of Contents
| • | expansion of eligibility criteria for Medicaid programs by, among other things, allowing states to offer Medicaid coverage to certain individuals with income at or below 133% of the federal poverty level, thereby potentially increasing a manufacturer’s Medicaid rebate liability; |
| • | expanded manufacturers’ rebate liability under the Medicaid Drug Rebate Program by increasing the minimum rebate for both branded and generic drugs and revising the definition of “average manufacturer price,” or AMP, for calculating and reporting Medicaid drug rebates on outpatient prescription drug prices and extending rebate liability to prescriptions for individuals enrolled in Medicare Advantage plans; |
| • | addressed a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for drugs that are inhaled, infused, instilled, implanted or injected; |
| • | expanded the types of entities eligible for the 340B drug discount program; |
| • | established the Medicare Part D coverage gap discount program by requiring manufacturers to provide a 50% point-of-sale-discount off the negotiated price of applicable brand drugs to eligible beneficiaries during their coverage gap period as a condition for the manufacturers’ outpatient drugs to be covered under Medicare Part D; |
| • | a new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research; |
| • | the Independent Payment Advisory Board, or IPAB, which has authority to recommend certain changes to the Medicare program to reduce expenditures by the program that could result in reduced payments for prescription drugs. However, the IPAB implementation has been not been clearly defined. PPACA provided that under certain circumstances, IPAB recommendations will become law unless Congress enacts legislation that will achieve the same or greater Medicare cost savings; and |
| • | established the Center for Medicare and Medicaid Innovation within CMS to test innovative payment and service delivery models to lower Medicare and Medicaid spending, potentially including prescription drug spending. Funding has been allocated to support the mission of the Center for Medicare and Medicaid Innovation from 2011 to 2019. |
Other legislative changes have been proposed and adopted in the United States since the Affordable Care Act was enacted. For example, in August 2011, the Budget Control Act of 2011, among other things, created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion for the years 2012 through 2021, was unable to reach required goals, thereby triggering the legislation’s automatic reduction to several government programs. This includes aggregate reductions of Medicare payments to providers of up to 2% per fiscal year, which went into effect in April 2013 and will remain in effect through 2024 unless additional Congressional action is taken. In January 2013, President Obama signed into law the American Taxpayer Relief Act of 2012, which, among other things, further reduced Medicare payments to several providers, including hospitals, imaging centers and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years.
Review and Approval of Animal Drugs in the United States
In addition to pursuing approval of our drug candidates for use in human beings, we may also seek approval of certain drug candidates for veterinary applications. As with new drug products for human beings, new animal drugs may not be marketed in the United States until they have been approved by the FDA as safe and effective. The requirements and phases governing approval of a new animal drug are analogous to those for new human drugs. Specifically, the Center for Veterinary Medicine or CVM at FDA is responsible for determining whether a new veterinary product should be approved on the basis of a NADA filed by the applicant. A NADA must contain substantial evidence of the safety and effectiveness of the animal drug, as well as data and controls
46
Table of Contents
demonstrating that the product will be manufactured and studied in compliance with, among other things, applicable cGMP and GLP practices.
To begin this process, an applicant must file an Investigational New Animal Drug application, or INAD, with the CVM. The applicant will hold a pre-development meeting with the CVM to reach general agreement on the plans for providing the data necessary to fulfill requirements for a NADA. In this context, an applicant must submit pivotal protocols to the CVM for review and concurrence prior to conducting the required studies. The applicant will gather and submit data on safety, efficacy and chemistry, manufacturing and controls or CMC to the CVM for review, as below:
| Safety: | The design and review of the safety study and the study protocol are completed prior to initiation of the study to help assure that the data generated will meet FDA requirements. These studies are conducted under rigorous quality control, including GLP, to assure integrity of the data. They are designed to clearly define a safety margin, identify any potential safety concerns, and establish a safe dose for the product. This dose and effectiveness is then evaluated in the pivotal field efficacy study where the product is studied in the animal patient population in which the product is intended to be used. |
| Efficacy: | Early pilot studies may be done in laboratory cats or dogs to establish effectiveness and the dose range for each product. When an effective dose is established, a study protocol to test the product in real world conditions is developed prior to beginning the study. The pivotal field efficacy study protocol is submitted for review and concurrence prior to study initiation, to help assure that the data generated will meet requirements. This study must be conducted with the formulation of the product that is intended to be commercialized, and is a multi-site, randomized, controlled study, generally with a placebo control. |
| CMC: | To assure that the new animal drug product can be manufactured consistently, FDA will require applicants to provide documentation of the process by which the active ingredient is made and the controls applicable to that process that assure the active ingredient and the formulation of the final commercial product meet certain criteria, including purity and stability. After a product is approved, applicants will be required to communicate with FDA before any changes are made to these procedures or at the manufacturing site. Both the active ingredient and commercial formulations are required to be manufactured at facilities that practice cGMP. |
Once all data have been submitted and reviewed for each technical section—safety, efficacy and CMC—the CVM will issue a technical section complete letter as each section review is completed. When the three letters have been issued, the applicant will compile a draft of the Freedom of Information Summary, the proposed labeling, and all other relevant information, and submit these as an administrative NADA for CVM review. Generally, if there are no deficiencies in the submission, the NADA will be issued within four to six months after submission of the administrative NADA. This review will be conducted according to timelines specified in the Animal Drug User Fee Act. The FDA’s basis for approving a NADA is documented in a Freedom of Information Summary. Post-approval monitoring of products is required by law, with reports being provided to the CVM’s Surveillance and Compliance group. Reports of product quality defects, adverse events or unexpected results must also be produced in accordance with the relevant regulatory requirements.
Employees
As of March 1, 2016, we had 105 full-time employees, 77 of whom were primarily engaged in research and development activities and 27 of whom had an M.D. or Ph.D. degree.
47
Table of Contents
Executive Officers of the Company
The following table lists the positions, names and ages of our executive officers as of March 1, 2016:
| Name |
Age | Position | ||||
| Michael G. Kauffman, M.D., Ph.D. |
52 | Chief Executive Officer and Director | ||||
| Sharon Shacham, Ph.D., M.B.A. |
45 | President and Chief Scientific Officer | ||||
| Justin A. Renz, C.P.A., M.S.T., M.B.A. |
44 | Executive Vice President, Chief Financial Officer and Treasurer | ||||
| Ran Frenkel, RPh. |
47 | Chief Development Operations Officer | ||||
| Christopher B. Primiano, J.D., M.B.A. |
35 | Senior Vice President, Corporate Development, General Counsel and Secretary | ||||
Michael G. Kauffman, M.D., Ph.D. Dr. Kauffman has served as Karyopharm’s Chief Executive Officer since January 2011 and has been one of our directors since 2008. Dr. Kauffman co-founded Karyopharm with Dr. Sharon Shacham in 2008 and served as our President from January 2011 to December 2013 and as Chief Medical Officer from December 2012 to December 2013. Prior to joining Karyopharm, he was Chief Medical Officer of Onyx Pharmaceuticals Inc., a biopharmaceutical company, from November 2009 to December 2010. From November 2008 to November 2009, Dr. Kauffman was Chief Medical Officer of Proteolix Inc., which was acquired by Onyx Pharmaceuticals. At Proteolix, he led the development of Kyprolis® (carfilzomib), a novel proteasome inhibitor approved in refractory myeloma by the FDA in July 2012. Dr. Kauffman was an operating partner at Bessemer Venture Partners from 2006 to 2008, where he led investments in biotechnology companies. From 2006 to 2008, he was President and Chief Executive Officer of Epix Pharmaceuticals, Inc., a biopharmaceutical company that underwent liquidation proceedings through an assignment for the benefit of creditors under Massachusetts law in 2009. Dr. Kauffman was President and Chief Executive Officer of Predix Pharmaceuticals, Inc., a private biopharmaceutical company focused on G protein-coupled receptors (GPCR), from 2002 until its merger into Epix Pharmaceuticals in 2006. In that role, he led the merger of Predix Pharmaceuticals and Epix Pharmaceuticals, oversaw the discovery and development of four new clinical candidates and led collaboration transactions with Amgen and GlaxoSmithKline. From March 2000 to September 2002, Dr. Kauffman was Vice President, Clinical at Millennium Pharmaceuticals, Inc., a biopharmaceutical company, where he led the Velcade® development program. From September 1997 to March 2000, Dr. Kauffman held a number of senior positions at Millennium Predictive Medicine, Inc., a biopharmaceutical company and a subsidiary of Millennium Pharmaceuticals, where he led the discovery and development of novel molecular diagnostics for major cancers, including melanoma, and led transactions with Becton-Dickenson and Bristol Myers Squibb. From August 1995 to September 1997, Dr. Kauffman held a number of senior positions at Biogen Idec, Inc., a biopharmaceutical company, where he led the clinical development of anti-CD40L antibodies in autoimmune and inflammatory diseases, and acted as the main medical advisor to the Biogen business development group. Dr. Kauffman currently serves on the board of directors and compensation committee of Verastem Inc., a public biopharmaceutical company, and on the board of directors and the compensation committee of Metamark Genetics Inc., a private molecular diagnostics company. Dr. Kauffman previously served on the board of directors and compensation and audit committees of Zalicus Inc., a biotechnology company. Dr. Kauffman received his B.A. in Biochemistry from Amherst College and his M.D. and Ph.D. from Johns Hopkins Medical School, and he trained in internal medicine and rheumatology at Beth Israel (now Beth Israel Deaconess Medical Center) and Massachusetts General Hospitals. He is board certified in internal medicine.
Sharon Shacham, Ph.D., M.B.A. Dr. Shacham founded Karyopharm in 2008 and has served as our President since December 2013, and as our Chief Scientific Officer since October 2010. Dr. Shacham served as our President of Research and Development from December 2012 to December 2013, as our Head of Research and Development from October 2010 to December 2012 and as our President and Chief Executive Officer from October 2010 to January 2011. Dr. Shacham established the company to focus on the discovery and development of small molecule inhibitors of nuclear export and has led our scientific progress since inception. Her
48
Table of Contents
computational drug discovery algorithms formed a critical part of the technological basis for our drug discovery and optimization expertise, which was used for the discovery of selinexor, our lead drug candidate. Dr. Shacham co-chairs our Scientific Advisory Board. Prior to founding Karyopharm, from 2006 to April 2009, she was Senior Vice President of Drug Development at Epix Pharmaceuticals, Inc., a biopharmaceutical company that underwent liquidation proceedings through an assignment for the benefit of creditors under Massachusetts law in 2009. She was Director, Algorithm and Software Development at Predix Pharmaceuticals Inc. from July 2000 until Predix’s merger into Epix Pharmaceuticals in 2006, where she led the company’s efforts in GPCR modeling, computational chemistry, lead optimization and development of clinical trials. Dr. Shacham received her B.Sc. in Chemistry, Ph.D. and M.B.A. from Tel Aviv University.
Justin A. Renz, C.P.A., M.S.T., M.B.A. Mr. Renz joined Karyopharm in August 2014 as Executive Vice President and Chief Financial Officer. Prior to joining Karyopharm, Mr. Renz served most recently as Executive Vice President, Chief Financial Officer and Treasurer at Zalicus Inc. (formerly CombinatoRx, Inc.), a biopharmaceutical company, which he joined in September 2006. Mr. Renz led core business and finance functions at Zalicus, oversaw multiple rounds of equity and debt financing and led the company’s asset monetization strategy. More recently, Mr. Renz was instrumental in the reverse merger and sale of Zalicus to EPIRUS Biopharmaceuticals Inc. in July 2014. Prior to Zalicus, Mr. Renz served in senior finance and accounting roles at Serono, Inc. and Coley Pharmaceutical Group, Inc. Earlier in his career, Mr. Renz held increasingly senior finance positions at ArQule, Inc. and Millipore Corporation. Mr. Renz began his career with Arthur Andersen LLP in 1993. Mr. Renz received a B.A. in Economics and Accounting from the College of the Holy Cross, an M.S. in Taxation from Northeastern University and an M.B.A. from Suffolk University.
Ran Frenkel, RPh. Mr. Frenkel has served as Karyopharm’s Chief Development Operations Officer since January 2015 and was Executive Vice President, Worldwide Development Operations from October 2014 to January 2015. Prior to joining Karyopharm, Mr. Frenkel held a number of senior management roles in Europe, Israel and the United States, most recently as Managing Director EMEA from January 2013 to October 2014 for Clinipace Worldwide, an international clinical research organization, where he had responsibility for the overall management of the organization in Europe, the Middle East and Africa. Prior to becoming Managing Director EMEA, Mr. Frenkel was VP International Business Development at Clinipace Worldwide from July 2011 to January 2013. Prior to joining Clinipace Worldwide, from January 2007 to August 2011, Mr. Frenkel established and managed the Israeli office of PFC Pharma Focus AG, a contract research organizationacquired by Clinipace Worldwide in 2011, and from 2004 to 2007, he held the position of Managing Director at Actelion Pharmaceuticals with responsibility for all science and business affairs of the company in Israel. Mr. Frenkel received a BPharm from Hebrew University.
Christopher B. Primiano, J.D., M.B.A. Mr. Primiano has served as Senior Vice President, Corporate Development, General Counsel and Secretary since September 2015 and was Vice President, Corporate Development, General Counsel and Secretary from March 2014 to September 2015. Prior to joining Karyopharm, Mr. Primiano was a Counsel at Wilmer Cutler Pickering Hale and Dorr LLP, where he had practiced law since October 2012. From August 2010 to August 2012, he served as Vice President, Corporate Development, General Counsel and Secretary of GlassHouse Technologies, Inc., an information technology consulting company, where he led global legal operations and managed asset and subsidiary acquisition and sale activity. Mr. Primiano began his career at Gunderson Dettmer Stough Villeneuve Franklin & Hachigian LLP, where he practiced law from August 2006 to July 2010. Mr. Primiano received a B.A. in Political Economy and English from Georgetown University, an M.B.A. from the Boston College Carroll School of Management and a J.D. from Boston College Law School.
Our Corporate Information
Karyopharm was incorporated under the laws of the state of Delaware on December 22, 2008 under the name Karyopharm Therapeutics Inc. Our principal executive offices are located at 85 Wells Avenue, 2nd Floor, Newton, Massachusetts 02459. Our telephone number is (617) 658-0600, and our website is located at
49
Table of Contents
www.karyopharm.com. References to our website are inactive textual references only and the content of our website should not be deemed incorporated by reference into this Form 10-K.
Available Information
Our Internet website is http://www.karyopharm.com. We make available free of charge through our website our annual report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Sections 13(a) and 15(d) of the Securities Exchange Act of 1934, as amended, or the Exchange Act. We make these reports available through our website as soon as reasonably practicable after we electronically file such reports with, or furnish such reports to, the U.S. Securities and Exchange Commission, or SEC. In addition, we regularly use our website to post information regarding our business, development programs and governance, and we encourage investors to use our website, particularly the information in the section entitled “Investors” as a source of information about us. You may also read and copy any materials we file with the SEC at the SEC’s Public Reference Room at 100 F Street, NE, Washington, DC 20549. Members of the public may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. The SEC also maintains a website at http://www.sec.gov that contains reports, proxy and information statements and other information regarding issuers that file electronically with the SEC.
Our Code of Business Conduct and Ethics, Corporate Governance Guidelines and the charters of the Audit, Compensation and Nominating and Corporate Governance Committees of our board of directors are all available on our website at http://www.karyopharm.com at the “Investors” section under “Corporate Governance”. Stockholders may request a free copy of any of these documents by writing to Investor Relations, Karyopharm Therapeutics Inc., 85 Wells Avenue, 2nd floor, Newton, Massachusetts 02459, U.S.A.
50
Table of Contents
| ITEM 1A. | RISK FACTORS |
Careful consideration should be given to the following risk factors, in addition to the other information set forth in this Annual Report on Form 10-K and in other documents that we file with the SEC, in evaluating the Company and our business. Investing in our common stock involves a high degree of risk. If any of the following risks and uncertainties actually occurs, our business, prospects, financial condition and results of operations could be materially and adversely affected. The risks described below are not intended to be exhaustive and are not the only risks facing the Company. New risk factors can emerge from time to time, and it is not possible to predict the impact that any factor or combination of factors may have on our business, prospects, financial condition and results of operations.
Risks Related to the Discovery, Development and Commercialization of Our Drug Candidates
We depend heavily on the success of our lead drug candidate selinexor (KPT-330), which is currently in clinical trials. Our clinical trials of selinexor may not be successful. If we are unable to commercialize selinexor or experience significant delays in doing so, our business will be materially harmed.
We have invested a significant portion of our efforts and financial resources in the research and development of our lead drug candidate, selinexor. Our ability to generate revenues from the sale of drugs that treat cancer and other diseases in humans, which we do not expect to occur for several years, if ever, will depend heavily on the successful development, regulatory approval and eventual commercialization of selinexor.
We cannot commercialize drug candidates in the United States without first obtaining regulatory approval for the drug from the United States Food and Drug Administration, or FDA; similarly, we cannot commercialize drug candidates outside of the United States without obtaining regulatory approval from similar regulatory authorities outside of the United States. Even if selinexor or another drug candidate were to successfully obtain approval from the FDA and non-U.S. regulatory authorities, any approval might contain significant limitations related to use restrictions for specified age groups, warnings, precautions or contraindications, or may be subject to burdensome post-approval study or risk management requirements. If we are unable to obtain regulatory approval for selinexor in one or more jurisdictions, or any approval contains significant limitations, we may not be able to obtain sufficient funding or generate sufficient revenue to continue the development, marketing and/or commercialization of selinexor or any other drug candidate that we may discover, in-license, develop or acquire in the future. Furthermore, even if we obtain regulatory approval for selinexor, we will still need to develop a commercial organization, or collaborate with a third party for the commercialization of selinexor, establish commercially viable pricing and obtain approval for adequate reimbursement from third-party and government payors. If we or our commercialization collaborators are unable to successfully commercialize selinexor, we may not be able to generate sufficient revenues to continue our business.
The results of previous clinical trials may not be predictive of future results, and the results of our current and planned clinical trials may not satisfy the requirements of the FDA or non-U.S. regulatory authorities.
We currently have no drugs approved for sale and we cannot guarantee that we will ever have marketable drugs. Clinical failure can occur at any stage of clinical development. Clinical trials may produce negative or inconclusive results, and we or any future collaborators may decide, or regulators may require us, to conduct additional clinical trials or preclinical studies. We will be required to demonstrate with substantial evidence through well-controlled clinical trials that our drug candidates are safe and effective for use in a diverse population before we can seek regulatory approvals for their commercial sale. Success in early-stage clinical trials does not mean that future larger registration clinical trials will be successful because drug candidates in later-stage clinical trials may fail to demonstrate sufficient safety and efficacy to the satisfaction of the FDA and non-U.S. regulatory authorities despite having progressed through early-stage clinical trials. Drug candidates that have shown promising results in early-stage clinical trials may still suffer significant setbacks in subsequent registration clinical trials. Additionally, the outcome of preclinical studies and early-stage clinical trials may not be predictive of the success of later-stage clinical trials and interim results of a clinical trial are not necessarily indicative of final results.
51
Table of Contents
In addition, the design of a clinical trial can determine whether its results will support approval of a drug and flaws in the design of a clinical trial may not become apparent until the clinical trial is well advanced. We have limited experience in designing clinical trials and may be unable to design and conduct a clinical trial to support regulatory approval. Further, if our drug candidates are found to be unsafe or lack efficacy, we will not be able to obtain regulatory approval for them and our business would be harmed. A number of companies in the pharmaceutical industry, including those with greater resources and experience than us, have suffered significant setbacks in advanced clinical trials, even after obtaining promising results in earlier clinical trials.
In some instances, there can be significant variability in safety and/or efficacy results between different trials of the same drug candidate due to numerous factors, including changes in trial protocols, differences in size and type of the patient populations, adherence to the dosing regimen and other trial protocols and the rate of dropout among clinical trial participants. We do not know whether any Phase 2, Phase 3 or other clinical trials we may conduct will demonstrate consistent or adequate efficacy and safety sufficient to obtain regulatory approval to market our drug candidates.
Further, our drug candidates may not be approved even if they achieve their primary endpoints in Phase 3 clinical trials or other registration trials. The FDA or non-U.S. regulatory authorities may disagree with our trial design and our interpretation of data from preclinical studies and clinical trials. In addition, any of these regulatory authorities may change requirements for the approval of a drug candidate even after reviewing and providing comments or advice on a protocol for a clinical trial that has the potential to result in approval by the FDA or another regulatory authority. In addition, any of these regulatory authorities may also approve a drug candidate for fewer or more limited indications than we request or may grant approval contingent on the performance of costly post-marketing clinical trials. In addition, the FDA or other non-U.S. regulatory authorities may not approve the labeling claims that we believe would be necessary or desirable for the successful commercialization of our drug candidates.
To date, we have had limited discussions with the FDA and non-U.S. regulatory authorities regarding the design of our later phase clinical trials for selinexor, of which we have commenced five such clinical trials. We plan to seek regulatory approvals of selinexor in North America and Europe in each indication with respect to which such later phase clinical trial is being conducted and with respect to which we receive positive results that may support full or accelerated approval, as the case may be. We may also seek such approvals in other geographies. We cannot be certain that we will commence additional later phase trials or complete ongoing later phase trials as anticipated. Before obtaining regulatory approvals for the commercial sale of any drug candidate for a target indication, we must demonstrate with substantial evidence gathered in preclinical studies and well-controlled clinical studies, and, with respect to approval in the United States, to the satisfaction of the FDA, that the drug candidate is safe and effective for use for that target indication. There is no assurance that the FDA or non-U.S. regulatory authorities would consider our current and planned later phase clinical trials to be sufficient to serve as the basis for filing for approval or to gain approval of selinexor for any indication. The FDA and non-U.S. regulatory authorities retain broad discretion in evaluating the results of our clinical trials and in determining whether the results demonstrate that selinexor is safe and effective. If we are required to conduct additional clinical trials of selinexor prior to approval, including additional earlier phase clinical trials that may be required prior to commencing any later phase clinical trials, or additional clinical trials following completion of our current and planned later phase clinical trials, we will need substantial additional funds and there is no assurance that the results of any such additional clinical trials will be sufficient for approval.
The results to date in preclinical and early clinical studies conducted by us or our academic collaborators and in Phase 1 and Phase 2 clinical trials that we are currently conducting include the response of tumors to selinexor. We expect that in any later phase clinical trial where patients are randomized to receive either selinexor on the one hand, or standard of care, supportive care or placebo on the other hand, the primary endpoint will be either progression free survival, meaning the length of time on treatment until objective tumor progression, or overall survival, while the primary endpoint in any later phase clinical trial that is not similarly randomized may be different. For example, the primary endpoint of our SOPRA study, the clinical trial of
52
Table of Contents
selinexor in patients over 60 years of age with relapsed and/or refractory acute myeloid leukemia (AML) in first relapse, who are not candidates for intensive chemotherapy or transplantation, is overall survival. Similarly, the primary endpoint of our SEAL study, the clinical trial of selinexor in patients with dedifferentiated liposarcoma, is progression free survival. We are in the early stages of collecting clinical data in humans relating to the impact of selinexor on overall survival and comparative clinical data between selinexor and supportive care. If selinexor does not demonstrate an overall survival benefit, it will likely not be approved. In some instances, the FDA and other regulatory bodies have accepted overall response rate as a surrogate for a clinical benefit, and have granted regulatory approvals based on this or other surrogate endpoints. Overall response rate is defined as the portion of patients with tumor size reduction of a predefined amount for a minimum time period. For some types of cancer, we may use overall response rate as a primary endpoint, as we are doing in our Selinexor Against Diffuse Aggressive Lymphoma (SADAL) study; our Selinexor In Initial or Relapsed/Refractory Richter’s Transformation (SIRRT) study and our Selinexor Treatment Of Refractory Myeloma (STORM) study. These clinical trials will not be randomized against control arms and the primary endpoints of these trials are overall response rate. If selinexor does not demonstrate sufficient overall response rates in these indications, or any other indication for which a clinical trial has overall response rate as a primary endpoint, or if the FDA or non-U.S. regulatory authorities do not deem overall response rate a sufficient endpoint, it will likely not be approved for that indication.
We are early in our development efforts with a limited number of drug candidates in human clinical development. If we are unable to successfully develop and commercialize our drug candidates or experience significant delays in doing so, our business will be materially harmed.
We are early in our development efforts and have three drug candidates, selinexor, verdinexor and KPT-8602, in clinical development for treatment of human diseases. The success of these and any of our other drug candidates will depend on several factors, including the following:
| • | successful completion of preclinical studies; |
| • | successful enrollment in, and completion of, clinical trials, including demonstration of a favorable risk-benefit ratio; |
| • | receipt of marketing approvals from applicable regulatory authorities; |
| • | establishing commercial manufacturing capabilities or making arrangements with third-party manufacturers; |
| • | obtaining and maintaining patent and trade secret protection and regulatory exclusivity for our drug candidates; |
| • | establishing sales, marketing, manufacturing and distribution capabilities to commercialize any drugs for which we may obtain marketing approval; |
| • | launching commercial sales of the drugs, if and when approved, whether alone or in collaboration with others; |
| • | acceptance of the drugs, if and when approved, by patients, the medical community and third-party payors; |
| • | effectively competing with other therapies; |
| • | obtaining and maintaining coverage and adequate reimbursement by third-party payors, including government payors, for any approved drugs; |
| • | maintaining an acceptable safety profile of the drugs following approval; |
| • | enforcing and defending intellectual property rights and claims; and |
| • | maintaining and growing an organization of scientists and business people, and possibly collaborators, who can develop and commercialize our drug candidates. |
53
Table of Contents
If we do not achieve one or more of these factors in a timely manner or at all, we could experience significant delays or an inability to successfully commercialize our drug candidates, which would materially harm our business.
We may seek approval from the FDA or comparable non-U.S. regulatory authorities to use accelerated development pathways for our product candidates. If we are not able to use such pathways, we may be required to conduct additional clinical trials beyond those that we contemplate and that would increase the expense of obtaining, and delay the receipt of, necessary marketing approvals, if we receive them at all. In addition, even if we are able to use an accelerated approval pathway, it may not lead to expedited approval of our product candidates.
Under the Federal Food, Drug and Cosmetic Act, or FDCA, and implementing regulations, the FDA may grant accelerated approval to a product candidate to treat a serious or life-threatening condition that provides meaningful therapeutic benefit over available therapies, upon a determination that the product has an effect on a surrogate endpoint or intermediate clinical endpoint that is reasonably likely to predict clinical benefit. The FDA considers a clinical benefit to be a positive therapeutic effect that is clinically meaningful in the context of a given disease, such as irreversible morbidity or mortality. For the purposes of accelerated approval, a surrogate endpoint is a marker, such as a laboratory measurement, radiographic image, physical sign, or other measure that is thought to predict clinical benefit, but is not itself a measure of clinical benefit. An intermediate clinical endpoint is a clinical endpoint that can be measured earlier than an effect on irreversible morbidity or mortality that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit measurement of a therapeutic effect that is considered reasonably likely to predict the clinical benefit of a drug. The accelerated approval pathway may be used in cases in which the advantage of a new drug over available therapy may not be a direct therapeutic advantage, but is a clinically important improvement from a patient and public health perspective.
Prior to seeking such accelerated approval, we will seek feedback from the FDA and will otherwise evaluate our ability to seek and receive such accelerated approval. There can be no assurance that the FDA will agree with our surrogate endpoints or intermediate clinical endpoints. There can also be no assurance that we will decide to pursue or submit an NDA for accelerated approval or any other form of expedited development, review or approval. Similarly, there can be no assurance that, after feedback from FDA, we will continue to pursue or apply for accelerated approval or any other form of expedited development, review or approval, even if we initially decide to do so. Furthermore, if we decide to submit an application for accelerated approval or under another expedited regulatory designation, there can be no assurance that such submission or application will be accepted or that any expedited development, review or approval will be granted on a timely basis, or at all.
Moreover, for drugs granted accelerated approval, the FDA typically requires post-marketing confirmatory trials to evaluate the anticipated effect on irreversible morbidity or mortality or other clinical benefit. These confirmatory trials must be completed with due diligence. The FDA may withdraw approval of our product candidate approved under the accelerated approval pathway if, for example, the trial required to verify the predicted clinical benefit of our product candidate fails to verify such benefit or does not demonstrate sufficient clinical benefit to justify the risks associated with the drug. The FDA may also withdraw approval if other evidence demonstrates that our product candidate is not shown to be safe or effective under the conditions of use, we fail to conduct any required post approval trial of our product candidate with due diligence, or we disseminate false or misleading promotional materials relating to our product candidate. A failure to obtain accelerated approval or any other form of expedited development, review or approval for our product candidates, or withdrawal of a product candidate, would result in a longer time period for commercialization of such product candidate, could increase the cost of development of such product candidate and could harm our competitive position in the marketplace.
54
Table of Contents
Our approach to the discovery and development of drug candidates that target Exportin 1, or XPO1, is unproven, and we do not know whether we will be able to develop any drugs of commercial value. If selinexor is unsuccessful in proving that drug candidates targeting XPO1 have commercial value or experiences significant delays in doing so, our business may be materially harmed.
Our SINE™ compounds inhibit the nuclear export protein XPO1. We believe that no currently approved cancer treatments are selectively targeting the restoration and increase in the levels of multiple tumor suppressor proteins in the nucleus. Despite promising results to date in preclinical and early clinical studies of selinexor that we have conducted and in Phase 1 and Phase 2 clinical trials of selinexor conducted by us or our academic collaborators, we may not succeed in demonstrating safety and efficacy of SINE™ compounds in our current and future human clinical trials. Any drug candidates that we develop may not effectively prevent the exportation of tumor suppressor and/or growth regulatory proteins from the nucleus in humans with a particular form of cancer. If selinexor is unsuccessful in proving that drug candidates targeting the regulation of intracellular transport of XPO1 have commercial value or experiences significant delays in doing so, our business may be materially harmed and we may not be able to generate sufficient revenues to continue our business.
We may not be successful in our efforts to identify or discover additional potential drug candidates.
Part of our strategy involves identifying and developing drug candidates to build a pipeline of novel drug candidates. Our drug discovery efforts may not be successful in identifying compounds that are useful in treating cancer or other diseases. Our research programs may initially show promise in identifying potential drug candidates, yet fail to yield drug candidates for clinical development for a number of reasons, including:
| • | the research methodology used may not be successful in identifying potential drug candidates; |
| • | potential drug candidates may, on further study, be shown to have harmful side effects or other characteristics that indicate that they are unlikely to be drugs that will receive marketing approval and/or achieve market acceptance; or |
| • | potential drug candidates may not be effective in treating their targeted diseases. |
Research programs to identify new drug candidates require substantial technical, financial and human resources. We may choose to focus our efforts and resources on a potential drug candidate that ultimately proves to be unsuccessful.
If we are unable to identify suitable compounds for preclinical and clinical development, we will not be able to obtain revenues from sale of drugs in future periods, which likely would result in significant harm to our financial position and adversely impact our stock price.
Clinical drug development is a lengthy and expensive process, with an uncertain outcome. If clinical trials of our drug candidates fail to demonstrate safety and efficacy to the satisfaction of regulatory authorities or do not otherwise produce positive results, we may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of our drug candidates.
Before obtaining marketing approval from regulatory authorities for the sale of our drug candidates, we must complete preclinical development and then conduct extensive clinical trials to demonstrate the safety and efficacy of our drug candidates in humans. Clinical testing is expensive, difficult to design and implement, can take many years to complete and is uncertain as to outcome. A failure of one or more clinical trials can occur at any stage of testing. The outcome of preclinical studies and early-stage clinical trials may not be predictive of the success of later clinical trials, and interim results of a clinical trial do not necessarily predict final results. For example, the results of our Phase 1 and Phase 2 clinical trials of selinexor to date are based on unaudited data provided by our clinical trial investigators. An audit of this data may change the conclusions drawn from this unaudited data provided by our clinical trial investigators indicating less promising results than we currently anticipate. Moreover, preclinical and clinical data are often susceptible to varying interpretations and analyses,
55
Table of Contents
and many companies that believed their drug candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval of their drugs.
We may experience numerous unforeseen events during, or as a result of, clinical trials that could delay or prevent our ability to receive marketing approval or commercialize our drug candidates, including:
| • | regulatory authorities or institutional review boards may not authorize us or our investigators to commence a clinical trial or conduct a clinical trial at a prospective trial site; |
| • | feedback from regulatory authorities that requires us to modify the design of our clinical trials; |
| • | we may have delays in reaching or fail to reach agreement on acceptable clinical trial contracts or clinical trial protocols with prospective trial sites or contract research organizations; |
| • | clinical trials of our drug candidates may produce negative or inconclusive results, and we may decide, or regulatory authorities may require us, to conduct additional clinical trials, suspend ongoing clinical trials or abandon drug development programs; |
| • | the number of patients required for clinical trials of our drug candidates may be larger than we anticipate, enrollment in these clinical trials may be slower than we anticipate or participants may drop out of these clinical trials at a higher rate than we anticipate; |
| • | our third-party contractors may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all; |
| • | we or our investigators might have to suspend or terminate clinical trials of our drug candidates for various reasons, including non-compliance with regulatory requirements, a finding that our drug candidates have undesirable side effects or other unexpected characteristics, or a finding that the participants are being exposed to unacceptable health risks; |
| • | the cost of clinical trials of our drug candidates may be greater than we anticipate; |
| • | the supply or quality of our drug candidates or other materials necessary to conduct clinical trials of our drug candidates may be insufficient or inadequate; |
| • | regulators may revise the requirements for approving our drug candidates, or such requirements may not be as we anticipate; and |
| • | any future collaborators that conduct clinical trials may face any of the above issues, and may conduct clinical trials in ways they view as advantageous to them but that are suboptimal for us. |
If we are required to conduct additional clinical trials or other testing of our drug candidates beyond those that we currently contemplate, if we are unable to successfully complete clinical trials of our drug candidates or other testing, if the results of these trials or tests are not positive or are only modestly positive or if there are safety concerns, we may:
| • | be delayed in obtaining marketing approval for our drug candidates; |
| • | not obtain marketing approval at all; |
| • | obtain marketing approval in some countries and not in others; |
| • | obtain approval for indications or patient populations that are not as broad as intended or desired; |
| • | obtain approval with labeling that includes significant use or distribution restrictions or safety warnings, including boxed warnings; |
| • | be subject to additional post-marketing testing requirements; or |
| • | have the drug removed from the market after obtaining marketing approval. |
56
Table of Contents
Our drug development costs will also increase if we experience delays in testing or marketing approvals. We do not know whether clinical trials will begin as planned, will need to be restructured or will be completed on schedule, or at all. Significant clinical trial delays also could shorten any periods during which we may have the exclusive right to commercialize our drug candidates, allow our competitors to bring drugs to market before we do or impair our ability to successfully commercialize our drug candidates, which would harm our business and results of operations.
If we experience delays or difficulties in the enrollment of patients in clinical trials, our receipt of necessary regulatory approvals could be delayed or prevented.
We may not be able to initiate or continue clinical trials for our drug candidates if we are unable to locate and enroll a sufficient number of eligible patients to participate in these trials as required by the FDA or similar regulatory authorities outside of the United States. In addition, some of our competitors may have ongoing clinical trials for drug candidates that treat the same indications as our drug candidates, and patients who would otherwise be eligible for our clinical trials may instead enroll in clinical trials of our competitors’ drug candidates.
Patient enrollment is affected by other factors, including:
| • | severity of the disease under investigation; |
| • | availability and efficacy of approved drugs for the disease under investigation; |
| • | patient eligibility criteria for the study in question; |
| • | competing drugs in clinical development; |
| • | perceived risks and benefits of the drug candidate under study; |
| • | efforts to facilitate timely enrollment in clinical trials; |
| • | patient referral practices of physicians; |
| • | the ability to monitor patients adequately during and after treatment; and |
| • | proximity and availability of clinical trial sites for prospective patients. |
Our inability to enroll a sufficient number of patients for our clinical trials would result in significant delays or may require us to abandon one or more clinical trials altogether. Enrollment delays in our clinical trials may result in increased development costs for our drug candidates, which would cause the value of our company to decline and limit our ability to obtain additional financing.
If serious adverse or unacceptable side effects are identified during the development of our drug candidates or we observe limited efficacy of our drug candidates, we may need to abandon or limit the development of one or more of our drug candidates.
Three of our drug candidates are in clinical development for treatment of human diseases and our other drug candidates for human diseases are in preclinical development. Their risk of failure is high. It is impossible to predict when or if any of our drug candidates will prove effective or safe in humans or will receive marketing approval. If our drug candidates are associated with undesirable side effects or have characteristics that are unexpected, we may need to abandon their development or limit development to certain uses or subpopulations in which the undesirable side effects or other characteristics are less prevalent, less severe or more acceptable from a risk-benefit perspective. For example, we have modified our informed consent form and advised patients already enrolled in our clinical trials of the potential for worsening of pre-existing cataracts as a result of treatment with selinexor. Also, even though selinexor has generally been well-tolerated by patients in our Phase 1 and Phase 2 clinical trials to date, in some cases there were adverse events, some of which were serious. The
57
Table of Contents
most common drug-related adverse events, or AEs, were gastrointestinal, such as nausea, anorexia, diarrhea and vomiting, and fatigue. These side effects were generally mild or moderate in severity. The most common AEs that were Grade 3 or Grade 4, meaning they were more than mild or moderate in severity, were thrombocytopenia, or low count of platelets in the blood, and neutropenia, or low neutrophil counts. We also noted an increase in the rates of sepsis in patients with acute myeloid leukemia, or AML, who received high doses of selinexor, typically 100mg or higher. A small percentage of patients have withdrawn from our clinical trials as a result of AEs. A small percentage of patients across our clinical trials have experienced serious adverse events, or SAEs, deemed by us and the clinical investigator to be related to selinexor. SAEs generally refer to AEs that result in death, are life threatening, require hospitalization or prolonging of hospitalization, or cause a significant and permanent disruption of normal life functions, congenital anomalies or birth defects, or require intervention to prevent such an outcome.
As a result of these adverse events or further safety or toxicity issues that we may experience in our clinical trials in the future, we may not receive approval to market any drug candidates, which could prevent us from ever generating revenue from the sale of drugs or achieving profitability. Results of our trials could reveal an unacceptably high severity and prevalence of side effects. In such an event, our trials could be suspended or terminated and the FDA or comparable foreign regulatory authorities could order us to cease further development of or deny approval of our drug candidates for any or all targeted indications. Many compounds that initially showed promise in early-stage trials for treating cancer or other diseases have later been found to cause side effects that prevented further development of the compound.
The FDA or non-U.S. regulatory authorities may disagree with our and/or our clinical trial investigators’ interpretation of data from clinical trials in determining if serious adverse or unacceptable side effects are drug-related.
We, and our clinical trial investigators, currently determine if serious adverse or unacceptable side effects are drug-related. The FDA or non-U.S. regulatory authorities may disagree with our or our clinical trial investigators’ interpretation of data from clinical trials and the conclusion by us or our clinical trial investigators that a serious adverse effect or unacceptable side effect was not drug-related. The FDA or non-U.S. regulatory authorities may require more information, including additional preclinical or clinical data to support approval, which may cause us to incur additional expenses, delay or prevent the approval of one of our drug candidates, and/or delay or cause us to change our commercialization plans, or we may decide to abandon the development or commercialization of the drug candidate altogether.
We may expend our limited resources to pursue a particular drug candidate or indication and fail to capitalize on drug candidates or indications that may be more profitable or for which there is a greater likelihood of success.
Because we have limited financial and managerial resources, we focus on research programs and drug candidates that we identify for specific indications. As a result, we may forego or delay pursuit of opportunities with other drug candidates or for other indications that later prove to have greater commercial potential. Our resource allocation decisions may cause us to fail to capitalize on viable commercial drugs or profitable market opportunities. Our spending on current and future research and development programs and drug candidates for specific indications may not yield any commercially-viable drugs. If we do not accurately evaluate the commercial potential or target market for a particular drug candidate, we may relinquish valuable rights to that drug candidate through collaboration, licensing or other royalty arrangements in cases in which it would have been more advantageous for us to retain sole development and commercialization rights to such drug candidate.
58
Table of Contents
Even if any of our drug candidates receives marketing approval, such drug may fail to achieve the degree of market acceptance by physicians, patients, third-party payors and others in the medical community necessary for commercial success.
If any of our drug candidates receive marketing approval, it may nonetheless fail to gain sufficient market acceptance by physicians, patients, third-party payors and others in the medical community. For example, current cancer treatments like chemotherapy and radiation therapy are well-established in the medical community, and doctors may continue to rely on these treatments. If our drug candidates do not achieve an adequate level of acceptance, we may not generate significant revenues from sales of drugs and we may not become profitable. The degree of market acceptance of our drug candidates, if approved for commercial sale, will depend on a number of factors, including:
| • | efficacy and potential advantages compared to alternative treatments; |
| • | the ability to offer our drugs for sale at competitive prices; |
| • | convenience and ease of administration compared to alternative treatments; |
| • | the willingness of the target patient population to try new therapies and of physicians to prescribe these therapies; |
| • | the strength of marketing and distribution support; |
| • | sufficient third-party coverage or reimbursement; |
| • | the prevalence and severity of any side effects; |
| • | any restrictions on the use of our drugs together with other medications; and |
| • | inability of certain types of patients to take our drugs. |
If, in the future, we are unable to establish sales and marketing capabilities or enter into agreements with third parties to sell and market our drug candidates, we may not be successful in commercializing our drug candidates if and when they are approved.
We do not have a sales or marketing infrastructure and have no experience in the sale or marketing of pharmaceutical drugs. To date, we have not entered into a strategic collaboration that provides us with access to a collaborator’s resources in selling or marketing drugs. To achieve commercial success for any approved drug for which sales and marketing is not the responsibility of any strategic collaborator that we may have in the future, we must either develop a sales and marketing organization or outsource these functions to other third parties. In the future, we may choose to build a sales and marketing infrastructure to market or co-promote some of our drug candidates if and when they are approved, or enter into collaborations with respect to the sale and marketing of our drug candidates. We currently intend to establish a corporate infrastructure to enable us to market selinexor in North America and Western Europe.
There are risks involved with both establishing our own sales and marketing capabilities and entering into arrangements with third parties to perform these services. For example, recruiting and training a sales force is expensive and time-consuming and could delay any commercial launch of a drug candidate. If the commercial launch of a drug candidate for which we recruit a sales force and establish marketing capabilities is delayed or does not occur for any reason, we would have prematurely or unnecessarily incurred these commercialization expenses. This may be costly, and our investment would be lost if we cannot retain or reposition our sales and marketing personnel.
Factors that may inhibit our efforts to commercialize our drugs on our own include:
| • | our inability to recruit and retain adequate numbers of effective sales and marketing personnel; |
| • | the inability of sales personnel to obtain access to physicians or persuade adequate numbers of physicians to prescribe any future drugs; |
59
Table of Contents
| • | the lack of complementary drugs to be offered by sales personnel, which may put us at a competitive disadvantage relative to companies with more extensive drug lines; |
| • | unforeseen costs and expenses associated with creating an independent sales and marketing organization; and |
| • | inability to obtain sufficient coverage and reimbursement from third-party payors and governmental agencies. |
If we enter into arrangements with third parties to perform sales and marketing services, our revenues from the sale of drug or the profitability of these revenues to us are likely to be lower than if we were to market and sell any drugs that we develop ourselves. In addition, we may not be successful in entering into arrangements with third parties to sell and market our drug candidates or may be unable to do so on terms that are favorable to us. We likely will have little control over such third parties, and any of them may fail to devote the necessary resources and attention to sell and market our drugs effectively. If we do not establish sales and marketing capabilities successfully, either on our own or in collaboration with third parties, we will not be successful in commercializing our drug candidates.
We face substantial competition, which may result in others discovering, developing or commercializing drugs before or more successfully than we do.
The discovery, development and commercialization of new drugs is highly competitive. We face competition with respect to our current drug candidates, and will face competition with respect to any drug candidates that we may seek to discover and develop or commercialize in the future, from major pharmaceutical companies, specialty pharmaceutical companies and biotechnology companies worldwide. There are a number of major pharmaceutical, specialty pharmaceutical and biotechnology companies that currently market and sell drugs or are pursuing the development of drugs for the treatment of cancer and the other disease indications for which we are developing our drug candidates, although we believe that to date, none of these competitive drugs and therapies currently in development are based on scientific approaches that are the same as our approach. Potential competitors also include academic institutions and governmental agencies and public and private research institutions.
We are initially focused on developing our current drug candidates for the treatment of cancer. There are a variety of available therapies marketed for cancer. In many cases, cancer drugs are administered in combination to enhance efficacy. Some of these drugs are branded and subject to patent protection, and others are available on a generic basis. Many of these approved drugs are well-established therapies and are widely accepted by physicians, patients and third-party payors. Insurers and other third-party payors may also encourage the use of generic drugs. We expect that if our drug candidates are approved, they will be priced at a significant premium over competitive generic drugs. This may make it difficult for us to achieve our business strategy of using our drug candidates in combination with existing therapies or replacing existing therapies with our drug candidates.
Our competitors may develop drugs that are more effective, safer, more convenient or less costly than any that we are developing or that would render our drug candidates obsolete or non-competitive. Our competitors may also obtain marketing approval from the FDA or other regulatory authorities for their drugs more rapidly than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we are able to enter the market.
Many of our competitors have significantly greater financial resources and expertise in research and development, manufacturing, preclinical studies, conducting clinical trials, obtaining regulatory approvals and marketing approved drugs than we do. Mergers and acquisitions in the pharmaceutical and biotechnology industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller and other early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These third parties compete with us in
60
Table of Contents
recruiting and retaining qualified scientific and management personnel, establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or that may be necessary for, our programs.
Even if we are able to commercialize any drug candidates, the drugs may become subject to unfavorable pricing regulations, third-party reimbursement practices or healthcare reform initiatives, which would harm our business.
The regulations that govern marketing approvals, pricing and reimbursement for new drugs vary widely from country to country. In the United States, recently enacted legislation may significantly change the approval requirements in ways that could involve additional costs and cause delays in obtaining approvals. Some countries require approval of the sale price of a drug before it can be marketed. In many countries, the pricing review period begins after marketing or drug licensing approval is granted. In some foreign markets, prescription pharmaceutical pricing remains subject to continuing governmental control even after initial approval is granted. As a result, we might obtain marketing approval for a drug in a particular country, but then be subject to price regulations that delay our commercial launch of the drug, possibly for lengthy time periods, and negatively impact the revenues we are able to generate from the sale of the drug in that country. Adverse pricing limitations may hinder our ability to recoup our investment in one or more drug candidates, even if our drug candidates obtain marketing approval.
Our ability to commercialize any drugs successfully also will depend in part on the extent to which reimbursement for these drugs and related treatments will be available from government health administration authorities, private health insurers and other organizations. Government authorities and third-party payors, such as private health insurers and health maintenance organizations, decide which medications they will pay for and establish reimbursement levels. A primary trend in the healthcare industry in the United States and elsewhere is cost containment. Government authorities and third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications. Increasingly, third-party payors are requiring that drug companies provide them with predetermined discounts from list prices and are challenging the prices charged for medical products. We cannot be sure that reimbursement will be available for any drug that we commercialize and, if reimbursement is available, we cannot be sure as to the level of reimbursement. Reimbursement may impact the demand for, or the price of, any drug candidate for which we obtain marketing approval. If reimbursement is not available or is available only to limited levels, we may not be able to successfully commercialize any drug candidate for which we obtain marketing approval.
There may be significant delays in obtaining reimbursement for newly-approved drugs, and coverage may be more limited than the purposes for which the drug is approved by the FDA or similar regulatory authorities outside of the United States. Moreover, eligibility for reimbursement does not imply that any drug will be paid for in all cases or at a rate that covers our costs, including research, development, manufacture, sale and distribution. Interim reimbursement levels for new drugs, if applicable, may also not be sufficient to cover our costs and may not be made permanent. Reimbursement rates may vary according to the use of the drug and the clinical setting in which it is used, may be based on reimbursement levels already set for lower cost drugs and may be incorporated into existing payments for other services. Net prices for drugs may be reduced by mandatory discounts or rebates required by government healthcare programs or private payors and by any future relaxation of laws that presently restrict imports of drugs from countries where they may be sold at lower prices than in the United States. Third-party payors often rely upon Medicare coverage policy and payment limitations in setting their own reimbursement policies. Our inability to promptly obtain coverage and profitable payment rates from both government-funded and private payors for any approved drugs that we develop could have a material adverse effect on our operating results, our ability to raise capital needed to commercialize drugs and our overall financial condition.
61
Table of Contents
Product liability lawsuits against us could cause us to incur substantial liabilities and to limit commercialization of any drugs that we may develop.
We face an inherent risk of product liability exposure related to the testing of our drug candidates in human clinical trials and will face an even greater risk if we commercially sell any drugs that we may develop. If we cannot successfully defend ourselves against claims that our drug candidates or drugs caused injuries, we will incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in:
| • | decreased demand for any drug candidates or drugs that we may develop; |
| • | injury to our reputation and significant negative media attention; |
| • | withdrawal of clinical trial participants; |
| • | significant costs to defend the related litigation; |
| • | substantial monetary awards to trial participants or patients; |
| • | loss of revenue; |
| • | reduced resources of our management to pursue our business strategy; and |
| • | the inability to commercialize any drugs that we may develop. |
We currently hold clinical trial liability insurance coverage, but that coverage may not be adequate to cover any and all liabilities that we may incur. We would need to increase our insurance coverage when we begin the commercialization of our drug candidates, if ever. Insurance coverage is increasingly expensive. We may not be able to maintain insurance coverage at a reasonable cost or in an amount adequate to satisfy any liability that may arise.
Verdinexor (KPT-335) is our clinical drug candidate for the treatment of pet dogs with newly-diagnosed and first time relapse lymphomas. If the results of our clinical trials of verdinexor are not viewed positively or verdinexor is not approved by the FDA, this may raise safety and efficacy concerns for selinexor, as the anti-cancer activity and adverse event profile of verdinexor in dogs with lymphomas provided support for our decision to move selinexor into Phase 1 clinical trials.
As part of the drug discovery and development process, we have used spontaneously occurring pet dog cancers as a surrogate model for human malignancies. Dog lymphomas respond to chemotherapy in a manner similar to their human counterparts (human non-Hodgkin’s lymphomas) and display a comparable genetic profile. The anti-cancer activity of our drug candidate verdinexor (KPT-335) in a Phase 1 clinical trial in dogs with certain lymphomas provided support for our decision to move selinexor, our closely-related human drug candidate, into Phase 1 clinical trials. We conducted a Phase 2b clinical trial of verdinexor in dogs with newly-diagnosed or first time relapse lymphomas. We have received a Minor Use / Minor Species, or MUMS, designation from the Center for Veterinary Medicine of the FDA for the treatment of newly-diagnosed or after first relapse lymphomas in dogs with verdinexor. Our Phase 2b clinical trial was intended to support regulatory approval under the MUMS designation. We submitted and the FDA accepted the safety and effectiveness sections of a NADA for verdinexor. If verdinexor fails to shows adequate safety or efficacy or is not otherwise viewed positively or if verdinexor is not otherwise approved by the FDA for the treatment of lymphomas in dogs, this may raise questions regarding selinexor because we have used dog cancers as a surrogate model for human malignancies. In such an event, verdinexor’s clinical trial results may cause the FDA or non-U.S. regulatory authorities to require more information, including additional preclinical or clinical data to support approval of selinexor. If the results of the Phase 2b clinical trial of verdinexor fail to demonstrate safety and efficacy to the satisfaction of the FDA or are not otherwise viewed positively, we may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of verdinexor. In such an event, we also may not be able to realize our potential to generate revenue from the commercialization of verdinexor, either on our own or with a collaborator.
62
Table of Contents
The business that we conduct outside the United States may be adversely affected by international risk and uncertainties.
Although our operations are based in the United States, we conduct business outside the United States and expect to continue to do so in the future. For instance, many of the sites at which our clinical trials are being conducted are located outside the United States. In addition, we plan to seek approvals to sell our products in foreign countries. Any business that we conduct outside the United States will be subject to additional risks that may materially adversely affect our ability to conduct business in international markets, including:
| • | potentially reduced protection for intellectual property rights; |
| • | the potential for so-called parallel importing, which is what happens when a local seller, faced with high or higher local prices, opts to import goods from a foreign market (with low or lower prices) rather than buying them locally; |
| • | unexpected changes in tariffs, trade barriers and regulatory requirements; |
| • | economic weakness, including inflation, or political instability in particular foreign economies and markets; |
| • | workforce uncertainty in countries where labor unrest is more common than in the United States; |
| • | production shortages resulting from any events affecting a product candidate and/or finished drug product supply or manufacturing capabilities abroad; |
| • | business interruptions resulting from geo-political actions, including war and terrorism, or natural disasters, including earthquakes, hurricanes, typhoons, floods and fires; and |
| • | failure to comply with Office of Foreign Asset Control rules and regulations and the Foreign Corrupt Practices Act, or FCPA. |
Risks Related to Our Financial Position and Need for Additional Capital
We have incurred significant losses since inception. We expect to incur losses for the foreseeable future and may never achieve or maintain profitability.
Since inception, we have incurred significant operating losses. Our net losses were $118.2 million and $75.8 million for the years ended December 31, 2015 and December 31, 2014, respectively. As of December 31, 2015 and December 31, 2014, we had accumulated deficits of $256.5 million and $138.3 million, respectively. We have not generated any revenue to date from sales of any drugs and have financed our operations principally through sales of equity in private placements, our initial public offering, or IPO, and two follow-on offerings of our common stock, as well as an “at-the-market” offering, also known as a controlled equity offering, that we commenced in December 2015 and pursuant to which we may sell additional shares of our common stock. We have devoted substantially all of our efforts to research and development. Our lead drug candidate, oral selinexor (KPT-330), as well as verdinexor (KPT-335) and KPT-8602, are in clinical development and our other drug candidates for the treatment of human disease are expected to begin clinical development in 2016 or are in preclinical development. As a result, we expect that it will be several years, if ever, before we have a drug candidate ready for commercialization for the treatment of human disease. We expect to continue to incur significant expenses and increasing operating losses for the foreseeable future. The net losses we incur may fluctuate significantly from quarter to quarter. We anticipate that our expenses will increase substantially if and as we:
| • | continue our research and preclinical and clinical development of our drug candidates; |
| • | identify additional drug candidates; |
| • | initiate additional clinical trials for our drug candidates; |
| • | seek marketing approvals for any of our drug candidates that successfully complete clinical trials; |
| • | ultimately establish sales, marketing, manufacturing and distribution infrastructure to commercialize any drugs for which we may obtain marketing approval; |
63
Table of Contents
| • | maintain, expand and protect our intellectual property portfolio; |
| • | hire additional clinical, quality control and scientific personnel; |
| • | acquire or in-license other drugs and technologies; and |
| • | add operational, financial and management information systems and personnel, including personnel to support our drug development, any future commercialization efforts and our operations as a public company. |
To become and remain profitable, we must develop and eventually commercialize a drug or drugs with significant market potential, either on our own or with a collaborator. This will require us to be successful in a range of challenging activities, including completing preclinical studies and clinical trials of our drug candidates, obtaining marketing approval for these drug candidates, manufacturing, marketing and selling those drugs for which we may obtain marketing approval and establishing and managing any collaborations for the development, marketing and/or commercialization of our drug candidates. We may never succeed in these activities and, even if we do, may never generate revenues that are significant or large enough to achieve profitability. If we do achieve profitability, we may not be able to sustain or increase profitability on a quarterly or annual basis. Our failure to become and remain profitable would decrease the value of the company and could impair our ability to raise capital, maintain our research and development efforts, expand our business and/or continue our operations. A decline in the value of our company could also cause our stockholders to lose all or part of their investment.
Our short operating history may make it difficult for stockholders to evaluate the success of our business to date and to assess our future viability.
We are an early-stage company. We were incorporated in 2008 and commenced operations in 2009. Our operations to date have been limited to organizing and staffing our company, business planning, raising capital, developing our platform, identifying potential drug candidates and conducting preclinical studies and early-stage clinical trials of our drug candidates. Our lead drug candidate is currently in multiple Phase 1 and Phase 2 clinical trials and all of our other drug candidates for the treatment of human disease are in early clinical development or preclinical development. We have not yet demonstrated our ability to successfully complete any late-stage clinical trials in humans, including large-scale clinical trials, obtain marketing approvals, manufacture a commercial scale drug, or arrange for a third party to do so on our behalf, or conduct sales and marketing activities necessary for successful drug commercialization. Typically, it takes about six to ten years to develop one new drug from the time it is in Phase 1 clinical trials to when it is available for treating patients. Consequently, any predictions stockholders make about our future success or viability may not be as accurate as they could be if we had a longer operating history.
In addition, as a business with a short operating history, we may encounter unforeseen expenses, difficulties, complications, delays and other known and unknown factors. We will need to transition from a company with a research focus to a company capable of supporting commercial activities. We may not be successful in such a transition.
As we continue to build our business, we expect our financial condition and operating results may fluctuate significantly from quarter to quarter and year to year due to a variety of factors, many of which are beyond our control. Accordingly, stockholders should not rely upon the results of any particular quarterly or annual periods as indications of future operating performance.
We will need substantial additional funding. If we are unable to raise capital when needed, we would be forced to delay, reduce or eliminate our research and drug development programs or commercialization efforts.
We expect our expenses to increase in connection with our ongoing activities, particularly as we continue the clinical trials of, and seek marketing approval for, selinexor and our other drug candidates. In addition, if we
64
Table of Contents
obtain marketing approval for any of our drug candidates, we expect to incur significant commercialization expenses related to drug sales, marketing, manufacturing and distribution to the extent that such sales, marketing, manufacturing and distribution are not the responsibility of any collaborator that we may have at such time for any such drug. Furthermore, we will continue to incur additional costs associated with operating as a public company. Accordingly, we will need to obtain substantial additional funding in connection with our continuing operations. If we are unable to raise capital when needed or on attractive terms, we would be forced to delay, reduce or eliminate our research and drug development programs or commercialization efforts.
We expect that our existing cash, cash equivalents, restricted cash and investments will enable us to fund our operating expenses and capital expenditure requirements into the middle of 2018. Our future capital requirements will depend on many factors, including:
| • | the progress and results of our current and planned clinical trials of selinexor; |
| • | the scope, progress, results and costs of drug discovery, preclinical development, laboratory testing and clinical trials for our other drug candidates; |
| • | the costs, timing and outcome of regulatory review of our drug candidates; |
| • | our ability to establish and maintain collaborations on favorable terms, if at all; |
| • | the success of any collaborations that we may enter into with third parties; |
| • | the extent to which we acquire or in-license other drugs and technologies; |
| • | the costs of future commercialization activities, including drug sales, marketing, manufacturing and distribution, for any of our drug candidates for which we receive marketing approval, to the extent that such sales, marketing, manufacturing and distribution are not the responsibility of any collaborator that we may have at such time; |
| • | the amount of revenue, if any, received from commercial sales of our drug candidates, should any of our drug candidates receive marketing approval; and |
| • | the costs of preparing, filing and prosecuting patent applications, maintaining and enforcing our intellectual property rights and defending intellectual property-related claims. |
Identifying potential drug candidates and conducting preclinical studies and clinical trials is a time-consuming, expensive and uncertain process that takes years to complete, and we may never generate the necessary data or results required to obtain marketing approval and achieve drug sales. In addition, our drug candidates, if approved, may not achieve commercial success. Our commercial revenues, if any, will be derived from sales of drugs that we do not expect to be commercially available for many years, if at all. Accordingly, we will need to continue to rely on additional financing to achieve our business objectives. Adequate additional financing may not be available to us on acceptable terms, or at all. In addition, we may seek additional capital due to favorable market conditions or strategic considerations, even if we believe we have sufficient funds for our current or future operating plans.
Raising additional capital may cause dilution to our stockholders, restrict our operations or require us to relinquish rights to our drug candidates.
Until such time, if ever, as we can generate substantial revenues from the sale of drugs, we expect to finance our cash needs through a combination of equity offerings, debt financings, collaborations, strategic alliances and/or licensing arrangements. We do not have any committed external source of funds. To the extent that we raise additional capital through the sale of equity or convertible debt securities, the ownership interests of stockholders will be diluted, and the terms of these securities may include liquidation or other preferences that adversely affect the rights of common stockholders. Debt financing, if available, may involve agreements that include covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, making capital expenditures or declaring dividends.
65
Table of Contents
If we raise funds through collaborations, strategic alliances or licensing arrangements with third parties, we may have to relinquish valuable rights to our future revenue streams, research programs or drug candidates or to grant licenses on terms that may not be favorable to us. If we are unable to raise additional funds through equity or debt financings when needed, we may be required to delay, limit, reduce or terminate our research and drug development or commercialization efforts or grant rights to develop and market drug candidates that we would otherwise prefer to develop and market ourselves.
Unstable market and economic conditions may have serious adverse consequences on our business, financial condition and stock price.
Global credit and financial markets have experienced extreme disruptions over some of the past several years, including in recent months. Such disruptions have resulted, and could in the future result, in diminished liquidity and credit availability, declines in consumer confidence, declines in economic growth, increases in unemployment rates and uncertainty about economic stability. There can be no assurance that any deterioration in credit and financial markets and confidence in economic conditions will not occur. Our general business strategy may be compromised by economic downturns, a volatile business environment and unpredictable and unstable market conditions. If the equity and credit markets deteriorate, it may make any necessary equity or debt financing more difficult to secure, more costly or more dilutive. Failure to secure any necessary financing in a timely manner and on favorable terms could harm our growth strategy, financial performance and stock price and could require us to delay or abandon plans with respect to our business, including clinical development plans. In addition, there is a risk that one or more of our current service providers, manufacturers or other third parties with which we conduct business may not survive difficult economic times, which could directly affect our ability to attain our operating goals on schedule and on budget.
Risks Related to Our Dependence on Third Parties
We expect to depend on third parties for certain aspects of the development, marketing and/or commercialization of our drug candidates. If those collaborations are not successful, we may not be able to capitalize on the market potential of these drug candidates.
We intend to seek third-party collaborators for certain aspects of the development, marketing and/or commercialization of our drug candidates. For example, while we currently plan to develop and seek approval of selinexor in North America and Western Europe with respect to the potential approval of selinexor without a collaborator, we anticipate that we will seek to enter into a collaboration for marketing and commercialization of selinexor at the appropriate time in the future for other geographies. In addition, we intend to seek one or more collaborators to aid in the further development, marketing and/or commercialization of our other SINE compounds for inflammatory, autoimmune and/or neurological conditions and viral indications. Our likely collaborators for any collaboration arrangements include large and mid-size pharmaceutical companies, regional and national pharmaceutical companies and biotechnology companies. If we do enter into any such arrangements with any third parties, we will likely have limited control over the amount and timing of resources that our collaborators dedicate to the development, marketing and/or commercialization of our drug candidates. Our ability to generate revenues from these arrangements will depend on our collaborators’ abilities to successfully perform the functions assigned to them in these arrangements.
Collaborations involving our drug candidates pose the following risks to us:
| • | collaborators have significant discretion in determining the efforts and resources that they will apply to these collaborations; |
| • | collaborators may not pursue development, marketing and/or commercialization of our drug candidates or may elect not to continue or renew development, marketing or commercialization programs based on clinical trial results, changes in the collaborator’s strategic focus or available funding or external factors such as an acquisition that diverts resources or creates competing priorities; |
66
Table of Contents
| • | collaborators may delay clinical trials, provide insufficient funding for a clinical trial program, stop a clinical trial or abandon a drug candidate, repeat or conduct new clinical trials or require a new formulation of a drug candidate for clinical testing; |
| • | collaborators could independently develop, or develop with third parties, drugs that compete directly or indirectly with our drugs or drug candidates if the collaborators believe that competitive drugs are more likely to be successfully developed or can be commercialized under terms that are more economically attractive than ours; |
| • | a collaborator with marketing and distribution rights to one or more drugs may not commit sufficient resources to the marketing and distribution of such drug or drugs; |
| • | collaborators may not properly maintain or defend our intellectual property rights or may use our proprietary information in such a way as to invite litigation that could jeopardize or invalidate our proprietary information or expose us to potential litigation; |
| • | collaborators may infringe the intellectual property rights of third parties, which may expose us to litigation and potential liability; |
| • | disputes may arise between the collaborators and us that result in the delay or termination of the research, development or commercialization of our drugs or drug candidates or that result in costly litigation or arbitration that diverts management’s attention and resources of the company; |
| • | we may lose certain valuable rights under circumstances identified in any collaboration arrangement that we enter into, such as if we undergo a change of control; |
| • | collaborations may be terminated and, if terminated, may result in a need for additional capital to pursue further development, marketing and/or commercialization of the applicable drug candidates; |
| • | collaborators may learn about our discoveries and use this knowledge to compete with us in the future; and |
| • | the number and type of our collaborations could adversely affect our attractiveness to future collaborators or acquirers. |
Collaboration agreements may not lead to development or commercialization of drug candidates in the most efficient manner, or at all.
If we are not able to establish collaborations as we currently plan, we may have to alter our development and commercialization plans.
Our drug development programs and the potential commercialization of our drug candidates will require substantial additional cash to fund expenses. As noted above, we expect to collaborate with pharmaceutical and biotechnology companies for the development and/or commercialization of our drug candidates.
We face significant competition in seeking appropriate collaborators. Whether we reach a definitive agreement for a collaboration will depend, among other things, upon our assessment of the collaborator’s resources and expertise, the terms and conditions of the proposed collaboration and the proposed collaborator’s evaluation of a number of factors. Those factors may include the design or results of clinical trials, the likelihood of approval by the FDA or similar regulatory authorities outside of the United States, the potential market for the subject drug candidate, the costs and complexities of manufacturing and delivering such drug candidate to patients, the potential of competing drugs, the existence of uncertainty with respect to our ownership of intellectual property, which can exist if there is a challenge to such ownership without regard to the merits of the challenge, and industry and market conditions generally. The collaborator may also consider alternative drug candidates or technologies for similar indications that may be available to collaborate on and whether such a collaboration could be more attractive than the one with us for our drug candidate.
67
Table of Contents
We may also be restricted under then-existing collaboration agreements from entering into future agreements on certain terms with potential collaborators.
Collaborations are complex and time-consuming to negotiate and document. In addition, there have been a significant number of recent business combinations among large pharmaceutical companies that have resulted in a reduced number of potential future collaborators.
We may not be able to negotiate collaborations on a timely basis, on acceptable terms, or at all. If we are unable to do so, we may have to curtail the development of such drug candidate, reduce or delay its development program or one or more of our other development programs, delay its potential commercialization or reduce the scope of any sales or marketing activities, or increase our expenditures and undertake development or commercialization activities at our own expense. If we elect to increase our expenditures to fund development or commercialization activities on our own, we may need to obtain additional capital, which may not be available to us on acceptable terms, or at all. If we do not have sufficient funds, we may not be able to further develop our drug candidates or bring them to market and generate revenue from sales of drugs.
We rely on third parties to conduct our clinical trials and some aspects of our research and preclinical studies, and those third parties may not perform satisfactorily, including failing to meet deadlines for the completion of such trials, research or testing.
We rely on third parties, such as contract research organizations, clinical data management organizations, medical institutions and clinical investigators, to conduct our clinical trials. We currently rely and expect to continue to rely on third parties to conduct some aspects of our research and preclinical studies. Any of these third parties may terminate their engagements with us at any time. If we need to enter into alternative arrangements, it would delay our drug development activities.
Our reliance on these third parties for research and development activities will reduce our control over these activities but will not relieve us of our responsibilities. For example, we will remain responsible for ensuring that each of our clinical trials is conducted in accordance with the general investigational plan and protocols for the trial. Moreover, the FDA requires us to comply with standards, commonly referred to as Good Clinical Practices, for conducting, recording and reporting the results of clinical trials to assure that data and reported results are credible and accurate and that the rights, integrity and confidentiality of trial participants are protected. The European Medicines Agency also requires us to comply with comparable standards. We also are required to register ongoing clinical trials and post the results of completed clinical trials on a government-sponsored database, ClinicalTrials.gov, within certain timeframes. Failure to do so can result in fines, adverse publicity and civil and criminal sanctions.
Furthermore, these third parties may also have relationships with other entities, some of which may be our competitors. If these third parties do not successfully carry out their contractual duties, meet expected deadlines or conduct our clinical trials in accordance with regulatory requirements or our stated protocols, we will not be able to obtain, or may be delayed in obtaining, marketing approvals for our drug candidates and will not be able to, or may be delayed in our efforts to, successfully commercialize our drug candidates.
We also expect to rely on other third parties to store and distribute drug supplies for our clinical trials. Any performance failure on the part of such third parties could delay clinical development or marketing approval of our drug candidates or commercialization of our drugs, producing additional losses and depriving us of potential revenue from sales of drugs.
68
Table of Contents
We rely on third parties to conduct investigator-sponsored clinical trials of selinexor and our other drug candidates. Any failure by a third party to meet its obligations with respect to the clinical development of our drug candidates may delay or impair our ability to obtain regulatory approval for selinexor and our other drug candidates.
We rely on academic and private non-academic institutions to conduct and sponsor clinical trials relating to selinexor and our other drug candidates. We do not control the design or conduct of the investigator-sponsored trials, and it is possible that the FDA or non-U.S. regulatory authorities will not view these investigator-sponsored trials as providing adequate support for future clinical trials, whether controlled by us or third parties, for any one or more reasons, including elements of the design or execution of the trials or safety concerns or other trial results.
Such arrangements will provide us certain information rights with respect to the investigator-sponsored trials, including access to and the ability to use and reference the data, including for our own regulatory filings, resulting from the investigator-sponsored trials. However, we do not have control over the timing and reporting of the data from investigator-sponsored trials, nor do we own the data from the investigator-sponsored trials. If we are unable to confirm or replicate the results from the investigator-sponsored trials or if negative results are obtained, we would likely be further delayed or prevented from advancing further clinical development of our drug candidates. Further, if investigators or institutions breach their obligations with respect to the clinical development of our drug candidates, or if the data proves to be inadequate compared to the first-hand knowledge, we might have gained had the investigator-sponsored trials been sponsored and conducted by us, then our ability to design and conduct any future clinical trials ourselves may be adversely affected.
Additionally, the FDA or non-U.S. regulatory authorities may disagree with the sufficiency of our right of reference to the preclinical, manufacturing or clinical data generated by these investigator-sponsored trials, or our interpretation of preclinical, manufacturing or clinical data from these investigator-sponsored trials. If so, the FDA or other non-U.S. regulatory authorities may require us to obtain and submit additional preclinical, manufacturing, or clinical data before we may initiate our planned trials and/or may not accept such additional data as adequate to initiate our planned trials.
We contract with third parties for the manufacture of our drug candidates for preclinical studies and clinical trials and expect to continue to do so for clinical trials and ultimately for commercialization. This reliance on third parties increases the risk that we will not have sufficient quantities of our drug candidates or drugs or such quantities at an acceptable cost, which could delay, prevent or impair our development or commercialization efforts.
We do not have any manufacturing facilities or personnel. We currently rely, and expect to continue to rely, on third-party manufacturers for the manufacture of our drug candidates for preclinical studies and clinical trials under the guidance of members of our organization. We have engaged third-party manufacturers for drug substance and drug product (fill-and-finish) services. We do not have a long term supply agreement with any of these third-party manufacturers, and we purchase our required drug supplies on a purchase order basis.
We expect to rely on third-party manufacturers or third-party collaborators for the manufacture of our drug candidates for clinical trials and ultimately for commercial supply of any of these drug candidates for which we or any of our future collaborators obtain marketing approval. We may be unable to establish any agreements with third-party manufacturers or to do so on acceptable terms. Even if we are able to establish agreements with third-party manufacturers, reliance on third-party manufacturers entails additional risks, including:
| • | reliance on the third party for regulatory compliance and quality assurance; |
| • | the possible breach of the manufacturing agreement by the third party; |
| • | the possible failure of the third party to manufacture our drug candidate according to our specifications; |
| • | the possible failure of the third party to manufacture our drug candidate according to our schedule, or at all; |
69
Table of Contents
| • | the possible misappropriation or disclosure by the third party or others of our proprietary information, including our trade secrets and know-how; and |
| • | the possible termination or nonrenewal of the agreement by the third party at a time that is costly or inconvenient for us. |
Third-party manufacturers may not be able to comply with cGMP regulations or similar regulatory requirements outside of the United States. Our failure, or the failure of our third-party manufacturers, to comply with applicable regulations could result in sanctions being imposed on us, including fines, injunctions, civil penalties, delays, suspension or withdrawal of approvals, license revocation, seizures or recalls of drug candidates or drugs, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect supplies of our drugs and harm our business and results of operations.
Any drugs that we may develop may compete with other drug candidates and drugs for access to manufacturing facilities. There are a limited number of manufacturers that operate under cGMP regulations and that might be capable of manufacturing for us.
Any performance failure on the part of our existing or future manufacturers could delay clinical development or marketing approval. If our current contract manufacturers cannot perform as agreed, we may be required to replace those manufacturers. Although we believe that there are several potential alternative manufacturers who could manufacture our drug candidates, we may incur added costs and delays in identifying and qualifying any such replacement.
Our current and anticipated future dependence upon others for the manufacture of our drug candidates or drugs may adversely affect our future profit margins and our ability to commercialize any drugs that receive marketing approval on a timely and competitive basis.
Risks Related to Our Intellectual Property
If we are unable to obtain and maintain patent protection for our drug candidates and other discoveries, or if the scope of the patent protection obtained is not sufficiently broad, our competitors could develop and commercialize drugs and other discoveries similar or identical to ours, and our ability to successfully commercialize our drug candidates and other discoveries may be adversely affected.
Our success depends in large part on our ability to obtain and maintain patent protection in the United States and other countries with respect to our proprietary drug candidates and other discoveries. We seek to protect our proprietary position by filing patent applications in the United States and abroad related to our novel drug candidates and other discoveries that are important to our business. To date, ten patents have issued that relate to XPO1 inhibitors, including composition of matter patents for selinexor, verdinexor and KPT-350 in the United States, and their use in targeted therapeutics. We cannot be certain that any other patents will issue with claims that cover any of our key drug candidates or other discoveries or drug candidates.
The patent prosecution process is expensive and time-consuming, and we may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner. It is also possible that we will fail to identify patentable aspects of our research and development output before it is too late to obtain patent protection.
The patent position of biotechnology and pharmaceutical companies generally is highly uncertain, involves complex legal and factual questions and has in recent years been the subject of much litigation. As a result, the issuance, scope, validity, enforceability and commercial value of our patent rights are highly uncertain. Our pending and future patent applications may not result in patents being issued which protect our drug candidates or other discoveries, or which effectively prevent others from commercializing competitive drugs and discoveries. Changes in either the patent laws or interpretation of the patent laws in the United States and other countries may diminish the value of our patents or narrow the scope of our patent protection.
70
Table of Contents
The laws of foreign countries may not protect our rights to the same extent as the laws of the United States. For example, in some foreign jurisdictions, our ability to secure patents based on our filings in the United States may depend, in part, on our ability to timely obtain assignment of rights to the invention from the employees and consultants who invented the technology. Publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in the United States and other jurisdictions are typically not published until 18 months after filing, or in some cases not at all. Therefore, we cannot be certain that we were the first to make the inventions claimed in our patent or pending patent applications, or that we were the first to file for patent protection of such inventions.
Assuming the other requirements for patentability are met, prior to March 2013, in the United States, the first to invent the claimed invention was entitled to the patent, while outside of the United States, the first to file a patent application is entitled to the patent. In March 2013, the United States transitioned to a first-inventor-to-file system in which, assuming the other requirements for patentability are met, the first inventor to file a patent application is entitled to the patent. We may be subject to a third-party preissuance submission of prior art to the U.S. Patent and Trademark Office, or become involved in opposition, derivation, revocation, reexamination, or post-grant or inter partes review or interference proceedings challenging our patent rights or the patent rights of others. An adverse determination in any such submission, proceeding or litigation could reduce the scope of, or invalidate, our patent rights, allow third parties to commercialize our discoveries or drugs and compete directly with us, without payment to us, or result in our inability to manufacture or commercialize drugs without infringing third-party patent rights.
Even if our patent applications issue as patents, they may not issue in a form that will provide us with any meaningful protection, prevent competitors from competing with us or otherwise provide us with any competitive advantage. Our competitors may be able to circumvent our patents by developing similar or alternative discoveries or drugs in a non-infringing manner.
The issuance of a patent is not conclusive as to its inventorship, scope, validity or enforceability, and our patents may be challenged in the courts or patent offices in the United States and abroad. Such challenges may result in loss of exclusivity or in patent claims being narrowed, invalidated or held unenforceable, which could limit our ability to stop others from using or commercializing similar or identical discoveries and drugs, or limit the duration of the patent protection of our discoveries and drug candidates. Given the amount of time required for the development, testing and regulatory review of new drug candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. As a result, our patent portfolio may not provide us with sufficient rights to exclude others from commercializing drugs similar or identical to ours.
We may become involved in lawsuits to protect or enforce our patents and other intellectual property rights, which could be expensive, time-consuming and unsuccessful.
Competitors or commercial supply companies or others may infringe our patents and other intellectual property rights. For example, we are aware of a third party selling a version of our lead product candidate for research purposes, which may infringe our intellectual property rights. To counter such infringement, we may advise such companies of our intellectual property rights, including, in some cases, intellectual property rights that provide protection for our lead product candidates, and demand that they stop infringing those rights. Such demand may provide such companies the opportunity to challenge the validity of certain of our intellectual property rights, or the opportunity to seek a finding that their activities do not infringe our intellectual property rights. We may also be required to file infringement actions, which can be expensive and time-consuming. In an infringement proceeding, a defendant may assert and a court may agree with a defendant that a patent of ours is invalid or unenforceable, or may refuse to stop the other party from using the intellectual property at issue. An adverse result in any litigation could put one or more of our patents at risk of being invalidated or interpreted narrowly. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation.
71
Table of Contents
Third parties may initiate legal proceedings alleging that we are infringing their intellectual property rights, the outcome of which would be uncertain and could have a material adverse effect on the success of our business.
Our commercial success depends upon our ability and the ability of any future collaborators that we may have to develop, manufacture, market and sell our drug candidates and use our proprietary technologies without infringing the proprietary rights of third parties. We may become party to, or threatened with, future adversarial proceedings or litigation regarding intellectual property rights with respect to our drug candidates and technology, including interference proceedings before the U.S. Patent and Trademark Office. Third parties may assert infringement claims against us based on existing patents or patents that may be granted in the future. No litigation asserting such infringement claims is currently pending against us, and we have not been found by a court of competent jurisdiction to have infringed a third party’s intellectual property rights; however, if we are found to infringe a third party’s intellectual property rights, we could be required to obtain a license from such third party to continue developing and marketing our drug candidates and using our technology. However, we may not be able to obtain any required license on commercially reasonable terms, or at all. Even if we were able to obtain a license, it could be non-exclusive, thereby giving our competitors access to the same intellectual property licensed to us. We could be forced, including by court order, to cease commercializing the infringing intellectual property or drug or to cease using the infringing technology. In addition, we could be found liable for monetary damages. A finding of infringement could prevent us from commercializing our drug candidates or force us to cease some of our business operations, which could materially harm our business. Claims that we have misappropriated the confidential information or trade secrets of third parties could have a similar negative impact on our business.
We may be subject to claims that our employees have wrongfully used or disclosed alleged trade secrets of their former employers.
Many of our employees were previously employed at universities or other biotechnology or pharmaceutical companies, including our competitors or potential competitors. Although we try to ensure that our employees do not use the proprietary information or know-how of others in their work for us, we may be subject to claims that we or these employees have used or disclosed intellectual property, including trade secrets or other proprietary information, of any such employee’s former employer. Although we have no knowledge of any such claims being alleged to date, if such claims were to arise, litigation may be necessary to defend against any such claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management.
Intellectual property litigation could cause us to spend substantial resources and distract our personnel from their normal responsibilities.
Even if resolved in our favor, litigation or other legal proceedings relating to intellectual property claims may cause us to incur significant expenses, and could distract our technical and management personnel from their normal responsibilities. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments and if securities analysts or investors perceive these results to be negative, it could have a material adverse effect on the price of our common stock. Such litigation or proceedings could substantially increase our operating losses and reduce the resources available for development activities or any future sales, marketing or distribution activities. We may not have sufficient financial or other resources to adequately conduct such litigation or proceedings. Some of our competitors may be able to sustain the costs of such litigation or proceedings more effectively than we can because of their greater financial resources. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could have a material adverse effect on our ability to compete in the marketplace.
72
Table of Contents
Obtaining and maintaining our patent protection depends on compliance with various procedural, documentary, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
Periodic maintenance fees, renewal fees, annuity fees and various other governmental fees on patents and/or applications will be due to the United States Patent and Trademark Office, or USPTO, and various foreign patent offices at various points over the lifetime of the patents and/or applications. We have systems in place to remind us to pay these fees, and we rely on our outside counsel to pay these fees when due. Additionally, the USPTO and various foreign patent offices require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. We employ reputable law firms and other professionals to help us comply with such provisions, and in many cases, an inadvertent lapse can be cured by payment of a late fee or by other means in accordance with rules applicable to the particular jurisdiction. However, there are situations in which non-compliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. If such an event were to occur, it could have a material adverse effect on our business.
If we do not successfully extend the term of patents covering our drug candidates under the Hatch-Waxman Amendments and similar foreign legislation, our business may be materially harmed.
Depending upon the timing, duration and conditions of FDA marketing approval, if any, of our drug candidates, one or more of our U.S. patents may be eligible for patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984, referred to as the Hatch-Waxman Amendments. The Hatch-Waxman Amendments permit a patent term extension of up to five years for one patent covering an approved product as compensation for effective patent term lost during product development and the FDA regulatory review process. However, we may not receive an extension if we fail to apply within applicable deadlines, fail to apply prior to expiration of relevant patents or otherwise fail to satisfy applicable requirements. Moreover, the length of the extension could be less than we request. The total patent term, including the extension period, may not exceed 14 years following FDA approval. Accordingly, the length of the extension, or the ability to even obtain an extension, depends on many factors.
In the United States, only a single patent can be extended for each qualifying FDA approval, and any patent can be extended only once and only for a single product. Laws governing analogous patent term extensions in foreign jurisdictions vary widely, as do laws governing the ability to obtain multiple patents from a single patent family. Because both selinexor and verdinexor are protected by a single family of patents and applications, we may not be able to secure patent term extensions for both of these drug candidates in all jurisdictions where these drug candidates are approved, if ever.
If we are unable to obtain a patent term extension for a drug candidate or the term of any such extension is less than we request, the period during which we can enforce our patent rights for that drug candidate, if any, in that jurisdiction will be shortened and our competitors may obtain approval to market competing products sooner. As a result, our revenue could be materially reduced.
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position would be harmed.
In addition to seeking patents for our drug candidates and other discoveries, we also rely on trade secrets, including unpatented know-how, technology and other proprietary information, to maintain our competitive position. We seek to protect these trade secrets, in part, by entering into non-disclosure and confidentiality agreements with parties who have access to them, such as our employees, outside scientific collaborators, contract research organizations, contract manufacturers, consultants, advisors and other third parties. We also enter into confidentiality and invention or patent assignment agreements with our employees and consultants. Despite these efforts, any of these parties may breach the agreements and disclose our proprietary information,
73
Table of Contents
including our trade secrets, and we may not be able to obtain adequate remedies for such breaches. To the extent that we are unable to timely enter into confidentiality and invention or patent assignment agreements with our employees and consultants, our ability to protect our business through trade secrets and patents may be harmed. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, some courts inside and outside of the United States are less willing or unwilling to protect trade secrets. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them from using that technology or information to compete with us. If any of our trade secrets were to be disclosed to or independently developed by a competitor, our competitive position would be harmed.
Not all of our trademarks are registered. Failure to secure those registrations could adversely affect our business.
Three of our trademarks are registered in the United States. We also have seven pending intent to use applications that we filed in 2014 and 2015. Five of those applications have been allowed, meaning that we can perfect our registrations when we have commenced use in commerce, and two are under examination. Outside the United States, we have five registrations in the European Union, and we filed two applications each in fourteen other jurisdictions. Some of those have proceeded to grant. If we do not secure registrations for our trademarks, we may encounter more difficulty in enforcing them against third parties than we otherwise would, which could adversely affect our business. During trademark registration proceedings in the United States and foreign jurisdictions, we may receive rejections. We are given an opportunity to respond to those rejections, but we may not be able to overcome such rejections. In addition, in the USPTO and in comparable agencies in many foreign jurisdictions, third parties are given an opportunity to oppose pending trademark applications and to seek to cancel registered trademarks. Opposition or cancellation proceedings may be filed against our trademarks, and our trademarks may not survive such proceedings.
In addition, any proprietary name we propose to use with our key drug candidates in the United States must be approved by the FDA, regardless of whether we have registered it, or applied to register it, as a trademark. The FDA typically conducts a review of proposed drug names, including an evaluation of potential for confusion with other drug names. If the FDA objects to any of our proposed proprietary drug names for any of our drug candidates, if approved, we may be required to expend significant additional resources in an effort to identify a suitable proprietary drug name that would qualify under applicable trademark laws, not infringe the existing rights of third parties and be acceptable to the FDA.
Risks Related to Regulatory Approval and Marketing of Our Product Candidates Other Legal Compliance Matters
We may not be able to obtain orphan drug exclusivity for our product candidates.
Regulatory authorities in some jurisdictions, including the United States and Europe, may designate drugs and biologics for relatively small patient populations as orphan drugs. Under the Orphan Drug Act, the FDA may designate a product as an orphan drug if it is a drug or biologic intended to treat a rare disease or condition, which is generally defined as a patient population of fewer than 200,000 individuals annually in the United States.
Generally, if a product with an orphan drug designation subsequently receives the first marketing approval for the indication for which it has such designation, the product is entitled to a period of marketing exclusivity, which precludes the EMA or the FDA from approving another marketing application for the same product for that time period. The applicable period is seven years in the United States and ten years in Europe. The European exclusivity period can be reduced to six years if a product no longer meets the criteria for orphan drug designation or if the product is sufficiently profitable so that market exclusivity is no longer justified. Orphan drug exclusivity may be lost if the FDA or EMA determines that the request for designation was materially
74
Table of Contents
defective or if the manufacturer is unable to assure sufficient quantity of the product to meet the needs of patients with the rare disease or condition.
Even if we obtain orphan drug exclusivity from the FDA for a product, as we have for selinexor in acute myeloid leukemia (AML), diffuse large B-cell lymphoma (DLBCL), including Richter’s transformation, and multiple myeloma, that exclusivity may not effectively protect the product from competition because different products can be approved for the same condition. Even after an orphan drug is approved, the FDA can subsequently approve the same product for the same condition if the FDA concludes that the later product is clinically superior in that it is shown to be safer, more effective or makes a major contribution to patient care.
A fast track designation, grant of priority review status or breakthrough therapy status by the FDA is not assured and, in any event, may not actually lead to a faster development or regulatory review or approval process and, moreover, would not assure FDA approval of our product candidates.
We may be eligible for fast track designation, priority review or breakthrough therapy status for product candidates that we develop. If a product is intended for the treatment of a serious or life-threatening disease or condition and the product demonstrates the potential to address unmet medical needs for this disease or condition, the product sponsor may apply for FDA fast track designation. If a product offers major advances in treatment, the product sponsor may apply for FDA priority review status. Additionally, a product candidate may be designated as a breakthrough therapy if it is intended, either alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or condition and preliminary clinical evidence indicates that the product may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints. The FDA has broad discretion whether or not to grant these designations, so even if we believe a particular product candidate is eligible for such designation or status, the FDA could decide not to grant it. Moreover, even if we do receive such a designation, we may not experience a faster development process, review or approval compared to conventional FDA procedures and there is no assurance that our product candidate will be approved by the FDA.
Even if we complete the necessary preclinical studies and clinical trials, the marketing approval process is expensive, time-consuming and uncertain and may prevent us from obtaining approvals for the commercialization of some or all of our drug candidates. As a result, we cannot predict when or if we, or any collaborators we may have in the future, will obtain marketing approval to commercialize a drug candidate.
The research, testing, manufacturing, labeling, approval, selling, marketing, promotion and distribution of drugs are subject to extensive regulation by the FDA and comparable foreign regulatory authorities, whose laws and regulations may differ from country to country. We are not permitted to market our drug candidates in the United States or in other countries until we, or any collaborators we may have in the future, receive approval of an NDA from the FDA or marketing approval from applicable regulatory authorities outside of the United States. Our drug candidates are in early stages of development and are subject to the risks of failure inherent in drug development. We have not submitted an application for or received marketing approval for any of our drug candidates in the United States or in any other jurisdiction. We have limited experience in conducting and managing the clinical trials necessary to obtain marketing approvals, including FDA approval of an NDA.
The process of obtaining marketing approvals, both in the United States and abroad, is a lengthy, expensive and uncertain process. It may take many years, if approval is obtained at all, and can vary substantially based upon a variety of factors, including the type, complexity and novelty of the drug candidates involved.
In addition, changes in marketing approval policies during the development period, changes in or the enactment or promulgation of additional statutes, regulations or guidance or changes in regulatory review for each submitted drug application, may cause delays in the approval or rejection of an application. Regulatory authorities have substantial discretion in the approval process and may refuse to accept any application or may decide that our data are insufficient for approval and require additional preclinical studies, clinical trials or other
75
Table of Contents
studies and testing. In addition, varying interpretations of the data obtained from preclinical studies and clinical trials could delay, limit or prevent marketing approval of a drug candidate. Any marketing approval we, or any collaborators we may have in the future, ultimately obtain may be limited or subject to restrictions or post-approval commitments that render the approved drug not commercially viable.
Any delay in obtaining or failure to obtain required approvals could materially adversely affect our ability or that of any collaborators we may have to generate revenue from the particular drug candidate, which likely would result in significant harm to our financial position and adversely impact our stock price.
Our failure to obtain marketing approval in foreign jurisdictions would prevent our product candidates from being marketed abroad, and any approval we are granted for our product candidates in the United States would not assure approval of product candidates in foreign jurisdictions.
In order to market and sell our drugs in the European Union and many other jurisdictions, we, and any collaborators we may have in the future, must obtain separate marketing approvals and comply with numerous and varying regulatory requirements. The approval procedure varies among countries and can involve additional testing. The time required to obtain approval may differ substantially from that required to obtain FDA approval. The marketing approval process outside of the United States generally includes all of the risks associated with obtaining FDA approval. In addition, in many countries outside of the United States, it is required that the drug be approved for reimbursement before the drug can be approved for sale in that country. We, and any collaborators we may have in the future, may not obtain approvals from regulatory authorities outside of the United States on a timely basis, if at all. Approval by the FDA does not ensure approval by regulatory authorities in other countries or jurisdictions, and approval by one regulatory authority outside of the United States does not ensure approval by regulatory authorities in other countries or jurisdictions or by the FDA.
Even if we, or any collaborators we may have in the future, obtain marketing approvals for our drug candidates, the terms of approvals and ongoing regulation of our drugs may limit how we, or they, manufacture and market our drugs, which could materially impair our ability to generate revenue.
Once marketing approval has been granted, an approved drug and its manufacturer and marketer are subject to ongoing review and extensive regulation. We, and any collaborators we may have in the future, must therefore comply with requirements concerning advertising and promotion for any of our drug candidates for which we or they obtain marketing approval. Promotional communications with respect to prescription drugs are subject to a variety of legal and regulatory restrictions and must be consistent with the information in the drug’s approved labeling. Thus, we, and any collaborators we may have in the future, may not be able to promote any drugs we develop for indications or uses for which they are not approved.
In addition, manufacturers of approved drugs and those manufacturers’ facilities are required to comply with extensive FDA requirements, including ensuring that quality control and manufacturing procedures conform to cGMPs, which include requirements relating to quality control and quality assurance as well as the corresponding maintenance of records and documentation and reporting requirements. We, our contract manufacturers, our future collaborators and their contract manufacturers could be subject to periodic unannounced inspections by the FDA to monitor and ensure compliance with cGMPs.
Accordingly, assuming we, or our future collaborators, receive marketing approval for one or more of our drug candidates, we, and our future collaborators, and our and their contract manufacturers will continue to expend time, money and effort in all areas of regulatory compliance, including manufacturing, production, product surveillance and quality control.
If we, and our future collaborators, are not able to comply with post-approval regulatory requirements, we, and our future collaborators, could have the marketing approvals for our drugs withdrawn by regulatory authorities and our, or our future collaborators’, ability to market any future drugs could be limited, which could
76
Table of Contents
adversely affect our ability to achieve or sustain profitability. Further, the cost of compliance with post-approval regulations may have a negative effect on our operating results and financial condition.
Any of our drug candidates for which we, or our future collaborators, obtain marketing approval in the future could be subject to post-marketing restrictions or withdrawal from the market and we, and our future collaborators, may be subject to substantial penalties if we, or they, fail to comply with regulatory requirements or if we, or they, experience unanticipated problems with our drugs following approval.
Any of our drug candidates for which we, or our future collaborators, obtain marketing approval in the future, as well as the manufacturing processes, post-approval studies and measures, labeling, advertising and promotional activities for such drug, among other things, will be subject to continual requirements of and review by the FDA and other regulatory authorities. These requirements include submissions of safety and other post-marketing information and reports, registration and listing requirements, requirements relating to manufacturing, quality control, quality assurance and corresponding maintenance of records and documents, requirements regarding the distribution of samples to physicians and recordkeeping. Even if marketing approval of a drug candidate is granted, the approval may be subject to limitations on the indicated uses for which the drug may be marketed or to the conditions of approval, including the requirement to implement a Risk Evaluation and Mitigation Strategy, which could include requirements for a restricted distribution system.
The FDA may also impose requirements for costly post-marketing studies or clinical trials and surveillance to monitor the safety or efficacy of a drug. The FDA and other agencies, including the Department of Justice, or the DOJ, closely regulate and monitor the post-approval marketing and promotion of drugs to ensure that they are manufactured, marketed and distributed only for the approved indications and in accordance with the provisions of the approved labeling. The FDA imposes stringent restrictions on manufacturers’ communications regarding off-label use and if we, or our future collaborators, do not market any of our drug candidates for which we, or they, receive marketing approval for only their approved indications, we, or they, may be subject to warnings or enforcement action for off-label marketing. Violation of the FDCA and other statutes, including the False Claims Act, relating to the promotion and advertising of prescription drugs may lead to investigations or allegations of violations of federal and state health care fraud and abuse laws and state consumer protection laws.
In addition, later discovery of previously unknown adverse events or other problems with our drugs or their manufacturers or manufacturing processes, or failure to comply with regulatory requirements, may yield various results, including:
| • | litigation involving patients taking our drug; |
| • | restrictions on such drugs, manufacturers or manufacturing processes; |
| • | restrictions on the labeling or marketing of a drug; |
| • | restrictions on drug distribution or use; |
| • | requirements to conduct post-marketing studies or clinical trials; |
| • | warning letters or untitled letters; |
| • | withdrawal of the drugs from the market; |
| • | refusal to approve pending applications or supplements to approved applications that we submit; |
| • | recall of drugs; |
| • | fines, restitution or disgorgement of profits or revenues; |
| • | suspension or withdrawal of marketing approvals; |
| • | damage to relationships with any potential collaborators; |
| • | unfavorable press coverage and damage to our reputation; |
77
Table of Contents
| • | refusal to permit the import or export of drugs; |
| • | drug seizure; or |
| • | injunctions or the imposition of civil or criminal penalties. |
Existing laws and future legislation may increase the difficulty and cost for us and our future collaborators to obtain marketing approval of and commercialize our drug candidates and affect the prices we, or they, may obtain.
In the United States and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval of our drug candidates, restrict or regulate post-approval activities and affect our ability, or the ability of our future collaborators, to profitably sell any drugs for which we, or they, obtain marketing approval. We expect that current laws, as well as other healthcare reform measures that be adopted in the future, may result in more rigorous coverage criteria and in additional downward pressure on the price that we, or our future collaborators, may receive for any approved drugs.
In the United States, the Medicare Prescription Drug, Improvement, and Modernization Act of 2003, or the MMA, changed the way Medicare covers and pays for pharmaceutical products and could decrease the coverage and price that we, or our future collaborators, may receive for any approved drugs. While the MMA only addresses drug benefits for Medicare beneficiaries, private payors often follow Medicare coverage policy and payment limitations in setting their own reimbursement rates. Therefore, any reduction in reimbursement that results from the MMA may result in a similar reduction in payments from private payors.
In 2010, President Obama signed into law the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act, or collectively the PPACA.
Among the provisions of the PPACA of potential importance to our drug candidates are the following:
| • | an annual, non-deductible fee on any entity that manufactures or imports specified branded prescription drugs and biologic agents; |
| • | an increase in the statutory minimum rebates a manufacturer must pay under the Medicaid Drug Rebate Program; |
| • | expansion of healthcare fraud and abuse laws, including the False Claims Act and the Anti-Kickback Statute, new government investigative powers and enhanced penalties for non-compliance; |
| • | a new Medicare Part D coverage gap discount program, in which manufacturers must agree to offer 50% point-of-sale discounts off negotiated prices; |
| • | extension of manufacturers’ Medicaid rebate liability; |
| • | expansion of eligibility criteria for Medicaid programs; |
| • | expansion of the entities eligible for discounts under the Public Health Service pharmaceutical pricing program; |
| • | new requirements to report financial arrangements with physicians and teaching hospitals; |
| • | a new requirement to annually report drug samples that manufacturers and distributors provide to physicians; and |
| • | a new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research. |
In addition, other legislative changes have been proposed and adopted since the PPACA was enacted. These new laws may result in additional reductions in Medicare and other healthcare funding and otherwise affect the prices we may obtain for any of our drug candidates for which marketing approval is obtained.
78
Table of Contents
We expect that the PPACA, as well as other healthcare reform measures that may be adopted in the future, may result in more rigorous coverage criteria and in additional downward pressure on the price that we receive for any approved drug. Any reduction in reimbursement from Medicare or other government programs may result in a similar reduction in payments from private payors. The implementation of cost containment measures or other healthcare reforms may prevent us from being able to generate revenue from sales of drugs, attain profitability, or commercialize our drug candidates.
Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for pharmaceutical products. We cannot be sure whether additional legislative changes will be enacted, or whether FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of our drug candidates, if any, may be. In addition, increased scrutiny by the United States Congress of the FDA’s approval process may significantly delay or prevent marketing approval, as well as subject us and our future collaborators to more stringent drug labeling and post-marketing testing and other requirements.
Our relationships with healthcare providers and physicians and third-party payors will be subject to applicable anti-kickback, fraud and abuse and other healthcare laws and regulations, which could expose us to criminal sanctions, civil penalties, contractual damages, reputational harm and diminished profits and future earnings.
Healthcare providers, physicians and third party payors will play a primary role in the recommendation and prescription of any drugs for which we obtain marketing approval. Our future arrangements with third party payors, healthcare providers and physicians may expose us to broadly applicable fraud and abuse and other healthcare laws and regulations that may constrain the business or financial arrangements and relationships through which we market, sell and distribute any drugs for which we obtain marketing approval. These include the following:
| • | Anti-Kickback Statute—the federal healthcare anti-kickback statute prohibits, among other things, persons from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward, or in return for, either the referral of an individual for, or the purchase, order or recommendation or arranging of, any good or service, for which payment may be made under a federal healthcare program such as Medicare and Medicaid; |
| • | False Claims Act—the federal False Claims Act imposes criminal and civil penalties, including through civil whistleblower or qui tam actions, against individuals or entities for, among other things, knowingly presenting, or causing to be presented false or fraudulent claims for payment by a federal healthcare program or making a false statement or record material to payment of a false claim or avoiding, decreasing or concealing an obligation to pay money to the federal government, with potential liability including mandatory treble damages and significant per-claim penalties, currently set at $5,500 to $11,000 per false claim; |
| • | HIPAA—the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters, and, as amended by the Health Information Technology for Economic and Clinical Health Act and its implementing regulations, also imposes obligations, including mandatory contractual terms and technical safeguards, with respect to maintaining the privacy, security and transmission of individually identifiable health information; |
| • | Transparency Requirements—federal laws require applicable manufacturers of covered drugs to report payments and other transfers of value to physicians and teaching hospitals; and |
| • | Analogous State and Foreign Laws—analogous state and foreign fraud and abuse laws and regulations, such as state anti-kickback and false claims laws, can apply to sales or marketing arrangements and claims involving healthcare items or services and are generally broad and are enforced by many different federal and state agencies as well as through private actions. |
79
Table of Contents
Some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government and require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures. State and foreign laws also govern the privacy and security of health information in some circumstances, many of which differ from each other in significant ways and often are not pre-empted by HIPAA, thus complicating compliance efforts.
Efforts to ensure that our business arrangements with third parties will comply with applicable healthcare laws and regulations will involve substantial costs. It is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, imprisonment, exclusion of drugs from government funded healthcare programs, such as Medicare and Medicaid, and the curtailment or restructuring of our operations. If any of the physicians or other healthcare providers or entities with whom we expect to do business is found to be not in compliance with applicable laws, they may be subject to criminal, civil or administrative sanctions, including exclusions from government funded healthcare programs.
Our employees may engage in misconduct or other improper activities, including non-compliance with regulatory standards and requirements, which could cause significant liability for us and harm our reputation.
We are exposed to the risk of employee fraud or other misconduct, including intentional failures to comply with FDA regulations or similar regulations of comparable foreign regulatory authorities, provide accurate information to the FDA or comparable foreign regulatory authorities, comply with manufacturing standards we have established, comply with federal and state healthcare fraud and abuse laws and regulations and similar laws and regulations established and enforced by comparable foreign regulatory authorities, report financial information or data accurately or disclose unauthorized activities to us. Employee misconduct could also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. It is not always possible to identify and deter employee misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws, standards or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business and results of operations, including the imposition of significant fines or other sanctions.
If we fail to comply with environmental, health and safety laws and regulations, we could become subject to fines or penalties or incur costs that could have a material adverse effect on our business.
We are subject to numerous environmental, health and safety laws and regulations, including those governing laboratory procedures and the handling, use, storage, treatment and disposal of hazardous materials and wastes. Our operations involve the use of hazardous and flammable materials, including chemicals and biological and radioactive materials. Our operations also produce hazardous waste products. We generally contract with third parties for the disposal of these materials and wastes. We cannot eliminate the risk of contamination or injury from these materials. In the event of contamination or injury resulting from our use of hazardous materials, we could be held liable for any resulting damages, and any liability could exceed our resources. We also could incur significant costs associated with civil or criminal fines and penalties.
Although we maintain workers’ compensation insurance to cover us for costs and expenses we may incur due to injuries to our employees resulting from the use of hazardous materials, this insurance may not provide adequate coverage against potential liabilities. We do not maintain insurance for environmental liability or toxic
80
Table of Contents
tort claims that may be asserted against us in connection with our storage or disposal of biological, hazardous or radioactive materials.
In addition, we may incur substantial costs in order to comply with current or future environmental, health and safety laws and regulations. These current or future laws and regulations may impair our research, development or commercialization efforts. Failure to comply with these laws and regulations also may result in substantial fines, penalties or other sanctions.
Laws and regulations governing any international operations we may have in the future may preclude us from developing, manufacturing and selling certain drug candidates outside of the United States and require us to develop and implement costly compliance programs.
We are subject to numerous laws and regulations in each jurisdiction outside the United States in which we operate. The creation, implementation and maintenance of international business practices compliance programs is costly and such programs are difficult to enforce, particularly where reliance on third parties is required.
The FCPA prohibits any U.S. individual or business from paying, offering, authorizing payment or offering of anything of value, directly or indirectly, to any foreign official, political party or candidate for the purpose of influencing any act or decision of the foreign entity in order to assist the individual or business in obtaining or retaining business. The FCPA also obligates companies whose securities are listed in the United States to comply with certain accounting provisions requiring the company to maintain books and records that accurately and fairly reflect all transactions of the corporation, including international subsidiaries, and to devise and maintain an adequate system of internal accounting controls for international operations. The anti-bribery provisions of the FCPA are enforced primarily by the DOJ. The Securities and Exchange Commission, or SEC, is involved with enforcement of the books and records provisions of the FCPA.
Compliance with the FCPA is expensive and difficult, particularly in countries in which corruption is a recognized problem. In addition, the FCPA presents particular challenges in the pharmaceutical industry, because, in many countries, hospitals are operated by the government, and doctors and other hospital employees are considered foreign officials. Certain payments to hospitals in connection with clinical trials and other work have been deemed to be improper payments to government officials and have led to FCPA enforcement actions.
Various laws, regulations and executive orders also restrict the use and dissemination outside of the United States, or the sharing with certain non-U.S. nationals, of information classified for national security purposes, as well as certain products and technical data relating to those products. Our expansion outside of the United States, has required, and will continue to require, us to dedicate additional resources to comply with these laws, and these laws may preclude us from developing, manufacturing, or selling certain drugs and drug candidates outside of the United States, which could limit our growth potential and increase our development costs.
The failure to comply with laws governing international business practices may result in substantial penalties, including suspension or debarment from government contracting. Violation of the FCPA can result in significant civil and criminal penalties. Indictment alone under the FCPA can lead to suspension of the right to do business with the U.S. government until the pending claims are resolved. Conviction of a violation of the FCPA can result in long-term disqualification as a government contractor. The termination of a government contract or relationship as a result of our failure to satisfy any of our obligations under laws governing international business practices would have a negative impact on our operations and harm our reputation and ability to procure government contracts. The SEC also may suspend or bar issuers from trading securities on U.S. exchanges for violations of the FCPA’s accounting provisions.
81
Table of Contents
Governments outside of the United States tend to impose strict price controls, which may adversely affect our revenues from the sales of drugs, if any.
In some countries, particularly the countries of the European Union, the pricing of prescription pharmaceuticals is subject to governmental control. In these countries, pricing negotiations with governmental authorities can take considerable time after the receipt of marketing approval for a drug. To obtain reimbursement or pricing approval in some countries, we, or our future collaborators, may be required to conduct a clinical trial that compares the cost-effectiveness of our drug to other available therapies. If reimbursement of our drugs is unavailable or limited in scope or amount, or if pricing is set at unsatisfactory levels, our business could be materially harmed.
Risks Related to Employee Matters and Managing Growth
Our future success depends on our ability to retain our Chief Executive Officer, our President and Chief Scientific Officer and other key executives and to attract, retain and motivate qualified personnel.
We are highly dependent on Michael Kauffman, M.D., Ph.D., our Chief Executive Officer, and Sharon Shacham, Ph.D., M.B.A., our President and Chief Scientific Officer, as well as the other principal members of our management and scientific teams. Although we have entered into formal employment agreements with Drs. Kauffman and Shacham, these agreements do not prevent them from terminating their employment with us at any time. We do not maintain “key person” insurance for any of our executives or other employees. The loss of the services of any of these persons could impede the achievement of our research, development and commercialization objectives.
Recruiting and retaining qualified scientific, clinical, manufacturing and sales and marketing personnel will also be critical to our success. We may not be able to attract and retain these personnel on acceptable terms given the competition among numerous pharmaceutical and biotechnology companies for similar personnel. We also experience competition for the hiring of scientific and clinical personnel from universities and research institutions. In addition, we rely on consultants and advisors, including scientific and clinical advisors, to assist us in formulating our research and development and commercialization strategy. Our consultants and advisors may be employed by employers other than us and may have commitments under consulting or advisory contracts with other entities that may limit their availability to us.
Drs. Kauffman and Shacham are married. The separation or divorce of the couple in the future could adversely affect our business.
Dr. Kauffman, our Chief Executive Officer and member of our board of directors, and Dr. Shacham, our President and Chief Scientific Officer, are married. They are two of our executive officers and are a vital part of our operations. If they were to become separated or divorced or could otherwise not amicably work with each other, one of them may decide to cease his or her employment with us or it could negatively impact our working environment. Alternatively, their work performance may not be satisfactory if they become preoccupied with issues relating to their personal situation. In these cases, our business could be materially harmed.
We expect to expand our development, regulatory and future sales and marketing capabilities, and as a result, we may encounter difficulties in managing our growth, which could disrupt our operations.
We expect to experience significant growth in the number of our employees and the scope of our operations, particularly in the areas of drug development, regulatory affairs and, potentially, sales and marketing. To manage our anticipated future growth, we must continue to implement and improve our managerial, operational and financial systems, expand our facilities and continue to recruit and train additional qualified personnel. Due to our limited financial resources and the limited experience of our management team in managing a company with such anticipated growth, we may not be able to effectively manage the expansion of our operations or recruit and train additional qualified personnel. The physical expansion of our operations may lead to significant costs and
82
Table of Contents
may divert our management and business development resources. Any inability to manage growth could delay the execution of our business plans or disrupt our operations.
Our business and operations may be materially adversely affected in the event of computer system failures or security breaches.
Despite the implementation of security measures, our internal computer systems, and those of our contract research organizations and other third parties on which we rely, are vulnerable to damage from computer viruses, unauthorized access, cyber attacks, natural disasters, fire, terrorism, war and telecommunication and electrical failures. If such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our drug development programs. For example, the loss of clinical trial data from ongoing or planned clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or security breach results in a loss of or damage to our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability and the further development of our drug candidates could be delayed. We may also be vulnerable to cyber attacks by hackers, or other malfeasance. This type of breach of our cybersecurity may compromise our confidential information and/or our financial information and adversely affect our business or result in legal proceedings.
Risks Related to Our Common Stock
Our executive officers, directors and principal stockholders maintain the ability to control all matters submitted to stockholders for approval.
As of December 31, 2015, our executive officers, directors and a small number of stockholders own more than a majority of our outstanding common stock. As a result, if these stockholders were to choose to act together, they would be able to control all matters submitted to our stockholders for approval, as well as our management and affairs. For example, these persons, if they choose to act together, would control the election of directors and approval of any merger, consolidation or sale of all or substantially all of our assets. This concentration of voting power could delay or prevent an acquisition of our company on terms that other stockholders may desire.
Provisions in our corporate charter documents and under Delaware law could make an acquisition of us, which may be beneficial to our stockholders, more difficult and may prevent attempts by our stockholders to replace or remove our current management.
Provisions in our corporate charter and our bylaws may discourage, delay or prevent a merger, acquisition or other change in control of us that stockholders may consider favorable, including transactions in which stockholders might otherwise receive a premium for their shares. These provisions could also limit the price that investors might be willing to pay in the future for shares of our common stock, thereby depressing the market price of our common stock. In addition, because our board of directors is responsible for appointing the members of our management team, these provisions may frustrate or prevent any attempts by our stockholders to replace or remove our current management by making it more difficult for stockholders to replace members of our board of directors. Among other things, these provisions:
| • | establish a classified board of directors such that not all members of the board are elected at one time; |
| • | allow the authorized number of our directors to be changed only by resolution of our board of directors; |
| • | limit the manner in which stockholders can remove directors from the board; |
| • | establish advance notice requirements for stockholder proposals that can be acted on at stockholder meetings and nominations to our board of directors; |
| • | require that stockholder actions must be effected at a duly called stockholder meeting and prohibit actions by our stockholders by written consent; |
83
Table of Contents
| • | limit who may call stockholder meetings; |
| • | authorize our board of directors to issue preferred stock without stockholder approval, which could be used to institute a “poison pill” that would work to dilute the stock ownership of a potential hostile acquirer, effectively preventing acquisitions that have not been approved by our board of directors; and |
| • | require the approval of the holders of at least 75% of the votes that all our stockholders would be entitled to cast to amend or repeal certain provisions of our charter or bylaws. |
Moreover, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporation Law, which prohibits a person who owns in excess of 15% of our outstanding voting stock from merging or combining with us for a period of three years after the date of the transaction in which the person acquired in excess of 15% of our outstanding voting stock, unless the merger or combination is approved in a prescribed manner.
An active trading market for our common stock may not be sustained.
Although our common stock is listed on The NASDAQ Global Select Market, an active trading market for our shares may not be sustained. If an active market for our common stock does not continue, it may be difficult for you to sell shares of our common stock without depressing the market price for the shares, or at all. An inactive trading market for our common stock may also impair our ability to raise capital to continue to fund our operations by selling shares and may impair our ability to acquire other companies or technologies by using our shares as consideration.
If securities analysts do not continue to publish research or reports about our business or if they publish negative evaluations of our stock, the price of our stock could decline.
The trading market for our common stock relies in part on the research and reports that industry or financial analysts publish about us or our business. There can be no assurance that analysts will provide favorable coverage or continue to cover us. If one or more of the analysts covering our business downgrade their evaluations of our stock, the price of our stock could decline. If one or more of these analysts cease to cover our stock, we could lose visibility in the market for our stock, which in turn could cause our stock price to decline.
The price of our common stock has been and may be volatile in the future and fluctuate substantially.
Our stock price has been and is likely to be volatile and may fluctuate substantially. For example, since January 1, 2015, our common stock has traded at prices per share as high as $38.47 and as low as $4.83. The stock market in general and the market for pharmaceutical and biotechnology companies in particular have experienced extreme volatility that has often been unrelated to the operating performance of particular companies. The market price for our common stock may be influenced by many factors, including:
| • | the success of competitive drugs or technologies; |
| • | results of clinical trials of our drug candidates or those of our competitors; |
| • | regulatory or legal developments in the United States and other countries; |
| • | developments or disputes concerning patent applications, issued patents or other proprietary rights; |
| • | the recruitment or departure of key personnel; |
| • | the level of expenses related to any of our drug candidates or clinical development programs; |
| • | the results of our efforts to discover, develop, acquire or in-license additional drug candidates or drugs; |
| • | actual or anticipated changes in estimates as to financial results, development timelines or recommendations by securities analysts; |
84
Table of Contents
| • | variations in our financial results or those of companies that are perceived to be similar to us; |
| • | changes in the structure of healthcare payment systems; |
| • | market conditions in the pharmaceutical and biotechnology sectors; |
| • | general economic, industry and market conditions; and |
| • | the other factors described in this “Risk Factors” section. |
We could be subject to securities class action litigation.
In the past, securities class action litigation has often been brought against a company following a decline in the market price of its securities. This risk is especially relevant for us because pharmaceutical companies have experienced significant stock price volatility in recent years. If we face such litigation, it could result in substantial costs and a diversion of management’s attention and our resources, which could harm our business.
We have broad discretion in the use of our cash and cash equivalents and may not use them effectively.
Our management has broad discretion to use our cash and cash equivalents to fund our operations and could spend these funds in ways that do not improve our results of operations or enhance the value of our common stock. The failure by our management to apply these funds effectively could result in financial losses that could have a material adverse effect on our business, cause the price of our common stock to decline and delay the development of our drug candidates. Pending their use to fund our operations, we may invest our cash and cash equivalents in a manner that does not produce income or that loses value.
We are an “emerging growth company,” and the reduced disclosure requirements applicable to emerging growth companies may make our common stock less attractive to investors.
We are an “emerging growth company,” as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act, and may remain an emerging growth company through 2018. For so long as we remain an emerging growth company, we are permitted and intend to rely on exemptions from certain disclosure requirements that are applicable to other public companies that are not emerging growth companies. These exemptions include not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act of 2002, not being required to comply with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements, reduced disclosure obligations regarding executive compensation and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and shareholder approval of any golden parachute payments not previously approved. We cannot predict whether investors will find our common stock less attractive if we rely on these exemptions. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may be more volatile.
In addition, the JOBS Act provides that an emerging growth company can take advantage of an extended transition period for complying with new or revised accounting standards. This allows an emerging growth company to delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have irrevocably elected not to avail ourselves of this exemption from new or revised accounting standards and, therefore, we will be subject to the same new or revised accounting standards as other public companies that are not emerging growth companies.
We will continue to incur increased costs as a result of operating as a public company, and our management will need to continue to devote substantial time to compliance initiatives and corporate governance practices.
As a public company, and particularly after we are no longer an “emerging growth company,” we will incur significant legal, accounting and other expenses. In addition, the Sarbanes-Oxley Act of 2002 and rules
85
Table of Contents
subsequently implemented by the SEC and NASDAQ have imposed various requirements on public companies, including establishment and maintenance of effective disclosure and financial controls and corporate governance practices. Our management and other personnel will need to continue to devote a substantial amount of time to these compliance initiatives. Moreover, these rules and regulations will increase our legal and financial compliance costs and will make some activities more time-consuming and costly.
We cannot predict with certainty the amount of additional costs we may incur to continue to operate as a public company, nor can we predict the timing of such costs. In addition, the rules and regulations applicable to public companies are often subject to varying interpretations, in many cases due to their lack of specificity, and, as a result, their application in practice may evolve over time as new guidance is provided by regulatory and governing bodies which could result in continuing uncertainty regarding compliance matters and higher costs necessitated by ongoing revisions to disclosure and governance practices.
Pursuant to Section 404 of the Sarbanes-Oxley Act of 2002, or Section 404, we are required to furnish a report by our management on our internal control over financial reporting. However, while we remain an emerging growth company, we are not required to include an attestation report on internal control over financial reporting issued by our independent registered public accounting firm. To achieve compliance with Section 404 within the prescribed period, we are engaged in a process to document and evaluate our internal control over financial reporting, which is both costly and challenging. In this regard, we will need to continue to dedicate internal resources, potentially engage outside consultants and adopt a detailed work plan to assess and document the adequacy of internal control over financial reporting, continue steps to improve control processes as appropriate, validate through testing that controls are functioning as documented and implement a continuous reporting and improvement process for internal control over financial reporting. There is a risk that neither we nor our independent registered public accounting firm will be able to conclude within the prescribed timeframe that our internal control over financial reporting is effective as required by Section 404. This could result in an adverse reaction in the financial markets due to a loss of confidence in the reliability of our financial statements. In addition, if we identify one or more material weaknesses, it could result in an adverse reaction in the financial markets due to a loss of confidence in the reliability of our financial statements.
Because we do not anticipate paying any cash dividends on our capital stock in the foreseeable future, capital appreciation, if any, of our common stock will be the sole source of gain for our stockholders.
We have never declared or paid cash dividends on our capital stock. We currently intend to retain all of our future earnings, if any, to finance the growth and development of our business. In addition, the terms of any future debt agreements may preclude us from paying dividends. As a result, capital appreciation, if any, of our common stock will be the sole source of gain for our stockholders for the foreseeable future.
A significant portion of our total outstanding shares are restricted from immediate resale but may be sold into the market in the near future, which could cause the market price of our common stock to drop significantly, even if our business is doing well.
Sales of a substantial number of shares of our common stock in the public market could occur at any time. These sales, or the perception in the market that the holders of a large number of shares intend to sell shares, could reduce the market price of our common stock. We had 35,864,765 shares outstanding as of December 31, 2015. Of such shares, at least 12.0 million shares are eligible for sale in the public market under Rule 144 of the Securities Act of 1933, as amended, or the Securities Act, subject to the volume limitations and other conditions of Rule 144. The holders of these shares may at any time decide to sell their shares in the public market.
Moreover, holders of an aggregate of approximately 12.1 million shares of our common stock as of December 31, 2015 have rights, subject to some conditions, to require us to file registration statements covering their shares or to include their shares in registration statements that we may file for ourselves or other stockholders. We have also registered all shares of common stock that we may issue under our equity
86
Table of Contents
compensation plans. As a result, these shares can be freely sold in the public market upon issuance, subject to volume limitations applicable to affiliates, to the extent applicable.
Our ability to use our net operating loss carryforwards and tax credit carryforwards to offset future taxable income may be subject to certain limitations.
Under the provisions of the Internal Revenue Code of 1986, as amended, or the Code, our net operating loss and tax credit carryforwards are subject to review and possible adjustment by the Internal Revenue Service (and state tax authorities under relevant state tax rules). The use of net operating loss and tax credit carryforwards may become subject to an annual limitation under Sections 382 and 383 of the Code, respectively, and similar state provisions in the event of certain cumulative changes in the ownership interest of significant shareholders in excess of 50 percent over a three-year period. This could limit the amount of tax attributes that can be utilized annually to offset future taxable income or tax liabilities. The amount of the annual limitation is determined based on the value of a company immediately prior to the ownership change. Subsequent ownership changes may further affect the limitation in future years. Our company has completed several financings since its inception that may have resulted in ownership changes under Sections 382 and 383 of the Code. In addition, future changes in our stock ownership, some of which are outside of our control, could result in ownership changes in the future. For these reasons, we may not be able to use some or all of our net operating loss and tax credit carryforwards, even if we attain profitability prior to the expiration of our net operating loss and tax credit carryforwards.
| Item 1B. | Unresolved Staff Comments |
None.
| Item 2. | Properties |
Our headquarters are located in Newton, Massachusetts, where we occupy approximately 46,167 square feet of office and laboratory space. In 2015, in order to accommodate our need for additional office and laboratory space, we amended our Newton, Massachusetts lease for an additional 16,234 square feet, which is included in the total above. We also occupy approximately 3,681 square feet of office space in Munich, Germany, which we began to occupy in 2015.
| Item 3. | Legal Proceedings |
We are not a party to any material legal proceedings.
| Item 4. | Mine Safety Disclosures |
Not applicable.
87
Table of Contents
| Item 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Market Information
Our common stock, $0.0001 par value per share, began trading on the NASDAQ Global Select Market on November 6, 2013, where its prices are quoted under the symbol “KPTI.”
Price Range of Our Common Stock
The following table sets forth the reported high and low sales prices of our common stock as reported on the NASDAQ Global Select Market for each quarter in the years ended December 31, 2015 and 2014:
| Year Ended December 31, 2015 |
||||||||
| High | Low | |||||||
| First Quarter |
$ | 38.47 | $ | 24.35 | ||||
| Second Quarter |
$ | 35.65 | $ | 24.72 | ||||
| Third Quarter |
$ | 27.71 | $ | 10.00 | ||||
| Fourth Quarter |
$ | 19.41 | $ | 10.35 | ||||
| Year Ended December 31, 2014 |
||||||||
| High | Low | |||||||
| First Quarter |
$ | 47.87 | $ | 21.13 | ||||
| Second Quarter |
$ | 47.98 | $ | 23.86 | ||||
| Third Quarter |
$ | 47.89 | $ | 32.97 | ||||
| Fourth Quarter |
$ | 49.01 | $ | 29.24 | ||||
Holders
As of March 1, 2016, there were 10 holders of record of our common stock.
Dividends
We have never paid cash dividends on our common stock, and we do not expect to pay any cash dividends in the foreseeable future.
88
Table of Contents
Stock Performance Graph
The following graph shows a comparison from November 6, 2013, the date on which our common stock first began trading on the NASDAQ Global Select Market, through December 31, 2015, of the cumulative total return on an assumed investment of $100.00 in cash in our common stock as compared to the same investment in the NASDAQ Composite Index and the NASDAQ Biotechnology Index. Such returns are based on historical results and are not intended to suggest future performance. Data for the NASDAQ Composite Index and NASDAQ Biotechnology Index assume reinvestment of dividends.

Cumulative Total Return Comparison
| 11/6/13 | 12/31/13 | 12/31/14 | 12/31/15 | |||||||||||||
| Karyopharm Therapeutics Inc. |
100.00 | 142.80 | 233.21 | 82.55 | ||||||||||||
| NASDAQ Composite |
100.00 | 106.84 | 121.45 | 128.59 | ||||||||||||
| NASDAQ Biotechnology |
100.00 | 108.50 | 143.80 | 152.18 | ||||||||||||
The performance graph in this Item 5 is not deemed to be “soliciting material” or to be “filed” with the SEC for purposes of Section 18 of the Exchange Act, as amended, or otherwise subject to the liabilities under that Section, and shall not be deemed incorporated by reference into any filing of Karyopharm Therapeutics Inc. under the Securities Act or the Exchange Act, except to the extent we specifically incorporate it by reference into such a filing.
89
Table of Contents
Recent Sales of Unregistered Securities
None.
Use of Proceeds from Registered Securities
On November 12, 2013, we issued and sold 6,800,000 shares of our common stock in the IPO at a public offering price of $16.00 per share, for aggregate gross proceeds of $108.8 million. On December 10, 2013, we issued and sold 1,020,000 shares of our common stock pursuant to the underwriters’ full exercise of their option to purchase additional shares in the IPO at $16.00 per share for gross proceeds of $16.3 million. All of the shares issued and sold in the IPO were registered under the Securities Act pursuant to a Registration Statement on Form S-1 (File No. 333-191584), which was declared effective by the SEC on November 5, 2013, and a Registration Statement on Form S-1 (File No. 333-192110) filed pursuant to Rule 462(b) of the Securities Act. Merrill Lynch, Pierce, Fenner & Smith Incorporated and Leerink Swann LLC acted as joint-book-running managers of the offering and as representatives of the underwriters. JMP Securities LLC and Oppenheimer & Co. Inc. acted as co-managers for the offering. The offering commenced on November 5, 2013 and terminated upon sale of all of the shares offered.
The net offering proceeds to us, after deducting underwriting discounts of $8.8 million and offering expenses payable by us totaling $3.2 million, were approximately $113.2 million. No offering expenses or net offering proceeds were paid directly or indirectly to any of our directors or officers (or their associates) or persons owning 10.0% or more of any class of our equity securities or to any other affiliates.
As of December 31, 2015, we have used all of such net offering proceeds to fund the continued clinical development of our lead drug candidate, selinexor, the preclinical development of our drug candidates for anti-inflammatory, viral and wound healing indications, the discovery, research and preclinical development of additional drug candidates and for working capital and other general corporate purposes. We are holding a significant portion of the balance of the net proceeds from the offering in interest-bearing money market accounts, prime money market funds and other short-term investments. There has been no material change in our planned use of the balance of the net proceeds from the offering described in the prospectus filed by us with the SEC pursuant to Rule 424(b)(4) on November 7, 2013.
90
Table of Contents
| Item 6. | Selected Financial Data |
You should read the following selected financial data together with our consolidated financial statements and the related notes appearing elsewhere in this Annual Report on Form 10-K and the “Management’s discussion and analysis of financial condition and results of operations” section of this Annual Report on Form 10-K. The selected historical financial information in this section is not intended to replace our financial statements and the related notes therein. Our historical results for any prior period are not necessarily indicative of results to be expected in any future period.
| Years Ended December 31, | ||||||||||||||||||||
| 2015 | 2014 | 2013 | 2012 | 2011 | ||||||||||||||||
| (In thousands, except share and per share amounts) | ||||||||||||||||||||
| Consolidated Statement of Operations Data: |
||||||||||||||||||||
| Contract and grant revenue |
$ | 250 | $ | 229 | $ | 387 | $ | 634 | $ | 152 | ||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Operating expenses: |
||||||||||||||||||||
| Research and development |
97,744 | 60,127 | 28,452 | 14,095 | 8,623 | |||||||||||||||
| General and administrative |
21,582 | 15,948 | 5,885 | 2,429 | 1,840 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Total operating expenses |
119,326 | 76,075 | 34,337 | 16,524 | 10,463 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Loss from operations |
(119,076 | ) | (75,846 | ) | (33,950 | ) | (15,890 | ) | (10,311 | ) | ||||||||||
| Other income, net |
895 | 69 | 3 | 2 | — | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Net loss |
$ | (118,181 | ) | $ | (75,777 | ) | $ | (33,947 | ) | $ | (15,888 | ) | $ | (10,311 | ) | |||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Net loss per share—basic and diluted |
$ | (3.32 | ) | $ | (2.43 | ) | $ | (5.59 | ) | $ | (8.95 | ) | $ | (10.27 | ) | |||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Weighted-average number of common shares used in net loss per share—basic and diluted |
35,619,506 | 31,135,694 | 6,067,679 | 1,775,323 | 1,004,144 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| As of December 31, | ||||||||||||||||||||
| 2015 | 2014 | 2013 | 2012 | 2011 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Consolidated Balance Sheet Data: |
||||||||||||||||||||
| Cash, cash equivalents and short-term investments |
$ | 175,633 | $ | 205,724 | $ | 155,974 | $ | 391 | $ | 6,512 | ||||||||||
| Working capital |
162,468 | 195,450 | 154,664 | (976 | ) | 4,749 | ||||||||||||||
| Total assets |
215,443 | 220,337 | 158,226 | 1,311 | 7,224 | |||||||||||||||
| Total preferred stock and preferred stock subscription |
— | — | — | 27,258 | 17,758 | |||||||||||||||
| Total stockholders’ equity (deficit) |
198,365 | 206,794 | 154,934 | (27,877 | ) | (12,651 | ) | |||||||||||||
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations |
The following discussion of our financial condition and results of operations should be read in conjunction with our consolidated financial statements and related notes included elsewhere in this report. Some of the information contained in this discussion and analysis and set forth elsewhere in this report, including information with respect to our plans and strategy for our business, includes forward-looking statements that involve risks and uncertainties. You should review the section titled “Risk Factors” in Part I—Item 1A of this report for a discussion of important factors that could cause actual results to differ materially from the results described in or implied by the forward-looking statements contained in the following discussion and analysis.
91
Table of Contents
Business Overview
Overview
We are a clinical-stage pharmaceutical company focused on the discovery, development and subsequent commercialization of novel, first-in-class drugs directed against nuclear transport and related targets for the treatment of cancer and other major diseases. Our scientific expertise is focused on understanding the regulation of intracellular communication between the nucleus and the cytoplasm. We have discovered and are developing wholly-owned, novel, small molecule Selective Inhibitor of Nuclear Export, or SINE™, compounds that inhibit the nuclear export protein XPO1. These SINE compounds represent a new class of drug candidates with a novel mechanism of action that have the potential to treat a variety of diseases in areas of unmet medical need. Our SINE compounds were the first oral XPO1 inhibitors in clinical development.
Our initial focus is on seeking the regulatory approval and commercialization of our lead drug candidate, selinexor (KPT-330), as an orally administered agent in cancer indications with significant unmet clinical need, initially for hematologic malignancies. We then plan to seek additional approvals for the use of selinexor in combination therapies to expand the patient populations that are eligible for selinexor, as well as to move selinexor further towards front-line cancer therapy. We are also advancing the clinical development of selinexor in multiple solid tumor indications. To date, we have initiated multiple later-phase clinical trials to evaluate selinexor in hematological cancers and solid tumors. We have also initiated a double-blinded, placebo-controlled, randomized Phase 2/3 study of single-agent selinexor in liposarcoma and expect to initiate in the middle of 2016 a double-blinded, randomized Phase 2/3 study of selinexor in combination with carfilzomib (Kyprolis®) and dexamethasone to treat multiple myeloma. We are preparing to establish the commercial infrastructure to support a potential launch of selinexor for hematologic indications in North America and Western Europe.
We have devoted substantially all of our efforts to research and development. We expect that it will be several years, if ever, before we have a drug candidate ready for commercialization for the treatment of human disease. To date, we have financed our operations primarily with the net proceeds from the private placements of our preferred stock and the net proceeds from our initial public offering.
As of December 31, 2015, we had an accumulated deficit of $256.5 million. We had net losses of $118.2 million, $75.8 million and $33.9 million for the years ended December 31, 2015, 2014 and 2013, respectively. We have not generated any revenue to date from sales of any drugs.
We expect to continue to incur significant expenses and increasing operating losses for the foreseeable future. The net losses we incur may fluctuate significantly from quarter to quarter. We anticipate that our expenses will increase substantially if and as we:
| • | continue our research and preclinical and clinical development of our drug candidates; |
| • | identify additional drug candidates; |
| • | initiate additional clinical trials for our drug candidates; |
| • | seek marketing approvals for any of our drug candidates that successfully complete clinical trials; |
| • | establish a sales, marketing and distribution infrastructure to commercialize any drugs for which we may obtain marketing approval; |
| • | maintain, expand and protect our intellectual property portfolio; |
| • | manufacture our drug candidates; |
| • | hire additional clinical, quality control and scientific personnel; |
| • | acquire or in-license other drugs and technologies; and |
92
Table of Contents
| • | add operational, financial and management information systems and personnel, including personnel to support our drug development, any future commercialization efforts and our operations as a public company. |
Financial Overview
Revenue Recognition
To date, we have not generated any revenue from drug sales and do not expect to generate any revenue from drug sales for several years, if ever. Our ability to generate revenues from drug sales will depend on the successful development and eventual commercialization of our drug candidates.
To date, our only revenue is from foundation and government grants and contracts.
Research and Development Expenses
Research and development expenses consist primarily of costs incurred for our research activities, including our drug discovery efforts, and the development of our drug candidates, which include:
| • | employee-related expenses, including salaries, benefits, travel and stock-based compensation expense; |
| • | expenses incurred under agreements with third parties, including contract research organizations, contract manufacturing organizations and consultants that conduct clinical trials and preclinical studies; |
| • | the cost of acquiring, developing and manufacturing clinical trial materials; |
| • | facilities, depreciation and other expenses, which include direct and allocated expenses for rent and maintenance of facilities, insurance, and other operating costs; and |
| • | costs associated with preclinical activities and regulatory operations. |
Costs for certain development activities, such as clinical trials, are recognized based on an evaluation of the progress to completion of specific tasks using data such as patient enrollment, clinical site activations, and information provided to us by our vendors on their actual costs incurred. Payments for these activities are based on the terms of the individual arrangements, which may differ from the pattern of costs incurred, and are reflected in the financial statements as prepaid or accrued research and development.
Since our research and development has been focused primarily on using our drug discovery and optimization platform to identify drug candidates, we have not historically tracked research and development costs by project. In addition, we use our employee and infrastructure resources across multiple research and development projects. The majority of our research and development expenses to date have been related to selinexor. We expect to begin to track costs by project when drug candidates other than selinexor enter clinical trials in humans.
The successful development of our drug candidates is highly uncertain. As such, at this time, we cannot reasonably estimate or know the nature, timing and estimated costs of the efforts that will be necessary to complete the remainder of the development of these drug candidates. We are also unable to predict when, if ever, material net cash inflows will commence from any drug candidates. This is due to the numerous risks and uncertainties associated with developing drugs, including the uncertainty of:
| • | establishing an appropriate safety profile with IND-enabling toxicology studies, and ongoing clinical trials; |
| • | successful enrollment in, and completion of, clinical trials; |
| • | receipt of marketing approvals from applicable regulatory authorities; |
93
Table of Contents
| • | establishing commercial manufacturing capabilities or making arrangements with third-party manufacturers; |
| • | obtaining and maintaining patent and trade secret protection and regulatory exclusivity for our drug candidates; |
| • | establishing commercial sales and marketing capabilities and launching commercial sales of the drugs, if and when approved, whether alone or in collaboration with others; and |
| • | maintaining a continued acceptable safety profile of the drugs following approval. |
A change in the outcome of any of these variables with respect to the development of any of our drug candidates would significantly change the costs and timing associated with the development of that drug candidate.
Research and development activities are central to our business model. Drug candidates in later stages of clinical development generally have higher development costs than those in earlier stages of clinical development, primarily due to the increased size and duration of later-stage clinical trials. We expect research and development costs to increase significantly for the foreseeable future as our drug candidates progress in clinical trials. However, we do not believe that it is possible at this time to accurately project total program-specific expenses through commercialization. There are numerous factors associated with the successful commercialization of any of our drug candidates, including future trial design and various regulatory requirements, many of which cannot be determined with accuracy at this time based on our stage of development. Additionally, future commercial and regulatory factors beyond our control will impact our clinical development programs and plans.
General and Administrative Expenses
General and administrative expenses consist primarily of salaries, benefits, travel, and other related costs, including stock-based compensation, for personnel in executive, finance and administrative functions. Other significant costs include facility costs not otherwise included in research and development expenses, legal fees relating to patent and corporate matters and fees for accounting and consulting services.
We anticipate that our general and administrative expenses will increase in the future to support continued research and development activities, potential commercialization of our drug candidates and increased costs of operating as a public company. These increases will likely include increased costs related to the hiring of additional personnel and fees to outside consultants, lawyers and accountants, among other expenses.
Other Income (Expense)
Other income consists primarily of interest income earned on our cash and cash equivalents and short-term and long-term investments. Other expense consists primarily of foreign currency transaction losses associated with our German subsidiary whose functional currency is the Euro.
Critical Accounting Policies and Estimates
Our discussion and analysis of our financial condition and results of operations are based on our consolidated financial statements, which we have prepared in accordance with United States generally accepted accounting principles. The preparation of these consolidated financial statements requires us to make estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements, as well as the reported amounts of revenues and expenses during the reporting periods. On an ongoing basis, we evaluate our estimates and judgments, including those described in greater detail below. We base our estimates on historical experience and on various other factors that
94
Table of Contents
we believe are reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions.
While our significant accounting policies are described in more detail in the notes to our consolidated financial statements included elsewhere in this Form 10-K, we believe that the following accounting policies are the most critical to aid you in fully understanding and evaluating our financial condition and results of operations.
Accrued Research and Development Expenses
As part of the process of preparing our consolidated financial statements, we are required to estimate our accrued research and development expenses. This process involves reviewing quotations and contracts, identifying services that have been performed on our behalf and estimating the level of service performed and the associated cost incurred for the service when we have not yet been invoiced or otherwise notified of the actual cost. The majority of our service providers invoice us monthly in arrears for services performed or when contractual milestones are met. We make estimates of our accrued expenses as of each balance sheet date in our financial statements based on facts and circumstances known to us at that time. We periodically confirm the accuracy of our estimates with the service providers and make adjustments if necessary. The significant estimates in our accrued research and development expenses include fees paid to contract research organizations, or CROs, and contract manufacturing organizations, or CMOs, in connection with research and development activities for which we have not yet been invoiced.
We base our expenses related to CROs and CMOs on our estimates of the services received and efforts expended pursuant to quotes and contracts with CROs and CMOs that conduct research and development on our behalf. The financial terms of these agreements are subject to negotiation, vary from contract to contract and may result in uneven payment flows. There may be instances in which payments made to our vendors will exceed the level of services provided and result in a prepayment of the research and development expense. In accruing service fees, we estimate the time period over which services will be performed and the level of effort to be expended in each period. If the actual timing of the performance of services or the level of effort varies from our estimate, we adjust the accrual or prepayment accordingly. Although we do not expect our estimates to be materially different from amounts actually incurred, if our estimates of the status and timing of services performed differ from the actual status and timing of services performed, it could result in us reporting amounts that are too high or too low in any particular period. Our estimates have not been materially different than amounts actually incurred to date.
Stock-based Compensation
We issue stock-based awards to employees and non-employees, generally in the form of stock options, restricted stock and restricted stock units. We account for our stock-based awards to employees in accordance with Financial Accounting Standards Board, or FASB, Accounting Standards Codification, or ASC, Topic 718, Compensation—Stock Compensation, or ASC 718. ASC 718 requires all stock-based awards to employees, including grants of employee stock options and modifications to existing stock options, to be recognized in the consolidated statements of operations and comprehensive loss based on their fair values. We account for stock-based awards to non-employees in accordance with FASB ASC Topic 505-50, Equity-Based Payments to Non-Employees, which requires the award to be re-measured at fair value as the award vests. We recognize the compensation cost of stock-based awards to employees on a straight-line basis over the vesting period of the award and by using an accelerated attribution model for awards to non-employees. Described below is the methodology we have utilized in measuring stock-based compensation expense.
We estimate the fair value of our options to employees and non-employees using the Black-Scholes option pricing model, which requires the input of assumptions, including (a) the expected volatility of our stock, (b) the
95
Table of Contents
expected term of the option, (c) the risk-free interest rate, and (d) expected dividends. Since there was no public market for our common stock prior to our initial public offering, we lacked company specific historical and implied volatility data. In addition, as a newly public company, we do not have sufficient history to estimate the volatility of our common stock price or the expected life of the options. Therefore, we base our estimate of expected volatility on the historical volatility of a group of representative companies that are publicly traded. For these analyses, we select companies with comparable characteristics to ours including enterprise value, risk profiles, position within the industry, and with historical share price information sufficient to meet the expected term of the options. We compute the historical volatility data using the closing prices for the selected companies’ shares during the equivalent period of the calculated expected term of our options. We will continue to apply this process until a sufficient amount of historical information regarding the volatility of our own stock price becomes available. We estimate the expected term of our employee stock options using the “simplified” method pursuant to Staff Accounting Bulletin No., 107 Share-based payments, whereby the expected term equals the average of the vesting term and the original contractual term of the option. For non-employee stock options, we utilize the contractual term of the option. The risk-free interest rates for periods within the expected term of the option are based on the U.S. Treasury yield curve in effect during the period the options were granted. We have not paid and do not anticipate paying cash dividends on our shares of common stock; therefore, the expected dividend yield is assumed to be zero.
We are also required to estimate forfeitures at the time of grant, and revise those estimates in subsequent periods if actual forfeitures differ from estimates. We use historical data to estimate pre-vesting option forfeitures and record stock-based compensation expense only for those options that are expected to vest. To the extent that actual forfeitures differ from our estimates, the difference is recorded as a cumulative adjustment in the period the estimates were revised. Stock-based compensation expense recognized in the financial statements is based on options that ultimately vest.
Results of Operations
The following table summarizes our results of operations for the years ended December 31, 2015, 2014 and 2013:
| Years Ended December 31, | ||||||||||||
| 2015 | 2014 | 2013 | ||||||||||
| (in thousands) | ||||||||||||
| Contract and grant revenue |
$ | 250 | $ | 229 | $ | 387 | ||||||
|
|
|
|
|
|
|
|||||||
| Operating expenses: |
||||||||||||
| Research and development |
97,744 | 60,127 | 28,452 | |||||||||
| General and administrative |
21,582 | 15,948 | 5,885 | |||||||||
|
|
|
|
|
|
|
|||||||
| Loss from operations |
(119,076 | ) | (75,846 | ) | (33,950 | ) | ||||||
| Other income, net |
895 | 69 | 3 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net loss |
$ | (118,181 | ) | $ | (75,777 | ) | $ | (33,947 | ) | |||
|
|
|
|
|
|
|
|||||||
Comparison of Years Ended December 31, 2015 and 2014
Contract and Grant Revenue. We recognize revenue pursuant to a sponsored research agreement. Contract and grant revenue for the year ended December 31, 2015 was $0.3 million compared to $0.2 million for the year ended December 31, 2014. The increase in revenue was the result of recognizing more revenue pursuant to grant funding during the year ended December 31, 2015.
96
Table of Contents
Research and Development Expense. Research and development expense increased by approximately $37.6 million to $97.7 million for the year ended December 31, 2015 from $60.1 million for the year ended December 31, 2014. The increase primarily related to:
| • | an increase of approximately $25.1 million in clinical trial costs, primarily related to an increase of approximately $18.6 million pertaining to selinexor (which included increases of approximately $20.4 million in external clinical trial costs, partially offset by decreases of approximately $1.9 million for manufacturing costs) and approximately $4.0 million pertained to our other pipeline programs; |
| • | an increase of $10.7 million in personnel costs, primarily due to increased headcount and an increase of $4.6 million in stock-based compensation expense related to equity awards granted to personnel; |
| • | an increase of $1.2 million in consulting fees, primarily due to an increase of $4.5 million paid to consultants pertaining to selinexor and other pipeline programs, offset by a decrease of $3.3 million in stock-based compensation expense related to equity awards granted to consultants, primarily due to the lower fair value of our common stock; |
| • | a decrease of $1.1 million in preclinical efficacy and toxicology study costs; and |
| • | a decrease of approximately $0.8 million in discovery work, including preclinical studies and screening; |
General and Administrative Expense. General and administrative expense increased by approximately $5.7 million to approximately $21.6 million for the year ended December 31, 2015 from approximately $15.9 million for the year ended December 31, 2014. The increase is primarily related to:
| • | an increase of approximately $4.6 million in personnel costs, primarily due to increased headcount and an increase of approximately $3.3 million in stock-based compensation expense related to equity awards granted to personnel; and |
| • | an increase of approximately $0.8 million in occupancy expense, primarily due to our expansion of our office space during the year. |
Other Income, net. Other income, net increased by approximately $0.9 million to approximately $0.9 million for the year ended December 31, 2015, from less than $0.1 million for the year ended December 31, 2014. The increase is primarily related to interest income earned on our investments.
Comparison of Years Ended December 31, 2014 and 2013
Contract and Grant Revenue. We recognize revenue pursuant to a sponsored research agreement. Contract and grant revenue for the year ended December 31, 2014 was $0.2 million compared to $0.4 million for the year ended December 31, 2013. The decrease in revenue was the result of recognizing less revenue pursuant to grant funding during the year ended December 31, 2014.
Research and Development Expense. Research and development expense increased by approximately $31.6 million to $60.1 million for the year ended December 31, 2014 from $28.5 million for the year ended December 31, 2013. The increase primarily related to:
| • | an increase of $14.7 million in clinical trial costs, primarily related to an increase of approximately $10.6 million in costs to CROs, and an increase of $6.9 million in costs related to the manufacture of selinexor, partially offset by a decrease of $2.8 million related to the manufacture of verdinexor; |
| • | an increase of $6.3 million in personnel costs, primarily due to an increased headcount and an increase of $3.1 million in stock-based compensation expense related to equity awards granted to personnel, primarily related to the higher fair value of our common stock; |
| • | an increase of $4.3 million in consulting fees, primarily due to an increase of $2.8 million paid to consultants and an increase of $1.5 million in stock-based compensation expense related to equity awards granted to consultants, primarily due to the higher fair value of our common stock; |
97
Table of Contents
| • | an increase of $4.0 million in preclinical efficacy and toxicology study costs; |
| • | an increase of approximately $1.1 million in discovery work, including preclinical studies and screening; and |
| • | a decrease of approximately $1.0 million in costs related to our clinical trials of verdinexor in pet dogs. |
General and Administrative Expense. General and administrative expense increased by approximately $10.0 million to approximately $15.9 million for the year ended December 31, 2014 from approximately $5.9 million for the year ended December 31, 2013. The increase is primarily related to:
| • | an increase of approximately $4.7 million in personnel costs, primarily due to increased headcount and an increase of approximately $3.3 million in stock-based compensation expense related to equity awards granted to personnel, primarily related to the higher fair value of our common stock; |
| • | an increase of approximately $2.8 million in consulting fees, primarily related to an increase in stock-based compensation expense related to equity awards granted to consultants, primarily due to the higher fair value of our common stock, partially offset by decreases in costs for consultants related to finance and business development; |
| • | an increase of approximately $2.0 million in professional fees, primarily related to higher legal fees for protecting our intellectual property, higher corporate legal fees, and higher public and investor relations fees and other fees to operate as a public company; and |
| • | an increase of approximately $0.5 million in insurance expense, primarily due to our becoming a publicly traded company. |
Other Income, net. Other income, net was less than $0.1 million for all periods presented.
Liquidity and Capital Resources
To date, we have not generated any material revenues. We have financed our operations to date principally through private placements of our preferred stock and proceeds from our initial public offering and follow-on offerings.
As of December 31, 2015, we had $210.0 million in cash, cash equivalents, restricted cash and short- and long-term investments. In July 2014, we completed a public offering of 2,844,334 shares of our common stock at a public offering price of $42.50 per share. We received net proceeds of approximately $112.8 million, after deducting underwriting discounts, commissions and expenses payable by us. In January 2015, we completed an underwritten offering of 2,950,000 shares of our common stock at public price of $33.00 per share. We received net proceeds of approximately $90.8 million, after deducting the underwriting discount and offering expenses payable by us. As of December 31, 2015, we commenced a controlled equity offering of our common stock, pursuant to which we may sell shares of our common stock with an aggregate offering price of up to $50.0 million. As of December 31, 2015, we had sold an aggregate of 121,314 shares of common stock in this offering for net proceeds of approximately $1.5 million.
98
Table of Contents
Cash flows
The following table provides information regarding our cash flows:
| Years Ended December 31, | ||||||||||||
| 2015 | 2014 | 2013 | ||||||||||
| (in thousands) | ||||||||||||
| Net cash used in operating activities |
$ | (94,029 | ) | $ | (51,447 | ) | $ | (30,290 | ) | |||
| Net cash used in investing activities |
(90,823 | ) | (67,031 | ) | (57 | ) | ||||||
| Net cash provided by financing activities |
92,700 | 113,121 | 185,930 | |||||||||
| Effect of exchange rate changes |
(99 | ) | (8 | ) | — | |||||||
|
|
|
|
|
|
|
|||||||
| Net (decrease) increase in cash and cash equivalents |
$ | (92,251 | ) | $ | (5,365 | ) | $ | 155,583 | ||||
|
|
|
|
|
|
|
|||||||
Net Cash Used in Operating Activities
Net cash used in operating activities was $94.0 million during the year ended December 31, 2015 compared to $51.4 million during the year ended December 31, 2014. The $42.6 million increase in cash used in operating activities during the year ended December 31, 2015 was driven primarily by an increase in our net loss adjusted for non-cash charges and changes in the components of working capital due to an increase in research and development expenses as we increased our research and development headcount and increased spending on external research and development costs related to selinexor.
Net cash used in operating activities was $51.4 million during the year ended December 31, 2014 compared to $30.3 million during the year ended December 31, 2013. The $21.1 million increase in cash used in operating activities during the year ended December 31, 2014 was driven primarily by an increase in our net loss adjusted for non-cash charges and changes in the components of working capital due to an increase in research and development expenses as we increased our research and development headcount and increased spending on external research and development costs related to selinexor.
Net Cash Used in Investing Activities
Net cash used in investing activities was $90.8 million during the year ended December 31, 2015 compared to $67.0 million during the year ended December 31, 2014. The cash used in investing activities for the year ended December 31, 2015 increased $23.8 million primarily related to an increase of $241.4 million in purchases of investments, offset by a decrease of $1.4 million in purchases of property and equipment related to the renovation of the new office space and a $215.9 million increase in the proceeds from maturities of investments.
Net cash used in investing activities was $67.0 million during the year ended December 31, 2014. The cash used in investing activities for the year ended December 31, 2014 reflects an increase of $63.8 million in purchases of investments, $0.4 million in restricted cash related to a facility lease and the purchase of $2.8 million of property and equipment related to the renovation of and relocation to new office and laboratory space. There was less than $0.1 million in investing activities for the year ended December 31, 2013.
Net Cash Provided by Financing Activities
Net cash provided by financing activities was $92.7 million during the year ended December 31, 2015 compared to $113.1 million during the year ended December 31, 2014. The cash provided by financing activities for the year ended December 31, 2015 reflects net proceeds of $90.8 million from the sale of common stock as part of a public offering of our common stock in January 2015, net proceeds of $1.5 million from the sale of common stock under a controlled equity offering agreement in December 2015, and the proceeds from the exercise of stock options and shares issued under our employee stock purchase plan. The cash provided by
99
Table of Contents
financing activities during the year ended December 31, 2014 reflects net proceeds of $112.8 million from the sale of common stock as part of a public offering of our common stock in July 2014, and the proceeds from the exercise of options and shares under our employee stock purchase plan.
Net cash provided by financing activities was $113.1 million during the year ended December 31, 2014 compared to $185.9 million during the year ended December 31, 2013. The cash provided by financing activities for the year ended December 31, 2014 reflects net proceeds of $112.8 million from the sale of common stock as part of a public offering of our common stock in July 2014, and the proceeds from the exercise of stock options and shares issued under our employee stock purchase plan. The cash provided by financing activities during the year ended December 31, 2013 was driven primarily by proceeds of $72.4 million from the sale of preferred stock and proceeds of $113.2 million from our initial public offering.
Funding requirements
We expect our expenses to increase in connection with our ongoing activities, particularly as we continue the clinical trials of, and assuming positive results of our clinical trials and based on regulatory feedback, if and when we seek marketing approval for, selinexor and our other drug candidates. In addition, if we obtain marketing approval for any of our drug candidates, we expect to incur significant commercialization expenses related to drug sales, marketing, manufacturing and distribution to the extent that such sales, marketing, manufacturing and distribution are not the responsibility of any collaborator that we may have at such time for any such drug. Furthermore, we expect to incur additional costs associated with operating as a public company. Accordingly, we will need to obtain substantial additional funding in connection with our continuing operations. If we are unable to raise capital when needed or on attractive terms, we would be forced to delay, reduce or eliminate our research and development programs or future commercialization efforts.
We expect that our existing cash, cash equivalents and short- and long-term investments will enable us to fund our current operating plan and capital expenditure requirements into the middle of 2018. Our future capital requirements will depend on many factors, including:
| • | the progress and results of our current and planned clinical trials of selinexor; |
| • | the scope, progress, results and costs of drug discovery, preclinical development, laboratory testing and clinical trials for our other drug candidates; |
| • | the costs, timing and outcome of regulatory reviews of our drug candidates; |
| • | our ability to establish and maintain collaborations on favorable terms, if at all; |
| • | the success of any collaborations that we may enter into with third parties; |
| • | the extent to which we acquire or in-license other drugs and technologies; |
| • | the costs of future commercialization activities, including drug sales, marketing, manufacturing and distribution, for any of our drug candidates for which we receive marketing approval, to the extent that such sales, marketing, manufacturing and distribution are not the responsibility of any collaborator that we may have at such time; |
| • | the amount of revenue, if any, received from commercial sales of our drug candidates, should any of our drug candidates receive marketing approval; and |
| • | the costs of preparing, filing and prosecuting patent applications, maintaining and enforcing our intellectual property rights and defending intellectual property-related claims. |
Identifying potential drug candidates and conducting preclinical studies and clinical trials is a time-consuming, expensive and uncertain process that takes years to complete, and we may never generate the necessary data or results required to obtain marketing approval and achieve drug sales. In addition, our drug
100
Table of Contents
candidates, if approved, may not achieve commercial success. Our commercial revenues, if any, will be derived from sales of drugs that we do not expect to be commercially available for many years, if at all. Accordingly, we will need to continue to rely on additional financing to achieve our business objectives. Adequate additional financing may not be available to us on acceptable terms, or at all. In addition, we may seek additional capital due to favorable market conditions or strategic considerations, even if we believe we have sufficient funds for our current or future operating plans.
Contractual Obligations
As of December 31, 2015, we had the following contractual obligations:
| Payments Due by Period | ||||||||||||||||||||
| Contractual Obligations |
Total | Less than 1 Year |
1 to 3 Years |
3 to 5 Years |
More than 5 Years |
|||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Operating lease obligations(1) |
$ | 9,483 | $ | 1,326 | $ | 4,270 | $ | 3,887 | $ | — | ||||||||||
| Purchase obligations(2) |
— | — | — | — | — | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Total contractual cash obligations |
$ | 9,483 | $ | 1,326 | $ | 4,270 | $ | 3,887 | $ | — | ||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| (1) | Represents future minimum lease payments under our non-cancelable operating lease. |
| (2) | We enter into agreements in the normal course of business with CROs and CMOs for clinical trials and clinical supply manufacturing and with vendors for preclinical research. We have not included these payments in the table of contractual obligations above since the contracts are cancelable at any time by us, generally upon 30 days prior written notice to the vendor. |
Royalty payments associated with our agreements have not been included in the above table of contractual obligations as we cannot reasonably estimate if or when they will occur. At this time, no royalty payments are probable of occurrence.
Multiple Myeloma Research Foundation
In July 2011, we entered into a research agreement with the Multiple Myeloma Research Foundation, or MMRF, for the research and development of small molecule XPO1 inhibitor compounds for the treatment of multiple myeloma. Pursuant to the research agreement, MMRF awarded us a $1.0 million grant, all of which has been paid to us based on our achievement of specified milestones. We own all inventions and other intellectual property that arose or will arise from the conduct of the research program, which we refer to as program inventions and program intellectual property, respectively.
If we, our affiliates, licensees or transferees commercialize products incorporating a program invention or program intellectual property, which we call research program products, we would be obligated to pay to MMRF mid- single-digit royalties as a percentage of worldwide net sales of research program products, including selinexor, sold by us, our affiliates, licensees or transferees. If we out-license rights to a research program product, we are obligated to pay MMRF a percentage of certain payments we receive from our licensee for the grant of such rights. If we sell all or substantially all of our assets to one or more third parties who were not our stockholders on the effective date of the agreement, or if one or more third parties acquire more than fifty percent of our equity and payments are made directly to our stockholders for the sale of their shares of our stock, each of which we call a change of control, we will be obligated to pay to MMRF a percentage of the value we or our shareholders receive in connection with such change of control. The maximum aggregate amount we may be obligated to pay to MMRF for royalties, out-licensing our rights or as a result of a change of control is $6.0 million.
While this agreement has expired in accordance with its terms, our payment obligations survive the expiration of the agreement.
101
Table of Contents
Off-Balance Sheet Arrangements
We did not have, during the periods presented, and we do not currently have, any off-balance sheet arrangements, as defined under applicable Securities and Exchange Commission rules.
Inflation
We do not believe that inflation has had a significant impact on our revenues or results of operations since inception.
Recently Issued Accounting Pronouncements
Recent accounting pronouncements which may be applicable to us are described in “Note 2. Summary of Significant Accounting Policies” in our Consolidated Financial Statements contained herein in Part II, Item 8.
| Item 7A. | Quantitative and Qualitative Disclosures about Market Risk |
We are exposed to market risk related to changes in interest rates. As of December 31, 2015 and 2014, we had cash, cash equivalents, restricted cash and investments of $210.0 million and $214.8 million, respectively. Our primary exposure to market risk is interest rate sensitivity, which is affected by changes in the general level of U.S. interest rates. Due to the short-term maturities of our cash equivalents and the low risk profile of our investments, an immediate 10% change in interest rates would not have a material effect on the fair market value of our cash equivalents or investment portfolio.
We do not believe our cash, cash equivalents, restricted cash and investments have significant risk of default or illiquidity. While we believe our cash, cash equivalents and investments do not contain excessive risk, we cannot provide absolute assurance that in the future our investments will not be subject to adverse changes in market value. In addition, we maintain significant amounts of cash, cash equivalents and available-for-sale securities at one or more financial institutions that are in excess of federally insured limits. Given the potential instability of financial institutions, we cannot provide assurance that we will not experience losses on these deposits.
We are also exposed to market risk related to change in foreign currency exchange rates. We contract with CROs and CMOs that are located in Canada and Europe, which are denominated in foreign currencies. We also contract with a number of clinical trial sites outside the United States, and our budgets for those studies are frequently denominated in foreign currencies. We are subject to fluctuations in foreign currency rates in connection with these agreements. We do not currently hedge our foreign currency exchange rate risk.
| Item 8. | Financial Statements and Supplementary Data |
Our consolidated financial statements, together with the reports of our independent registered public accounting firms, appear on pages 106 through 113 of this Annual Report on Form 10-K.
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
The Company has established disclosure controls and procedures designed to ensure that information required to be disclosed in the reports that the Company files or submits under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the rules and forms prescribed by the Securities and Exchange Commission and is accumulated and communicated to management, including the principal executive officer (our Chief Executive Officer) and principal financial officer (our Executive Vice President, Chief Financial Officer), to allow timely decisions regarding required disclosure.
102
Table of Contents
Our management, under the supervision and with the participation of our Chief Executive Officer and Executive Vice President, Chief Financial Officer, has evaluated the effectiveness of our disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act) as of the end of the period covered by this Annual Report on Form 10-K. Management recognizes that any disclosure controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives. Our disclosure controls and procedures have been designed to provide reasonable assurance of achieving their objectives. Based on such evaluation, our Chief Executive Officer and Executive Vice President, Chief Financial Officer, concluded that our disclosure controls and procedures were effective at the reasonable assurance level as of December 31, 2015.
Management’s Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Rules 13a-15(f) and 15d-15(f) of the Exchange Act. Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with policies or procedures may deteriorate. Our internal control over financial reporting is a process designed under the supervision of our principal executive officer and principal financial officer to provide reasonable assurance regarding the reliability of financial reporting and the preparation of our financial statements for external reporting purposes in accordance with U.S. generally accepted accounting principles.
Under the supervision and with the participation of management, including our principal executive officer and principal financial officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting based on the 2013 framework in Internal Control –Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on our evaluation under that framework, management concluded that our internal control over financial reporting was effective as of December 31, 2015.
Attestation Report of the Registered Public Accounting Firm
This report does not include an attestation report of our independent registered public accounting firm regarding internal control over financial reporting.
Changes in Internal Control over Financial Reporting
There were no changes in our internal control over financial reporting identified in connection with the evaluation required by Rule 13a-15(d) and 15d-15(d) of the Exchange Act that occurred during the quarter ended December 31, 2015 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
None.
103
Table of Contents
Certain information required by Part III is omitted from this Annual Report on Form 10-K and is incorporated by reference from our definitive proxy statement relating to our 2016 annual meeting of stockholders, pursuant to Regulation 14A of the Exchange Act, which we refer to as our 2016 Proxy Statement. We expect to file our 2016 Proxy Statement with the SEC no later than April 29, 2016.
| Item 10. | Directors, Executive Officers and Corporate Governance |
Information regarding our directors, including the audit committee and audit committee financial experts, and executive officers and compliance with Section 16(a) of the Exchange Act will be included in our 2016 Proxy Statement and is incorporated herein by reference.
We have adopted a Code of Business Conduct and Ethics for all of our directors, officers and employees as required by NASDAQ governance rules and as defined by applicable SEC rules. Stockholders may locate a copy of our Code of Business Conduct and Ethics on our website at www.karyopharm.com or request a copy without charge from:
Karyopharm Therapeutics Inc.
Attention: Investor Relations
85 Wells Avenue, 2nd Floor
Newton, MA 02459
We will post to our website any amendments to the Code of Business Conduct and Ethics, and any waivers that are required to be disclosed by the rules of either the SEC or NASDAQ.
| Item 11. | Executive Compensation |
The information required by this Item 11 of Form 10-K regarding executive compensation will be included in our 2016 Proxy Statement and is incorporated herein by reference.
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
The information required by this Item 12 of Form 10-K regarding security ownership of certain beneficial owners and management will be included in our 2016 Proxy Statement and is incorporated herein by reference.
| Item 13. | Certain Relationships and Related Transactions, and Director Independence |
The information required by this Item 13 of Form 10-K regarding certain relationships and related transactions and director independence will be included in our 2016 Proxy Statement and is incorporated herein by reference.
| Item 14. | Principal Accountant Fees and Services |
The information required by this Item 14 of Form 10-K regarding principal accountant fees and services will be included in our 2016 Proxy Statement and is incorporated herein by reference.
104
Table of Contents
| Item 15. | Exhibits and Financial Statement Schedules |
(a)(1) Financial Statements
The financial statements listed below are filed as a part of this Annual Report on Form 10-K.
(a)(2) Financial Statement Schedules
All financial schedules have been omitted because the required information is either presented in the consolidated financial statements or the notes thereto or is not applicable or required.
(a)(3) Exhibits
The exhibits required by Item 601 of Regulation S-K and Item 15(b) of this Annual Report on Form 10-K are listed in the Exhibit Index immediately preceding the exhibits and are incorporated herein.
105
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and
Shareholders of Karyopharm Therapeutics Inc.
We have audited the accompanying consolidated balance sheets of Karyopharm Therapeutics Inc. (the Company) as of December 31, 2015 and 2014, and the related consolidated statements of operations, comprehensive loss, convertible preferred stock and stockholders’ equity (deficit), and cash flows for the years then ended. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. We were not engaged to perform an audit of the Company’s internal control over financial reporting. Our audits included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of Karyopharm Therapeutics Inc. at December 31, 2015 and 2014, and the consolidated results of its operations and its cash flows for the years then ended, in conformity with U.S. generally accepted accounting principles.
/s/ Ernst & Young LLP
Boston, Massachusetts
March 15, 2016
106
Table of Contents
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders
Karyopharm Therapeutics Inc.
We have audited the accompanying consolidated statements of operations, comprehensive loss, convertible preferred stock and stockholders’ equity (deficit), and cash flows for the year ended December 31, 2013 of Karyopharm Therapeutics Inc. and subsidiary (the “Company”). These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audit provides a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the results of the operations of Karyopharm Therapeutics Inc. and subsidiary and their cash flows for the year ended December 31, 2013, in conformity with U.S. generally accepted accounting principles.
/s/ RSM US LLP
Boston, Massachusetts
March 21, 2014
107
Table of Contents
Karyopharm Therapeutics Inc.
(in thousands, except share and per share amounts)
| December 31, 2015 |
December 31, 2014 |
|||||||
| ASSETS |
||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 58,358 | $ | 150,609 | ||||
| Short-term investments |
117,275 | 55,115 | ||||||
| Prepaid expenses and other current assets |
1,967 | 2,027 | ||||||
|
|
|
|
|
|||||
| Total current assets |
177,600 | 207,751 | ||||||
| Property and equipment, net |
3,483 | 2,754 | ||||||
| Long-term investments |
33,878 | 8,658 | ||||||
| Other assets |
— | 774 | ||||||
| Restricted cash |
482 | 400 | ||||||
|
|
|
|
|
|||||
| Total assets |
$ | 215,443 | $ | 220,337 | ||||
|
|
|
|
|
|||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY |
||||||||
| Current liabilities: |
||||||||
| Accounts payable |
$ | 3,808 | $ | 6,288 | ||||
| Accrued expenses |
11,023 | 5,825 | ||||||
| Deferred rent |
206 | 126 | ||||||
| Other current liabilities |
95 | 62 | ||||||
|
|
|
|
|
|||||
| Total current liabilities |
15,132 | 12,301 | ||||||
| Deferred rent, net of current portion |
1,946 | 1,242 | ||||||
|
|
|
|
|
|||||
| Total liabilities |
17,078 | 13,543 | ||||||
|
|
|
|
|
|||||
| Commitments and contingencies (Note 8) |
||||||||
| Stockholders’ equity: |
||||||||
| Preferred stock, $0.0001 par value; 5,000,000 shares authorized; none issued and outstanding |
— | — | ||||||
| Common stock, $0.0001 par value; 100,000,000 shares authorized; 35,864,765 and 32,699,380 shares issued and outstanding at December 31, 2015 and 2014, respectively |
4 | 3 | ||||||
| Additional paid-in capital |
455,170 | 345,166 | ||||||
| Accumulated other comprehensive loss |
(282 | ) | (29 | ) | ||||
| Accumulated deficit |
(256,527 | ) | (138,346 | ) | ||||
|
|
|
|
|
|||||
| Total stockholders’ equity |
198,365 | 206,794 | ||||||
|
|
|
|
|
|||||
| Total liabilities and stockholders’ equity |
$ | 215,443 | $ | 220,337 | ||||
|
|
|
|
|
|||||
The accompanying notes are an integral part of these consolidated financial statements.
108
Table of Contents
Karyopharm Therapeutics Inc.
Consolidated Statements of Operations
(in thousands, except share and per share amounts)
| For the Years Ended December 31, | ||||||||||||
| 2015 | 2014 | 2013 | ||||||||||
| Contract and grant revenue |
$ | 250 | $ | 229 | $ | 387 | ||||||
|
|
|
|
|
|
|
|||||||
| Operating expenses: |
||||||||||||
| Research and development |
97,744 | 60,127 | 28,452 | |||||||||
| General and administrative |
21,582 | 15,948 | 5,885 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total operating expenses |
119,326 | 76,075 | 34,337 | |||||||||
|
|
|
|
|
|
|
|||||||
| Loss from operations |
(119,076 | ) | (75,846 | ) | (33,950 | ) | ||||||
| Other income (expense): |
||||||||||||
| Interest income |
897 | 97 | 3 | |||||||||
| Interest expense |
— | (1 | ) | — | ||||||||
| Other expense |
(2 | ) | (27 | ) | — | |||||||
|
|
|
|
|
|
|
|||||||
| Total other income, net |
895 | 69 | 3 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net loss |
$ | (118,181 | ) | $ | (75,777 | ) | $ | (33,947 | ) | |||
|
|
|
|
|
|
|
|||||||
| Net loss per share—basic and diluted |
$ | (3.32 | ) | $ | (2.43 | ) | $ | (5.59 | ) | |||
|
|
|
|
|
|
|
|||||||
| Weighted-average number of common shares outstanding used in net loss per share—basic and diluted |
35,619,506 | 31,135,694 | 6,067,679 | |||||||||
|
|
|
|
|
|
|
|||||||
The accompanying notes are an integral part of these consolidated financial statements.
109
Table of Contents
Karyopharm Therapeutics Inc.
Consolidated Statements of Comprehensive Loss
(in thousands)
| For the Years Ended December 31, | ||||||||||||
| 2015 | 2014 | 2013 | ||||||||||
| Net loss |
$ | (118,181 | ) | $ | (75,777 | ) | $ | (33,947 | ) | |||
|
|
|
|
|
|
|
|||||||
| Other comprehensive loss: |
||||||||||||
| Unrealized loss on investments |
(167 | ) | (22 | ) | — | |||||||
| Foreign currency translation adjustment |
(86 | ) | (7 | ) | — | |||||||
|
|
|
|
|
|
|
|||||||
| Comprehensive loss |
$ | (118,434 | ) | $ | (75,806 | ) | $ | (33,947 | ) | |||
|
|
|
|
|
|
|
|||||||
The accompanying notes are an integral part of these consolidated financial statements.
110
Table of Contents
Karyopharm Therapeutics Inc.
Consolidated Statements of Convertible Preferred Stock and Stockholders’ Equity (Deficit)
(in thousands, except share amounts)
| Special Participation Shares |
Series A Convertible Preferred Shares |
Series A-2 Convertible Preferred Shares |
Series A-3 Convertible Preferred Shares |
Series A-4 Convertible Preferred Shares |
Series B Convertible Preferred Shares |
Series B-1 Convertible Preferred Shares |
||||||||||||||||||||||||||||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | Shares | Amount | Shares | Amount | Shares | Amount | Shares | Amount | Shares | Amount | |||||||||||||||||||||||||||||||||||||||||||
| Balance at December 31, 2012 |
10,000 | — | 18,437,500 | 18,278 | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Issuance of Series A preferred stock |
— | — | 2,500,000 | 2,500 | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Proceeds from the sale of Series A-3 convertible preferred stock |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Proceeds from the sale of Series B convertible preferred stock |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Issuance of Series B preferred stock, net of issuance costs of $143 |
— | — | — | — | — | — | — | — | — | — | 23,100,000 | 46,057 | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Issuance of Series B-1 preferred stock, net of issuance costs of $123 |
— | — | — | — | — | — | — | — | — | — | — | — | 8,636,362 | 18,877 | ||||||||||||||||||||||||||||||||||||||||||
| Issuance of shares related to preferred stock subscription |
— | — | — | — | 6,100,000 | 6,980 | 1,764,706 | 3,000 | 1,538,461 | 2,000 | 1,000,000 | 2,000 | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Conversion of convertible preferred stock into common stock |
— | — | (20,937,500 | ) | (20,778 | ) | (6,100,000 | ) | (6,980 | ) | (1,764,706 | ) | (3,000 | ) | (1,538,461 | ) | (2,000 | ) | (24,100,000 | ) | (48,057 | ) | (8,636,362 | ) | (18,877 | ) | ||||||||||||||||||||||||||||||
| Settlement of special participation preferred shares |
(10,000 | ) | — | — | — | — | — | — | — | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
| Exercise of stock options |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Vesting of restricted stock |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Initial Public Offering, net of issuance costs of $3,207 |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
| Balance at December 31, 2013 |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Vesting of restricted stock |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Exercise of stock options and shares issued under the employee stock purchase plan |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Issuance of common stock upon public offering, net of issuance costs of $794 |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Unrealized loss on investments |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
| Balance at December 31, 2014 |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Vesting of restricted stock |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Exercise of stock options and shares issued under the employee stock purchase plan |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Issuance of common stock upon public offering, net of issuance costs of $6,520 |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Issuance of common stock, net of issuance costs of $284 |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Unrealized loss on investments |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | — | — | — | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
| Balance at December 31, 2015 |
— | $ | — | — | $ | — | — | $ | — | — | $ | — | — | $ | — | — | $ | — | — | $ | — | |||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
111
Table of Contents
Karyopharm Therapeutics Inc.
Consolidated Statements of Convertible Preferred Stock and Stockholders’ Equity (Deficit) — (Continued)
(in thousands, except share amounts)
| Preferred Stock Subscription |
|
Common Shares | ||||||||||||||||||||||||||||||||
| Shares | Amount |
|
Shares | Amount | Additional Paid-In Capital |
Accumulated Other Comprehensive Loss |
Accumulated Deficit |
Total Stockholders’ Equity (Deficit) |
||||||||||||||||||||||||||
| Balance at December 31, 2012 |
7,638,461 | $ | 8,980 | 2,123,388 | $ | — | $ | 745 | $ | — | $ | (28,622 | ) | $ | (27,877 | ) | ||||||||||||||||||
| Issuance of Series A preferred stock |
— | — | — | — | — | — | — | — | ||||||||||||||||||||||||||
| Proceeds from the sale of Series A-3 convertible preferred stock |
1,764,706 | 3,000 | — | — | — | — | — | — | ||||||||||||||||||||||||||
| Proceeds from the sale of Series B convertible preferred stock |
1,000,000 | 2,000 | — | — | — | — | — | — | ||||||||||||||||||||||||||
| Issuance of Series B preferred stock, net of issuance costs of $143 |
— | — | — | — | — | — | — | — | ||||||||||||||||||||||||||
| Issuance of Series B-1 preferred stock, net of issuance costs of $123 |
— | — | — | — | — | — | — | — | ||||||||||||||||||||||||||
| Issuance of shares related to preferred stock subscription |
(10,403,167 | ) | (13,980 | ) | — | — | — | — | — | — | ||||||||||||||||||||||||
| Conversion of convertible preferred stock into common stock |
— | — | 19,114,241 | 2 | 99,689 | — | — | 99,691 | ||||||||||||||||||||||||||
| Settlement of special participation preferred shares |
— | — | 12,121 | — | 88 | — | — | 88 | ||||||||||||||||||||||||||
| Exercise of stock options |
— | — | 79,122 | — | 34 | — | — | 34 | ||||||||||||||||||||||||||
| Vesting of restricted stock |
— | — | 438,386 | — | 5 | — | — | 5 | ||||||||||||||||||||||||||
| Initial Public Offering, net of issuance costs of $3,207 |
— | — | 7,820,000 | 1 | 113,154 | — | — | 113,155 | ||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | — | — | 3,785 | — | — | 3,785 | ||||||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | (33,947 | ) | (33,947 | ) | ||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
| Balance at December 31, 2013 |
— | — | 29,587,258 | 3 | 217,500 | — | (62,569 | ) | 154,934 | |||||||||||||||||||||||||
| Vesting of restricted stock |
— | — | 155,058 | — | 305 | — | — | 305 | ||||||||||||||||||||||||||
| Exercise of stock options and shares issued under the employee stock purchase plan |
— | — | 112,730 | — | 284 | — | — | 284 | ||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | — | — | 14,240 | — | — | 14,240 | ||||||||||||||||||||||||||
| Issuance of common stock upon public offering, net of issuance costs of $794 |
— | — | 2,844,334 | — | 112,837 | — | — | 112,837 | ||||||||||||||||||||||||||
| Unrealized loss on investments |
— | — | — | — | — | (22 | ) | — | (22 | ) | ||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | (7 | ) | — | (7 | ) | ||||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | (75,777 | ) | (75,777 | ) | ||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
| Balance at December 31, 2014 |
— | — | 32,699,380 | 3 | 345,166 | (29 | ) | (138,346 | ) | $ | 206,794 | |||||||||||||||||||||||
| Vesting of restricted stock |
— | — | 11,410 | — | — | — | — | — | ||||||||||||||||||||||||||
| Exercise of stock options and shares issued under the employee stock purchase plan |
— | — | 82,661 | — | 616 | — | — | 616 | ||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | — | — | 17,057 | — | — | 17,057 | ||||||||||||||||||||||||||
| Issuance of common stock upon public offering, net of issuance costs of $6,520 |
— | — | 2,950,000 | — | 90,830 | — | — | 90,830 | ||||||||||||||||||||||||||
| Issuance of common stock, net of issuance costs of $284 |
— | — | 121,314 | 1 | 1,501 | — | — | 1,502 | ||||||||||||||||||||||||||
| Unrealized loss on investments |
— | — | — | — | — | (167 | ) | — | (167 | ) | ||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | (86 | ) | — | (86 | ) | ||||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | (118,181 | ) | (118,181 | ) | ||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
| Balance at December 31, 2015 |
— | $ | — | 35,864,765 | $ | 4 | $ | 455,170 | $ | (282 | ) | $ | (256,527 | ) | $ | 198,365 | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
112
Table of Contents
Karyopharm Therapeutics Inc.
Consolidated Statements of Cash Flows
(in thousands)
| For the Year Ended December 31, | ||||||||||||
| 2015 | 2014 | 2013 | ||||||||||
| Operating activities |
||||||||||||
| Net loss |
$ | (118,181 | ) | $ | (75,777 | ) | $ | (33,947 | ) | |||
| Adjustments to reconcile net loss to net cash used in operating activities: |
||||||||||||
| Depreciation and amortization |
634 | 323 | 144 | |||||||||
| Noncash consulting expense |
— | — | 88 | |||||||||
| Loss on disposal of fixed assets |
— | 50 | — | |||||||||
| Net amortization of premiums and discounts on investments |
1,778 | 2 | — | |||||||||
| Stock-based compensation expense |
17,057 | 14,240 | 3,785 | |||||||||
| Change in operating assets and liabilities: |
||||||||||||
| Prepaid expenses and other current assets |
(55 | ) | (45 | ) | (1,419 | ) | ||||||
| Other assets |
500 | (470 | ) | — | ||||||||
| Accounts payable |
(2,426 | ) | 4,496 | 664 | ||||||||
| Accrued expenses and other liabilities |
5,766 | 4,445 | 382 | |||||||||
| Deferred revenue |
— | (79 | ) | 13 | ||||||||
| Deferred rent |
213 | 1,368 | — | |||||||||
| Cash received related to tenant lease incentives |
685 | — | — | |||||||||
|
|
|
|
|
|
|
|||||||
| Net cash used in operating activities |
(94,029 | ) | (51,447 | ) | (30,290 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Investing activities |
||||||||||||
| Purchases of property and equipment |
(1,416 | ) | (2,834 | ) | (57 | ) | ||||||
| Increase in restricted cash |
(82 | ) | (400 | ) | — | |||||||
| Proceeds from maturities of investments |
215,867 | — | — | |||||||||
| Purchases of investments |
(305,192 | ) | (63,797 | ) | — | |||||||
|
|
|
|
|
|
|
|||||||
| Net cash used in investing activities |
(90,823 | ) | (67,031 | ) | (57 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Financing activities |
||||||||||||
| Proceeds from issuance of common stock, net of issuance costs |
92,084 | 112,837 | 113,155 | |||||||||
| Proceeds from the exercise of stock options and shares issued under employee stock purchase plan |
616 | 284 | 341 | |||||||||
| Proceeds from sale of convertible preferred stock, net of issuance costs |
— | — | 72,434 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net cash provided by financing activities |
92,700 | 113,121 | 185,930 | |||||||||
|
|
|
|
|
|
|
|||||||
| Effect of exchange rate on cash |
(99 | ) | (8 | ) | — | |||||||
| Net (decrease) increase in cash and cash equivalents |
(92,251 | ) | (5,365 | ) | 155,583 | |||||||
| Cash and cash equivalents, beginning of period |
150,609 | 155,974 | 391 | |||||||||
|
|
|
|
|
|
|
|||||||
| Cash and cash equivalents, end of period |
$ | 58,358 | $ | 150,609 | $ | 155,974 | ||||||
|
|
|
|
|
|
|
|||||||
| Supplemental disclosure of non-cash investing and financing activities: |
||||||||||||
| Property and equipment purchases included in accounts payable |
$ | — | $ | 52 | $ | — | ||||||
|
|
|
|
|
|
|
|||||||
| Issuance of preferred stock in satisfaction of preferred stock subscription |
$ | — | $ | — | $ | 13,980 | ||||||
|
|
|
|
|
|
|
|||||||
| Preferred stock conversion to common stock |
$ | — | $ | — | $ | 99,691 | ||||||
|
|
|
|
|
|
|
|||||||
| Vesting of restricted common stock |
$ | — | $ | 305 | $ | 5 | ||||||
|
|
|
|
|
|
|
|||||||
| Deferred financing costs included in accounts payable and accrued expenses |
$ | 26 | $ | 274 | $ | — | ||||||
|
|
|
|
|
|
|
|||||||
The accompanying notes are an integral part of these consolidated financial statements.
113
Table of Contents
Karyopharm Therapeutics Inc.
Notes to Consolidated Financial Statements
(in thousands, except share and per share amounts)
1. Organization and Operations
The Company
Karyopharm Therapeutics Inc. (the “Company”) is a clinical stage pharmaceutical company that seeks to discover, develop, and commercialize drugs to treat cancer and certain other major diseases. It was incorporated in Delaware on December 22, 2008 and has a principal place of business in Newton, Massachusetts.
The Company’s operations to date have consisted primarily of raising capital, product research and development, and initial market development.
The Company has not generated any revenue related to its primary business purpose to date and is subject to a number of risks similar to those of other early stage life science companies, including rapid technology change, regulatory approval of products, uncertainty of market acceptance of products, compliance with government regulations, protection of proprietary technology, dependence on key individuals, competition from other companies, the need for development of commercially viable products, and the need to obtain adequate additional financing to fund the development of its product candidates.
The Company has generated an accumulated deficit of $256,527 since inception. The Company has financed its operations primarily through private placements of its preferred stock, an initial public offering (“IPO”) completed in November 2013 and two follow-on offerings of common stock as well as a controlled equity offering. The Company has not completed development of any product candidate and has devoted substantially all of its financial resources and efforts to research and development, including preclinical and clinical development. The Company expects to continue to incur significant expenses and increasing operating losses for at least several years. The Company believes its cash, cash equivalents, and investments as of December 31, 2015 and proceeds from its controlled equity offering commenced in December 2015 will be sufficient to allow the Company to fund its current operating plan through at least January 1, 2017.
2. Summary of Significant Accounting Policies
Basis of Presentation
The accompanying financial statements have been prepared in accordance with accounting principles generally accepted in the United States of America (“U.S. GAAP”).
Segment Information
Operating segments are defined as components of an enterprise about which separate discrete information is available for evaluation by the chief operating decision maker, or decision-making group, in deciding how to allocate resources and in assessing performance. The Company views its operations and manages its business in one operating segment, which is the business of discovering, developing and commercializing drugs to treat cancer and certain other major diseases. All of the Company’s revenues are derived in the United States. All material long-lived assets of the Company reside in the United States.
Use of Estimates
The preparation of financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period.
114
Table of Contents
On an ongoing basis, the Company’s management evaluates its estimates, including estimates related to clinical trial accruals, stock-based compensation expense, and reported amounts of revenues and expenses during the reported period. The Company bases its estimates on historical experience and other market-specific or other relevant assumptions that it believes to be reasonable under the circumstances. Although the Company regularly assesses these estimates, actual results could differ from those estimates. Changes in estimates are recorded in the period in which they become known.
Principles of Consolidation
The consolidated financial statements at December 31, 2015 include the accounts of Karyopharm Therapeutics Inc. (a Delaware corporation), the accounts of Karyopharm Securities Corp. (“KPSC”, a wholly-owned Massachusetts corporation of the Company incorporated in December 2013), the accounts of Karyopharm Europe GmbH (a wholly-owned German Limited Liability Company, incorporated in September 2014), and the accounts of Karyopharm Therapeutics (Bermuda) Ltd. (a limited liability company, registered in Bermuda in March 2015).
Cash and Cash Equivalents
Cash equivalents consist primarily of demand deposit accounts and deposits in short-term money market funds. Cash equivalents are stated at cost, which approximates fair value. The Company considers all highly liquid investments with maturities of three months or less from the date of purchase to be cash equivalents.
Investments
The Company determines the appropriate classification of its investments in debt securities at the time of purchase. All of the Company’s securities are classified as available-for-sale and are reported in short-term investments or long-term investments based on maturity dates and whether such assets are reasonably expected to be realized in cash or sold or consumed during the normal cycle of business. Available-for-sale investments are recorded at fair value, with unrealized gains or losses included in Accumulated Other Comprehensive Loss on the Company’s Consolidated Balance Sheets, exclusive of other-than-temporary impairment losses, if any. Short-term and long-term investments are comprised of corporate debt securities, commercial paper, U.S. government agency securities and certificates of deposit.
Concentrations of Credit Risk and Off-Balance Sheet Risk
Financial instruments which potentially subject the Company to credit risk consist primarily of cash, cash equivalents and investment securities. The Company holds these investments in highly rated financial institutions, and, by policy, limits the amounts of credit exposure to any one financial institution. These amounts at times may exceed federally insured limits. The Company has not experienced any credit losses in such accounts and does not believe it is exposed to any significant credit risk on these funds. The Company has no off-balance sheet concentrations of credit risk, such as foreign currency exchange contracts, option contracts or other hedging arrangements.
Fair Value Measurements
Financial instruments, including cash, restricted cash, prepaid expenses and other current assets, accounts payable and accrued expenses, are presented in the consolidated financial statements at amounts that approximate fair value at December 31, 2015 and 2014.
The Company is required to disclose information on all assets and liabilities reported at fair value that enables an assessment of the inputs used in determining the reported fair values. The fair value hierarchy prioritizes valuation inputs based on the observable nature of those inputs. The fair value hierarchy applies only
115
Table of Contents
to the valuation inputs used in determining the reported fair value of the investments and is not a measure of the investment credit quality. The hierarchy defines three levels of valuation inputs:
| Level 1 inputs | Quoted prices in active markets for identical assets or liabilities | |
| Level 2 inputs | Inputs other than quoted prices included within Level 1 that are observable for the asset or liability, either directly or indirectly | |
| Level 3 inputs |
Unobservable inputs that reflect the Company’s own assumptions about the assumptions market participants would use in pricing the asset or liability | |
The Company’s cash equivalents are comprised of money market funds. The Company measures these investments at fair value. The fair value of cash equivalents is determined based on “Level 1” inputs.
Items classified as Level 2 within the valuation hierarchy consist of commercial paper, corporate debt securities, U.S. government agency securities and certificates of deposit. The Company estimates the fair values of these marketable securities by taking into consideration valuations obtained from third-party pricing sources. These pricing sources utilize industry standard valuation models, including both income and market-based approaches, for which all significant inputs are observable, either directly or indirectly, to estimate fair value. These inputs include market pricing based on real-time trade data for the same or similar securities, issuer credit spreads, benchmark yields, and other observable inputs. The Company validates the prices provided by its third-party pricing sources by understanding the models used, obtaining market values from other pricing sources and analyzing pricing data in certain instances.
The following table presents information about the Company’s financial assets that have been measured at fair value at December 31, 2015 and indicates the fair value hierarchy of the valuation inputs utilized to determine such fair value (in thousands):
| Description |
Total | Quoted Prices in Active Markets (Level 1) |
Significant Other Observable Inputs (Level 2) |
Significant Unobservable Inputs (Level 3) |
||||||||||||
| Financial assets |
||||||||||||||||
| Cash equivalents: |
||||||||||||||||
| Money market funds |
$ | 49,172 | $ | 49,172 | $ | — | $ | — | ||||||||
| Investments: |
||||||||||||||||
| Current: |
||||||||||||||||
| Corporate debt securities |
86,447 | — | 86,447 | — | ||||||||||||
| Commercial paper |
29,828 | 29,828 | ||||||||||||||
| U.S. government and agency securities |
1,000 | — | 1,000 | — | ||||||||||||
| Non-current: |
||||||||||||||||
| Corporate debt securities (one to two year maturity) |
33,878 | — | 33,878 | — | ||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| $ | 200,325 | $ | 49,172 | $ | 151,153 | $ | — | |||||||||
|
|
|
|
|
|
|
|
|
|||||||||
116
Table of Contents
The following table presents information about the Company’s financial assets that have been measured at fair value at December 31, 2014 and indicates the fair value hierarchy of the valuation inputs utilized to determine such fair value (in thousands):
| Description |
Total | Quoted Prices in Active Markets (Level 1) |
Significant Other Observable Inputs (Level 2) |
Significant Unobservable Inputs (Level 3) |
||||||||||||
| Financial assets |
||||||||||||||||
| Cash equivalents: |
||||||||||||||||
| Money market funds |
$ | 129,209 | $ | 129,209 | $ | — | $ | — | ||||||||
| Investments: |
||||||||||||||||
| Current: |
||||||||||||||||
| Certificates of deposit |
15,000 | — | 15,000 | — | ||||||||||||
| Corporate debt securities |
10,135 | 10,135 | ||||||||||||||
| Commercial paper |
29,980 | — | 29,980 | — | ||||||||||||
| Non-current: |
||||||||||||||||
| Corporate debt securities (one to two year maturity) |
5,113 | — | 5,113 | — | ||||||||||||
| U.S. government and agency securities |
3,545 | — | 3,545 | — | ||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| $ | 192,982 | $ | 129,209 | $ | 63,773 | $ | — | |||||||||
|
|
|
|
|
|
|
|
|
|||||||||
Property and Equipment, net
Property and equipment are recorded at cost, less accumulated depreciation. Depreciation is recorded using the straight-line method over the estimated useful lives of the respective assets, generally three to five years. Leasehold improvements are amortized over the shorter of the lease term or the estimated useful economic lives of the related assets. Expenditures for maintenance and repairs are charged to expense while the costs of significant improvements are capitalized. Upon retirement or sale, the cost of the assets disposed of and the related accumulated depreciation are eliminated from the balance sheets and any related gains or losses are reflected in the consolidated statements of operations.
Long-Lived Assets
The Company reviews the carrying values of its long-lived assets for possible impairment whenever events or changes in circumstances indicate that the carrying amounts of the assets may not be recoverable. Any long-lived assets held for disposal are reported at the lower of their carrying amounts or fair values less costs to sell. The Company has not recorded an impairment in any period since inception.
Deferred Rent
Deferred rent consists of rent escalation payment terms, tenant improvement allowances and other incentives received from landlords related to the Company’s operating leases. Rent escalation represents the difference between actual operating lease payments due and straight-line rent expense, which is recorded by the Company over the term of the lease. Tenant improvement allowances and other incentives are recorded as deferred rent and amortized as a reduction of periodic rent expense, over the term of the applicable lease.
117
Table of Contents
Revenue Recognition
The Company recognizes revenue in accordance with the FASB ASC 605, Revenue Recognition. Accordingly, revenue is recognized for each unit of accounting when all of the following criteria are met:
| • | persuasive evidence of an arrangement exists; |
| • | delivery has occurred or services have been rendered; |
| • | the seller’s price to the buyer is fixed or determinable; and |
| • | collectability is reasonably assured. |
The Company recognizes revenue in accordance with the milestone method of revenue recognition for arrangements involving research or development or other performance obligations whereby a portion or all of the consideration is contingent upon achievement of milestone events. Under these provisions, arrangement consideration contingent upon achievement of a milestone is recognized by the Company in the period the milestone is met when the Company concludes that the milestone is substantive. At the inception of each applicable arrangement, the Company assesses each milestone and the consideration payable upon achievement of each milestone and concludes that the milestone is substantive if all of the following criteria are met: (i) the consideration is commensurate with the Company’s performance or the enhanced value of a delivered item which is a direct result of the Company’s performance to achieve the milestone, (ii) the consideration relates to past performance and there are no refund rights or other penalties related to the consideration based on completion of future performance and (iii) the consideration is reasonable relative to all the deliverables and payment terms within the arrangement. The related consideration for milestones that are considered substantive is recognized in its entirety in the period which the milestone is met.
The milestone method of revenue recognition was applicable to two research agreements executed during 2013 and 2011.
The agreement executed during 2013 includes payments upon the achievement of several development milestones as well as an upfront payment. The Company concluded that the upfront payment of $100 did not represent a substantive milestone. Accordingly, the Company recognized this amount on a straight-line basis from the date when substantive services commenced through the estimated completion of the final milestone. During the year ended December 31, 2015, the Company recognized $250 related to this agreement. During the year ended December 31, 2014, the Company recognized $229 related to this agreement, including $79 of the upfront payment and $150 related to other milestones associated with the agreement. During the year ended December 31, 2013 the Company recognized $21 of the upfront payment and no additional milestones were met according to this research agreement. There are no future milestones to be met under this agreement.
The agreement executed during 2011 includes payments upon the achievement of several development milestones as well as an upfront payment. The Company concluded that the upfront payment of $200 did not represent a substantive milestone. Accordingly, the Company recognized this amount on a straight-line basis from the date when substantive services commenced through the estimated completion of the final milestone. The Company did not recognize revenue under this agreement during the years ended December 31, 2015 and 2014. During the year ended December 31, 2013, the Company recognized $366 related to this agreement, including $66 related to the upfront payment and $300 related to other milestones associated with the agreement. There are no future milestones to be met under this agreement.
Research and Development Expenses
Research and development costs are charged to expense as incurred and include, but are not limited to:
| • | employee-related expenses, including salaries, benefits, travel and stock-based compensation expense; |
118
Table of Contents
| • | expenses incurred under agreements with contract research organizations, contract manufacturing organizations and consultants that conduct clinical trials and preclinical studies; |
| • | the cost of acquiring, developing and manufacturing clinical trial materials; |
| • | facility, depreciation and other expenses, which include direct and allocated expenses for rent and maintenance of facilities, insurance and other supplies; and |
| • | costs associated with preclinical activities and regulatory operations. |
Costs for certain development activities, such as clinical trials, are recognized based on an evaluation of the progress to completion of specific tasks using data such as patient enrollment, clinical site activations, or information provided to the Company by its vendors on their actual costs incurred. Payments for these activities are based on the terms of the individual arrangements, which may differ from the pattern of costs incurred, and are accordingly reflected in the financial statements as prepaid or accrued research and development.
Comprehensive Loss
Comprehensive loss consists of net loss and changes in equity during a period from transactions and other equity and circumstances generated from non-owner sources, and currently consists of net loss, unrealized losses on investments and foreign currency translation adjustments.
Foreign Currency Transactions
The functional currency of the Company’s subsidiary in Germany is the Euro. Foreign currency transaction gains and losses are recorded in the consolidated statement of operations. Net foreign exchange losses of $2 and $27 were recorded in other expense for the years ended December 31, 2015 and 2014, respectively. There were no foreign exchange gains or losses for the year ended December 31, 2013.
Income Taxes
The Company uses the liability method of accounting for income taxes. Under this method, deferred tax assets and liabilities are determined based on the difference between the financial reporting and the tax reporting basis of assets and liabilities and are measured using the enacted tax rates and laws that are expected to be in effect when the differences are expected to reverse. The Company provides a valuation allowance against net deferred tax assets unless, based upon the available evidence, it is more likely than not that the deferred tax assets will be realized. The Company has evaluated available evidence and concluded that the Company may not realize the benefit of its deferred tax assets; therefore a valuation allowance has been established for the full amount of the deferred tax assets. The Company recognizes interest and/or penalties related to income tax matters in income tax expense.
Accounting for Stock-Based Compensation
The Company accounts for its stock-based compensation awards in accordance with FASB ASC Topic 718, Compensation—Stock Compensation (“ASC 718”). ASC 718 requires all stock-based payments to employees, including grants of employee stock options, restricted stock and restricted stock units and modifications to existing stock options, to be recognized in the consolidated statements of operations based on their fair values. The Company uses the Black-Scholes option pricing model to determine the fair value of options granted.
Consistent with the guidance in FASB ASC Topic 505-50, Equity-Based Payments to Non-Employees, the fair value of each non-employee stock option is estimated at the date of grant using the Black-Scholes option pricing model with assumptions generally consistent with those used for employee stock options, with the exception of expected term, which is over the contractual life.
119
Table of Contents
Compensation expense related to awards to employees is recognized on a straight-line basis based on the grant date fair value over the requisite service period of the award, which is generally the vesting term. Stock-based compensation expense for awards granted to non-employees is adjusted as the award vests to reflect the current fair value of such awards, and is recognized using an accelerated attribution model.
Net Loss Per Share
Basic and diluted net loss per common share is calculated by dividing net loss by the weighted-average number of common shares outstanding for the period, without consideration for common stock equivalents. The Company’s potential dilutive shares, stock options, unvested restricted stock and restricted stock units are considered to be common stock equivalents and are only included in the calculation of diluted net loss per share when their effect is dilutive.
The following potentially dilutive securities were excluded from the calculation of diluted net loss per share due to their anti-dilutive effect at December 31, 2015, 2014 and 2013 (in common stock equivalent shares):
| December 31, | ||||||||||||
| 2015 | 2014 | 2013 | ||||||||||
| Outstanding stock options |
4,443,317 | 3,012,923 | 2,410,522 | |||||||||
| Unvested restricted stock |
— | 11,410 | 166,949 | |||||||||
| Unvested restricted stock units |
508,800 | — | — | |||||||||
Recently Issued Accounting Pronouncements
In July 2015, the FASB deferred the effective date for Accounting Standards Updates (“ASU”) No. 2014-09, Revenue from Contracts with Customers (ASU 2014-09), by one year. ASU 2014-09 will supersede the revenue recognition requirements in Revenue Recognition (Topic 605) and requires entities to recognize revenue in a way that depicts the transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled to in exchange for those goods or services. ASU 2014-09 is effective for annual reporting periods beginning after December 15, 2017, including interim periods within that reporting period, which for the Company is January 1, 2018. Early adoption is permitted only for periods after December 15, 2016. The new standard can be applied retrospectively to each prior reporting period presented or retrospectively with the cumulative effect of the change recognized at the date of the initial application in retained earnings. The Company is currently evaluating the potential impact the adoption of ASU 2014-09 will have on its consolidated financial statements and has not yet selected a transition method.
In September 2015, the FASB issued ASU No. 2015-16, Simplifying the Accounting for Measurement-Period Adjustments (ASU 2015-16). The amended guidance requires that an acquirer recognize adjustments to provisional amounts that are identified during the measurement period in the reporting period in which the adjustment amounts are determined. The amendments are effective prospectively for the fiscal years, and the interim reporting periods within those years, beginning on or after December 15, 2015 and early adoption is permitted. The Company does not believe ASU No. 2015-16 will have a material impact on the Company’s financial statements.
In November 2015, the FASB issued authoritative accounting guidance related to the balance sheet classification of deferred taxes. This guidance requires deferred tax liabilities and assets to be classified as noncurrent in a classified statement of financial position. This guidance may be applied on either a prospective or retrospective basis and is effective for annual reporting periods beginning after December 15, 2016, with early adoption permitted. The Company adopted this standard prospectively in the fourth quarter of 2015, and as the Company’s deferred tax assets are fully offset by a valuation allowance, there was no impact to the Company’s financial position or results of operations upon its adoption of this standard.
120
Table of Contents
In January 2016, the FASB issued ASU No. 2016-01, Financial Instruments—Overall (Subtopic 825-10): Recognition and Measurement of Financial Assets and Financial Liabilities (ASU 2016-01). ASU 2016-01 addresses certain aspects of recognition, measurement, presentation, and disclosure of financial instruments. ASU 2016-01 is effective for fiscal years, and interim periods within those years, beginning after December 15, 2017, which for the Company is January 1, 2018. The Company is currently evaluating the impact that the standard will have on its consolidated financial statements.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842): (ASU 2016-02). ASU 2016-02 improves financial reporting around leasing transactions and more closely aligns accounting for leases with the recently issued International Financial Reporting Standard. ASU 2016-02 requires a lessee to recognize assets and liabilities on the balance sheet for operating leases and changes many key definitions, including the definition of a lease. ASU 2016-02 includes a short-term lease exception for leases with a term of 12 months or less, in which a lessee can make an accounting policy election not to recognize lease assets and lease liabilities. Lessees will continue to differentiate between finance leases (previously referred to as capital leases) and operating leases, using classification criteria that are substantially similar to the previous guidance. ASU 2016-02 is effective for fiscal years beginning after December 15, 2018 and interim periods within those fiscal years, with earlier application permitted. The Company is currently evaluating the impact that the standard will have on its consolidated financial statements.
3. Property and Equipment, net
Property and equipment, net consist of the following (in thousands):
| December 31, | ||||||||||
| Estimated Useful Life Years |
2015 | 2014 | ||||||||
| Laboratory equipment |
4 | $ | 538 | $ | 434 | |||||
| Furniture and fixtures |
5 | 322 | 95 | |||||||
| Office and computer equipment |
3 | 360 | 170 | |||||||
| Construction in progress |
— | — | 92 | |||||||
| Leasehold improvements |
Lesser of useful life or lease term | 3,391 | 2,457 | |||||||
|
|
|
|
|
|||||||
| 4,611 | 3,248 | |||||||||
| Less accumulated depreciation and amortization |
(1,128 | ) | (494 | ) | ||||||
|
|
|
|
|
|||||||
| $ | 3,483 | $ | 2,754 | |||||||
|
|
|
|
|
|||||||
Depreciation and amortization expense recorded for the years ended December 31, 2015, 2014, and 2013 were $634, $323, and $144, respectively.
121
Table of Contents
4. Investments
The following table summarizes the Company’s investments as of December 31, 2015 (in thousands):
| Amortized Cost | Gross Unrealized Gains |
Gross Unrealized Loss |
Fair Value | |||||||||||||
| Current: |
||||||||||||||||
| Corporate debt securities |
$ | 86,515 | $ | 4 | $ | (72 | ) | $ | 86,447 | |||||||
| Commercial paper |
29,808 | 20 | — | 29,828 | ||||||||||||
| U.S. government and agency securities |
1,000 | — | — | 1,000 | ||||||||||||
| Non-current: |
||||||||||||||||
| Corporate debt securities (one to two year maturity) |
34,019 | 2 | (143 | ) | 33,878 | |||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| $ | 151,342 | $ | 26 | $ | (215 | ) | $ | 151,153 | ||||||||
|
|
|
|
|
|
|
|
|
|||||||||
The following table summarizes the Company’s investments as of December 31, 2014 (in thousands):
| Amortized Cost | Gross Unrealized Gains |
Gross Unrealized Loss |
Fair Value | |||||||||||||
| Current: |
||||||||||||||||
| Certificates of deposit |
$ | 15,000 | $ | — | $ | — | $ | 15,000 | ||||||||
| Corporate debt securities |
10,144 | 1 | (10 | ) | 10,135 | |||||||||||
| Commercial paper |
29,980 | — | — | 29,980 | ||||||||||||
| Non-current: |
||||||||||||||||
| Corporate debt securities (one to two year maturity) |
5,122 | 1 | (10 | ) | 5,113 | |||||||||||
| U.S. government and agency securities |
3,549 | 1 | (5 | ) | 3,545 | |||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| $ | 63,795 | $ | 3 | $ | (25 | ) | $ | 63,773 | ||||||||
|
|
|
|
|
|
|
|
|
|||||||||
At December 31, 2015 and December 31, 2014, the Company held 69 and 11 debt securities, respectively, that were in an unrealized loss position for less than one year. The aggregate fair value of debt securities in unrealized loss positions at December 31, 2015 and December 31, 2014 was $117,851 and $12,635, respectively. There were no individual securities that were in a significant unrealized loss position or that had been in an unrealized loss position for greater than one year as of December 31, 2015 or December 31, 2014.
The Company reviews investments for other-than-temporary impairment whenever the fair value of an investment is less than the amortized cost and evidence indicates that an investment’s carrying amount is not recoverable within a reasonable period of time. Other-than-temporary impairments of investments are recognized in the consolidated statements of operations if the Company has experienced a credit loss or has the intent to sell the investment or if it is more likely than not that the Company will be required to sell the investment before recovery of the amortized cost basis. Evidence considered in this assessment includes reasons for the impairment, compliance with the Company’s investment policy, the severity and the duration of the impairment and changes in value subsequent to the end of the period.
122
Table of Contents
5. Accrued Liabilities
Accrued expenses consist of the following (in thousands):
| December 31, | ||||||||
| 2015 | 2014 | |||||||
| Research and development costs |
$ | 8,007 | $ | 3,624 | ||||
| Payroll and employee-related costs |
2,445 | 1,568 | ||||||
| Professional fees |
270 | 324 | ||||||
| Other |
301 | 309 | ||||||
|
|
|
|
|
|||||
| $ | 11,023 | $ | 5,825 | |||||
|
|
|
|
|
|||||
6. Related Party Transactions
The Company incurred expenses for consulting and contract research services with certain related parties, including a family member of management, a board member and a private diagnostics company, of which three of the Company’s Board of Directors, including the Company’s CEO, were also members of the private company’s Board of Directors. The Company paid consulting and histopathology services of $456, $664 and $452 for the years ended December 31, 2015, 2014, and 2013, respectively. At December 31, 2015 and 2014 there was $55 and $94, respectively, included in accounts payable and accrued expenses due to related parties.
7. Stockholders’ Equity
Controlled Equity Offering Sales Agreement
On December 7, 2015, the Company entered into a Controlled Equity Offering Sales Agreement (the “Agreement”), with Cantor Fitzgerald & Co., as sales agent (“Cantor”), pursuant to which the Company may issue and sell, from time to time, through Cantor shares of the Company’s common stock, up to an aggregate offering price of $50.0 million (the “Shares”).
Under the Agreement, Cantor may sell the Shares by methods deemed to be an “at-the-market” offering as defined in Rule 415 promulgated under the Securities Act of 1933, as amended (the “Securities Act”), including sales made directly on The NASDAQ Global Select Market, on any other existing trading market for the Shares or to or through a market maker. In addition, under the Agreement, Cantor may sell the Shares by any other method permitted by law, including in privately negotiated transactions.
The Company is not obligated to make any sales of the Shares under the Agreement. The Company or Cantor may suspend or terminate the offering of Shares upon notice to the other party and subject to other conditions. The Company will pay Cantor a commission of up to 3.0% of the gross proceeds from the sale of the Shares pursuant to the Agreement and has agreed to provide Cantor with customary indemnification and contribution rights.
As of December 31, 2015, the Company had sold an aggregate of 121,314 shares of common stock for net proceeds of approximately $1,502 under the Agreement.
Common Stock
In January 2015, the Company completed an underwritten offering of 2,950,000 shares of its common stock at a public offering price of $33.00 per share. The net proceeds received by the Company were $90,830 after deducting the underwriting discount and offering expenses payable by the Company.
123
Table of Contents
In July 2014, the Company completed a public offering of its common stock, which resulted in the sale of 2,447,247 shares of its common stock at a public offering price of $42.50 per share. Also, in July 2014, the Company issued 397,087 shares of its common stock upon exercise by the underwriters of their option to purchase additional shares. The Company received net proceeds of approximately $112,837, after deducting underwriting discounts, commissions and expenses payable by the Company of $794.
In November 2013, the Company closed an IPO of its common stock, which resulted in the sale of 6,800,000 shares of its common stock at a public offering price of $16.00 per share. In December 2013, the Company issued 1,020,000 shares of common stock upon the exercise by the underwriters of their option to purchase additional shares at the public offering price. The Company received net proceeds from the IPO of approximately $113,155, after deducting underwriting discounts and expenses payable by the Company.
In connection with the closing of the IPO, all of the Company’s outstanding convertible preferred stock automatically converted to common stock in November 2013, resulting in an additional 19,114,241 shares of common stock of the Company becoming outstanding. Upon the closing of its IPO, the Company had 5,000,000 shares of authorized preferred stock. As of December 31, 2015, 2014 and 2013, the Company did not have any preferred stock issued or outstanding.
8. Commitments and Contingencies
Operating Leases
In March 2014, the Company entered into an operating lease for approximately 29,933 square feet of office and research space in Newton, Massachusetts. The Company uses the leased premises as its corporate headquarters and for research and development purposes. The lease was amended on December 31, 2014 by extending the lease term of the lease from November 30, 2021 to approximately September 30, 2022. The Amendment provided for the expansion of the premises leased by the Company by approximately 16,234 square feet. The Company may extend the lease term for one additional five year period. The Company has agreed to pay pro rata increases in operating expenses and property taxes. The Company is recording rent expense on a straight-line basis through the end of the lease term, inclusive of the period in which there are no scheduled rent payments. The Company has recorded deferred rent on the consolidated balance sheet at December 31, 2015 and December 31, 2014, accordingly. The lease provides the Company with an allowance for improvements of $1,616 of which $1,616 was incurred through December 31, 2015 and was deemed normal tenant improvements. Therefore, the amounts were recorded as a leasehold improvement and deferred rent, and will be recorded as a reduction to rent expense ratably over the lease term. The Company has provided a security deposit in the form of a cash-collateralized letter of credit in the amount of $400, which amount may be reduced to $200 in January 2018. The amount is classified as restricted cash on the consolidated balance sheet.
In November 2014, the Company signed a five-year operating lease agreement in Munich, Germany for approximately 3,681 square feet of office space. The lease is for the period from February 2015 through January 2020. Pursuant to the lease agreement, the Company is obligated to make aggregate rent payments of €374, (approximately $409) through January 31, 2020. The Company is recording rent expense on a straight-line basis through the end of the lease term, inclusive of the period in which there are no scheduled rent payments.
124
Table of Contents
As of December 31, 2015, the minimum future rent payments under the lease agreements are as follows (in thousands):
| 2016 |
$ | 1,326 | ||
| 2017 |
1,400 | |||
| 2018 |
1,423 | |||
| 2019 |
1,447 | |||
| 2020 |
1,389 | |||
| Thereafter |
2,498 | |||
|
|
|
|||
| Total future minimum lease payments |
$ | 9,483 | ||
|
|
|
The Company recorded rent expense totaling $1,033, $520 and $174 for the years ended December 31, 2015, 2014, and 2013, respectively.
Research Agreements
In July 2011 and September 2013, the Company entered into research agreements in which the Company received payments upon the achievement of certain milestones. The agreements require the Company to pay royalties on product sales, up to a predetermined maximum. The Company must also pay a royalty on any sublicense income, up to a predetermined maximum. No royalties or sublicense payments have been made to date.
Litigation
From time to time the Company may face legal claims or actions in the normal course of business. The Company is not currently a party to any litigation and, accordingly, does not have amounts recorded for any litigation-related matters.
9. Stock-based Compensation
During 2010, the Company established the 2010 Stock Incentive Plan (the “Plan” or the “2010 Plan”). Under the terms of the Plan, options and other equity interests may be granted to employees, officers, directors, consultants and advisors of the Company. The exercise price of each stock option shall be the fair market value as determined in good faith by the Board of Directors (the Board) at the time each option is granted. The Company has granted service-based options under the Plan. Service-based option grants under the Plan generally vest as follows: 25% of the shares vest one calendar year from the vesting start date, 2.083% of the shares vest on the first day of each month thereafter. The options granted under the Plan generally expire in 10 years from the date of grant.
In October 2013, the Company’s board of directors adopted and the Company’s stockholders approved the 2013 Stock Incentive Plan (the “2013 Plan”). The 2013 Plan became effective immediately prior to the closing of the IPO and provides for the grant of incentive stock options, nonstatutory stock options, stock appreciation rights, restricted stock awards, restricted stock unit awards and other stock-based awards. The number of shares of common stock reserved for issuance under the 2013 Plan is equal to the sum of (1) 969,696 shares plus (2) the number of shares (up to 2,126,377 shares) equal to the sum of the number of shares of common stock then available for issuance under the 2010 Plan and the number of shares of common stock subject to outstanding awards under the 2010 Plan that expire, terminate or are otherwise surrendered, cancelled, forfeited or repurchased by the Company at their original issuance price pursuant to a contractual repurchase right plus (3) an annual increase, to be added on the first day of each fiscal year, beginning with the fiscal year ending December 31, 2014 and continuing until, and including, the fiscal year ending December 31, 2023, equal to the lesser of (A) 1,939,393 shares of common stock, (B) 4% of the number of shares of common stock outstanding
125
Table of Contents
on the first day of such fiscal year, and (C) an amount determined by the Board. The Company will grant no further stock options or other awards under the 2010 Plan.
The Company amended the 2013 Plan in March 2015 to increase the number of shares available for issuance under the 2013 Plan by 1,308,431 shares of common stock. As of December 31, 2015, the Company had 429,180 shares available for issuance.
In connection with all share-based payment awards, total stock-based compensation expense recognized was as follows (in thousands):
| Year Ended December 31, | ||||||||||||
| 2015 | 2014 | 2013 | ||||||||||
| Research and development |
$ | 8,368 | $ | 7,078 | $ | 2,567 | ||||||
| General and administrative |
8,689 | 7,162 | 1,218 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total |
$ | 17,057 | $ | 14,240 | $ | 3,785 | ||||||
|
|
|
|
|
|
|
|||||||
Stock Options
Total expense related to employee and non-employee stock options for the years ended December 31, 2015, 2014 and 2013 was $16,094, $13,962, and $3,020, respectively.
The following table summarizes stock option activity for employees and nonemployees:
| Shares | Weighted- Average Exercise Price |
Weighted- Average Remaining Contractual Term (years) |
Aggregate Intrinsic Value |
|||||||||||||
| Options outstanding at December 31, 2014 |
3,012,923 | $ | 16.65 | 8.7 | $ | 64,659 | ||||||||||
| Granted |
1,795,800 | 26.00 | ||||||||||||||
| Exercised |
(57,240 | ) | 4.62 | |||||||||||||
| Forfeited |
(308,166 | ) | 26.42 | |||||||||||||
|
|
|
|||||||||||||||
| Options outstanding at December 31, 2015 |
4,443,317 | $ | 19.91 | 8.2 | $ | 15,598 | ||||||||||
|
|
|
|||||||||||||||
| Options vested or expected to vest at December 31, 2015(1) |
4,335,443 | $ | 19.76 | 8.2 | $ | 15,532 | ||||||||||
|
|
|
|||||||||||||||
| Options exercisable at December 31, 2015 |
1,617,948 | $ | 12.95 | 7.4 | $ | 10,871 | ||||||||||
|
|
|
|||||||||||||||
| (1) | This represents the number of vested options, plus the number of unvested options that the Company estimated would vest, based on the unvested options as of the year ended December 31, 2015 as adjusted for the estimated forfeiture rate. |
The total intrinsic value of stock options exercised for the years ended December 31, 2015, 2014 and 2013 was $1,248, $3,716, and $239, respectively.
126
Table of Contents
The fair value of each stock option granted to employees is estimated on the date of grant and for non-employees on each reporting date and upon vesting using the Black-Scholes option-pricing model. The following table summarizes the assumptions used in calculating the fair value of the awards:
| Years Ended December 31, | ||||||
| 2015 | 2014 | 2013 | ||||
| Volatility |
79%-88% | 84%-95% | 85%-93% | |||
| Expected term (in years) |
5.0-9.9 | 5.5-9.9 | 6.25-10 | |||
| Risk-free interest rate |
1.45%-2.33% | 1.73%-2.15% | 1.07%-3.01% | |||
| Dividend |
0% | 0% | 0% | |||
The Company uses the simplified method as prescribed by the Securities and Exchange Commission Staff Accounting Bulletin No. 107, Share-Based Payment, to calculate the expected term as it does not have sufficient historical exercise data to provide a reasonable basis upon which to estimate the expected term for options granted to employees and utilizes the contractual term for options granted to non-employees. The expected term is applied to the stock option grant group as a whole, as the Company does not expect substantially different exercise or post-vesting termination behavior among its employee population. The expected volatility is based on the historical volatility of a representative group of companies with similar characteristics to the Company, including early stage of product development and therapeutic focus. For these analyses, the Company selects companies with comparable characteristics to theirs including enterprise value, risk profiles, position within the industry, and with historical share price information sufficient to meet the expected term of the options. The risk-free interest rate is based on a treasury instrument whose term is consistent with the expected term of the stock options. Management estimates expected forfeitures based on historical data from the Company and recognizes compensation costs only for those equity awards expected to vest.
Using the Black-Scholes option-pricing model, the weighted-average grant date fair values of options granted during the years ended December 31, 2015, 2014 and 2013 was $18.67, $29.71, and $11.09 per share, respectively.
At December 31, 2015, the total unrecognized compensation related to unvested employee and non-employee stock option awards granted under the 2010 Plan and 2013 Plan, including estimated forfeitures, was $41,275, which the Company expects to recognize over a weighted-average period of approximately 2.5 years.
In 2014 certain individuals changed status from employees to non-employees. The outstanding stock option awards for these individuals continued to vest under the original vesting terms of the awards as the individuals continued to provide service to the Company as consultants. In addition, in August 2014, the Company modified a stock option grant for one of these individuals to accelerate vesting of a stock option award in connection with a separation agreement. The Company recorded stock-based compensation expense of $1,866 associated with these awards. As of December 31, 2015, there was no unrecognized compensation expense related to these awards as the individuals are no longer providing service to the Company.
127
Table of Contents
Restricted Stock
To date, the Company has granted 1,958,210 shares of restricted stock outside of the 2010 Plan and the 2013 Plan and 45,454 shares of restricted stock under the 2010 Plan. The following table summarizes the status of the Company’s unvested restricted common shares:
| Number of Shares |
Weighted-Average Grant Date Fair Value |
|||||||
| Unvested at December 31, 2014 |
4,262 | $ | 0.26 | |||||
| Granted |
— | — | ||||||
| Cancelled |
— | — | ||||||
| Vested |
(4,262 | ) | 0.26 | |||||
|
|
|
|
|
|||||
| Unvested at December 31, 2015 |
— | $ | — | |||||
|
|
|
|
|
|||||
The total expense related to employee and non-employee restricted stock for the years ended December 31, 2015, 2014 and 2013 was $111, $193 and $765, respectively.
As of December 31, 2015, there was no unrecognized compensation cost related to employee and non-employee unvested restricted stock.
Restricted Stock Unit
A restricted stock unit (“RSU”) is a stock award that entitles the holder to receive shares of the Company’s common stock as the award vests. The fair value of each RSU is based on the closing price of the Company’s stock on the date of grant. In November 2015, the Company granted RSUs with service conditions (service RSUs) that vest in two equal annual installments provided that the employee remains employed with the Company. The following is a summary of RSU activity for the 2013 Plan for the year ended December 31, 2015:
| Number of Shares Underlying RSUs |
Weighted-Average Grant Date Fair Value |
|||||||
| Unvested at December 31, 2014 |
— | $ | — | |||||
| Granted |
511,800 | 17.91 | ||||||
| Forfeited |
(3,000 | ) | 17.91 | |||||
| Vested |
— | — | ||||||
|
|
|
|
|
|||||
| Unvested at December 31, 2015 |
508,800 | $ | 17.91 | |||||
|
|
|
|
|
|||||
The total expense related to RSUs for the year ended December 31, 2015 was $660.
As of December 31, 2015, $7,734 of unrecognized compensation costs related to unvested service RSUs are expected to be recognized over a weighted average period of 1.8 years.
Employee Stock Purchase Plan
The Company has an Employee Stock Purchase Plan (“ESPP”) that permits eligible employees to enroll in a twelve-month offering period comprising two six-month purchase periods. Participants may purchase shares of the Company’s common stock, through payroll deductions, at a price equal to 85% of the fair market value of the common stock on the first day of the applicable six-month offering period, or the last day of the applicable six-month purchase period, whichever is lower. Purchase dates under the ESPP occur on or about May 1 and November 1of each year. In 2013, the Company’s shareholders approved an increase in the number of shares of common stock authorized for issuance pursuant to the ESPP to 242,424 shares of common stock.
128
Table of Contents
During the years ended December 31, 2015 and 2014, $352 and $141, respectively, was withheld from employees, on an after-tax basis, in order to purchase 25,421 and 6,202 shares of the Company’s common stock, respectively. For the years ended December 31, 2015 and 2014, the Company recorded stock-based compensation expense of $192 and $85, respectively. As of December 31, 2015, 537,908 shares of Company’s common stock remain available for issuance under the ESPP. As of December 31, 2015, there was $93 of total unrecognized stock-based compensation expense related to the ESPP. The expense is expected to be recognized over a period of four months.
The fair value of the option component of the shares purchased under the ESPP was estimated using the Black-Scholes option-pricing model with the following weighted-average assumptions:
| Years Ended December 31, | ||||
| 2015 | 2014 | |||
| Volatility |
69.5%-95.5% | 75% | ||
| Expected term (in years) |
0.5 | 0.5 | ||
| Risk-free interest rate |
0.05%-0.08% | 0.05% | ||
| Dividend |
0% | 0% | ||
10. 401(k) Plan
The Company has a 401(k) retirement and profit-sharing plan (the “401(k) Plan”) covering all qualified employees. The 401(k) Plan allows each participant to contribute a portion of their base wages up to an amount not to exceed an annual statutory maximum. Effective January 1, 2011, the Company adopted a Safe Harbor Plan that provides a Company match up to 4% of salary. The Company contributed a match of $366, $197 and $91 to the 401(k) Plan for the years ended December 31, 2015, 2014 and 2013, respectively.
11. Income Taxes
The Company provides for income taxes under ASC Topic 740, Accounting for Income Taxes. Under ASC Topic 740, the liability method is used in accounting for income taxes. Under this method, deferred tax assets and liabilities are determined based on differences between financial reporting and tax bases of assets and liabilities, and are measured using the enacted tax rates and laws that will be in effect when the differences are expected to reverse.
For the year ended December 31, 2015, the Company recorded income tax expense of $96 for its operations in Germany, and for the year ended December 31 2014, the Company did not record a current or deferred income tax expense or benefit.
The components of income (loss) before income taxes were as follows:
| Year Ended December 31, |
||||||||||||
| 2015 | 2014 | 2013 | ||||||||||
| Foreign |
$ | (21,409 | ) | $ | (2,887 | ) | $ | (10,922 | ) | |||
| U.S. |
(96,676 | ) | (72,890 | ) | (23,025 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Totals |
$ | (118,085 | ) | $ | (75,777 | ) | $ | (33,947 | ) | |||
|
|
|
|
|
|
|
|||||||
129
Table of Contents
Deferred taxes are recognized for temporary differences between the basis of assets and liabilities for financial statement and income tax purposes. The significant components of the Company’s deferred tax assets are comprised of the following:
| Year Ended December 31, |
||||||||
| 2015 | 2014 | |||||||
| Deferred tax assets: |
||||||||
| U.S. and state net operating loss carryforwards |
$ | 63,561 | $ | 39,970 | ||||
| Stock-based compensation |
11,574 | 6,405 | ||||||
| Accruals and other temporary differences |
2,194 | 1,225 | ||||||
| Research and development credits |
21,590 | 4,161 | ||||||
| Capitalized research and development |
3,883 | 4,505 | ||||||
|
|
|
|
|
|||||
| Total deferred tax assets |
102,802 | 56,266 | ||||||
| Less valuation allowance |
(102,802 | ) | (56,266 | ) | ||||
|
|
|
|
|
|||||
| Net deferred tax assets |
$ | — | $ | — | ||||
|
|
|
|
|
|||||
The Company has evaluated the positive and negative evidence bearing upon the realizability of its deferred tax assets. Based on the Company’s history of operating losses, the Company has concluded that it is more likely than not that the benefit of its deferred tax assets will not be realized. Accordingly, the Company has provided a full valuation allowance for deferred tax assets as of December 31, 2015 and 2014. The valuation allowance increased approximately $46,536 and $31,170 during the years ended December 31, 2015 and 2014, respectively, due primarily to the generation of net operating losses during the periods then ended.
In November of 2015, the FASB released Accounting Standards Update (“ASU”) No. 2015-17, Balance Sheet Classification of Deferred Taxes (“the Update”). The Board issued ASU 2015-17 as part of the Simplification Initiative, allowing for all deferred income tax assets and liabilities to be presented as noncurrent in a classified statement of financial position. The Update permits early application of the rules to an entity’s statement of financial position on a prospective or retrospective basis. The Company will prospectively apply the rules under ASU 2015-17 and is therefore required to disclose 1) the nature and reason for the change in accounting principle and 2) a statement that prior periods were not retrospectively adjusted.
| 1) | The Company has elected to early adopt and prospectively apply the rules of ASU 2015-17 to its statement of financial position. The reason for this change in accounting principle is to allow the Company to benefit from the simplified presentation of deferred income taxes and to conform to the FASB’s initiative to improve generally accepted accounting principles for which costs and complexity can be reduced. |
| 2) | Financial statement users are to be made aware the prior period statement of financial position has not been retrospectively adjusted for the Company’s early adoption of the Update. |
130
Table of Contents
A reconciliation of income tax expense computed at the statutory federal income tax rate to income taxes as reflected in the financial statements is as follows:
| Year Ended December 31, |
||||||||||||
| 2015 | 2014 | 2013 | ||||||||||
| Federal income tax expense at statutory rate |
34.0 | % | 34.0 | % | 34.0 | % | ||||||
| State income tax, net of federal benefit |
3.5 | % | 4.9 | % | 4.9 | % | ||||||
| Permanent differences |
(5.1 | )% | (0.7 | )% | 0.0 | % | ||||||
| Research and development credit |
12.2 | % | 1.4 | % | 3.9 | % | ||||||
| Foreign rate differential |
(6.3 | )% | (1.3 | )% | (2.9 | )% | ||||||
| Other |
1.0 | % | 2.8 | % | (0.8 | )% | ||||||
| Change in valuation allowance |
(39.4 | )% | (41.1 | )% | (39.1 | )% | ||||||
|
|
|
|
|
|
|
|||||||
| Effective income tax rate |
(0.1 | )% | 0.0 | % | 0.0 | % | ||||||
|
|
|
|
|
|
|
|||||||
As of December 31, 2015 and 2014, the Company had U.S. federal net operating loss carryforwards of approximately $166,680 and $105,628, respectively, which may be available to offset future income tax liabilities and expire at various dates through 2035. As of December 31, 2015 and 2014, the Company also had U.S. state net operating loss carryforwards of approximately $164,572 and $104,259, respectively, which may be available to offset future income tax liabilities and expire at various dates through 2035. Included in the U.S. federal and state net operating loss carryforwards is a deduction for option exercises of $4,600 and $3,824 as of December 31, 2015 and 2014, respectively.
As of December 31, 2014, the Company had liquidated its Canadian subsidiary resulting in the loss of its net operating loss carryforwards there.
As of December 31, 2015 and 2014, the Company had federal research and development tax credit carryforwards of approximately $19,988 and $3,042, respectively, available to reduce future tax liabilities which expire at various dates through 2035. As of December 31, 2015 and 2014, the Company had state research and development tax credit carryforwards of approximately $2,428 and $1,695, respectively, available to reduce future tax liabilities which expire at various dates through 2030.
Under the provisions of the Internal Revenue Code, the net operating loss and tax credit carryforwards are subject to review and possible adjustment by the Internal Revenue Service and state tax authorities. Net operating loss and tax credit carryforwards may become subject to an annual limitation in the event of certain cumulative changes in the ownership interest of significant shareholders over a three-year period in excess of 50 percent, as defined under Sections 382 and 383 of the Internal Revenue Code, respectively, as well as similar state provisions. This could limit the amount of tax attributes that can be utilized annually to offset future taxable income or tax liabilities. The amount of the annual limitation is determined based on the value of the Company immediately prior to the ownership change. Subsequent ownership changes may further affect the limitation in future years. The Company has completed several financings since its inception which may have resulted in a change in control as defined by Sections 382 and 383 of the Internal Revenue Code, or could result in a change in control in the future.
The Company will recognize interest and penalties related to uncertain tax positions in income tax expense. As of December 31, 2015 and 2014, the Company had no accrued interest or penalties related to uncertain tax positions and no such amounts have been recognized in the Company’s statements of operations and comprehensive loss.
For all years through December 31, 2015, the Company generated research credits but has not conducted a study to document the qualified activities. This study may result in an adjustment to the Company’s research and development credit carryforwards; however, until a study is completed and any adjustment is known, no amounts are being presented as an uncertain tax position for these years. A full valuation allowance has been provided
131
Table of Contents
against the Company’s research and development credits and, if an adjustment is required, this adjustment would be offset by an adjustment to the deferred tax asset established for the research and development credit carryforwards and the valuation allowance.
The Company or one of its subsidiaries files income tax returns in the United States, and various state and foreign jurisdictions. The federal, state and foreign income tax returns are generally subject to tax examinations for the tax years ended December 31, 2012 through December 31, 2015. To the extent the Company has tax attribute carryforwards, the tax years in which the attribute was generated may still be adjusted upon examination by the Internal Revenue Service, state or foreign tax authorities to the extent utilized in a future period.
12. Selected Quarterly Financial Information (Unaudited)
The following table summarizes the unaudited quarterly financial data for the last two fiscal years (in thousands).
| Year Ended December 31, 2015 |
First Quarter |
Second Quarter |
Third Quarter |
Fourth Quarter |
||||||||||||
| Contract and grant revenue |
$ | — | $ | 150 | $ | 75 | $ | 25 | ||||||||
| Total operating expenses |
$ | 26,150 | $ | 33,163 | $ | 30,685 | $ | 29,328 | ||||||||
| Loss from operations |
$ | (26,150 | ) | $ | (33,013 | ) | $ | (30,610 | ) | $ | (29,303 | ) | ||||
| Total other income (expense) |
$ | 83 | $ | 318 | $ | 237 | $ | 257 | ||||||||
| Net loss |
$ | (26,067 | ) | $ | (32,695 | ) | $ | (30,373 | ) | $ | (29,046 | ) | ||||
| Net loss per share applicable to common stockholders, basic and diluted |
$ | (0.74 | ) | $ | (0.92 | ) | $ | (0.85 | ) | $ | (0.81 | ) | ||||
| Year Ended December 31, 2014 |
First Quarter |
Second Quarter |
Third Quarter |
Fourth Quarter |
||||||||||||
| Contract and grant revenue |
$ | 171 | $ | 21 | $ | 21 | $ | 16 | ||||||||
| Total operating expenses |
$ | 13,883 | $ | 16,469 | $ | 19,765 | $ | 25,958 | ||||||||
| Loss from operations |
$ | (13,712 | ) | $ | (16,448 | ) | $ | (19,744 | ) | $ | (25,942 | ) | ||||
| Total other income (expense) |
$ | 18 | $ | 17 | $ | 20 | $ | 14 | ||||||||
| Net loss |
$ | (13,694 | ) | $ | (16,431 | ) | $ | (19,724 | ) | $ | (25,928 | ) | ||||
| Net loss per share applicable to common stockholders, basic and diluted |
$ | (0.46 | ) | $ | (0.55 | ) | $ | (0.61 | ) | $ | (0.79 | ) | ||||
132
Table of Contents
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| KARYOPHARM THERAPEUTICS INC. | ||||||
| Date: March 15, 2016 | By: | /s/ Michael G. Kauffman | ||||
| Michael G. Kauffman, M.D., Ph.D. Chief Executive Officer and Director (Principal Executive Officer) | ||||||
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| Signature | Title | Date | ||
| /s/ Michael G. Kauffman |
Chief Executive Officer and Director | March 15, 2016 | ||
| Michael G. Kauffman, M.D., Ph.D. | (Principal Executive Officer) | |||
| /s/ Justin A. Renz |
Executive Vice President & Chief | March 15, 2016 | ||
| Justin A. Renz |
Financial Officer (Principal Financial and Accounting Officer) |
|||
| /s/ Garen G. Bohlin |
Director | March 15, 2016 | ||
| Garen G. Bohlin | ||||
| /s/ Mikael Dolsten |
Director | March 15, 2016 | ||
| Mikael Dolsten, M.D., Ph.D. | ||||
| /s/ J. Scott Garland |
Director | March 15, 2016 | ||
| J. Scott Garland | ||||
| /s/ Barry E. Greene |
Director | March 15, 2016 | ||
| Barry E. Greene | ||||
| /s/ Deepa R. Pakianathan |
Director | March 15, 2016 | ||
| Deepa R. Pakianathan, Ph.D. | ||||
| /s/ Mansoor Raza Mirza |
Director | March 15, 2016 | ||
| Mansoor Raza Mirza, M.D. | ||||
| /s/ Kenneth E. Weg |
Director | March 15, 2016 | ||
| Kenneth E. Weg | ||||
133
Table of Contents
EXHIBIT INDEX
| Exhibit Number |
Description of Exhibit | |
| Articles of Incorporation and Bylaws | ||
| 3.1 | Restated Certificate of Incorporation of the Registrant (incorporated by reference to Exhibit 3.1 to the Registrant’s Current Report on Form 8-K (File No. 001-36167) filed with the Commission on November 18, 2013) | |
| 3.2 | Amended and Restated By-Laws of the Registrant (incorporated by reference to Exhibit 3.2 to the Registrant’s Current Report on Form 8-K (File No. 001-36167) filed with the Commission on November 18, 2013) | |
| Instruments Defining the Rights of Security Holders, Including Indentures | ||
| 4.1 | Specimen Stock Certificate evidencing the shares of common stock (incorporated by reference to Exhibit 4.1 to the Registrant’s Amendment No. 1 to Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 28, 2013) | |
| 4.2 | Third Amended and Restated Investors’ Rights Agreement dated as of July 26, 2013 (incorporated by reference to Exhibit 4.2 to the Registrant’s Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 4, 2013) | |
| Material Contracts—Management Contracts and Compensatory Plans | ||
| 10.1 | 2010 Stock Incentive Plan (incorporated by reference to Exhibit 10.1 to the Registrant’s Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 4, 2013) | |
| 10.2 | Forms of Non-Qualified Stock Option Agreement under 2010 Stock Incentive Plan (incorporated by reference to Exhibit 10.2 to the Registrant’s Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 4, 2013) | |
| 10.3 | 2013 Stock Incentive Plan (incorporated by reference to Exhibit 10.3 to the Registrant’s Amendment No. 1 to Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 28, 2013) | |
| 10.4 | Form of Incentive Stock Option Agreement under 2013 Stock Incentive Plan (incorporated by reference to Exhibit 10.4 to the Registrant’s Amendment No. 1 to Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 28, 2013) | |
| 10.5 | Form of Nonstatutory Stock Option Agreement under 2013 Stock Incentive Plan (incorporated by reference to Exhibit 10.5 to the Registrant’s Amendment No. 1 to Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 28, 2013) | |
| 10.6 | Form of Restricted Stock Unit Agreement under the 2013 Stock Incentive Plan (incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q (File No. 001-36167) filed with the Commission on November 9, 2015) | |
| 10.7 | 2013 Employee Stock Purchase Plan (incorporated by reference to Exhibit 10.6 to the Registrant’s Amendment No. 1 to Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 28, 2013) | |
| 10.8 | Consulting Agreement, dated as of September 1, 2012, between the Registrant and Mirza Consulting (incorporated by reference to Exhibit 10.11 to the Registrant’s Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 4, 2013) | |
134
Table of Contents
| Exhibit Number |
Description of Exhibit | |
| 10.9 | Form of Indemnification Agreement between the Registrant and each of its Directors (incorporated by reference to Exhibit 10.12 to the Registrant’s Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 4, 2013) | |
| 10.10 | Managing Director Agreement, dated October 15, 2014, by and between Karyopharm Europe GmbH and Ran Frenkel (incorporated by reference to Exhibit 10.16 to the Registrant’s Annual Report on Form 10-K (File No. 001-36167) filed with the Commission on March 13, 2015) | |
| 10.11 | Letter Agreement, dated October 15, 2014, by and between Karyopharm Therapeutics Inc. and Ran Frenkel (incorporated by reference to Exhibit 10.17 to the Registrant’s Annual Report on Form 10-K (File No. 001-36167) filed with the Commission on March 13, 2015) | |
| 10.12 | Amended and Restated Letter Agreement, dated as of January 23, 2015, between the Registrant and Michael Kauffman, M.D., Ph.D. (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K (File No. 001-36167) filed with the Commission on January 23, 2015) | |
| 10.13 | Amended and Restated Letter Agreement, dated as of January 23, 2015, between the Registrant and Sharon Shacham, Ph.D., M.B.A. (incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K (File No. 001-36167) filed with the Commission on January 23, 2015) | |
| 10.14 | Amended and Restated Letter Agreement, dated as of January 23, 2015, between the Registrant and Justin Renz (incorporated by reference to Exhibit 10.3 to the Registrant’s Current Report on Form 8-K filed with the Commission on January 23, 2015) | |
| 10.15 | Amendment to Managing Director Agreement, dated February 15, 2015, by and between Karyopharm Europe GmbH and Ran Frenkel (incorporated by reference to Exhibit 10.22 to the Registrant’s Annual Report on Form 10-K (File No. 001-36167) filed with the Commission on March 13, 2015) | |
| 10.16 | Offer Letter, dated June 7, 2015, between Karyopharm Therapeutics Inc. and Ran Frenkel (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K (File No. 001-36167) filed with the Commission on June 10, 2015) | |
| 10.17 | Amended and Restated Letter Agreement, dated as of September 18, 2015, between the Registrant and Christopher B. Primiano (incorporated by reference to Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q (File No. 001-36167) filed with the Commission on November 9, 2015) | |
| 10.18 | Amendment to Managing Director Agreement, dated October 16, 2015, between Karyopharm Europe GmbH and Ran Frenkel (incorporated by reference to Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q (File No. 001-36167) filed with the Commission on November 9, 2015) | |
| 10.19 | Amendment to Consulting Agreement, dated September 1, 2015, between the Registrant and Mirza Consulting (incorporated by reference to Exhibit 10.4 to the Registrant’s Quarterly Report on Form 10-Q (File No. 001-36167) filed with the Commission on November 9, 2015) | |
| Material Contracts—Leases | ||
| 10.20 | Office Lease Agreement between NS Wells Acquisition LLC and the Registrant, dated March 27, 2014 (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K (File No. 001-36167) filed with the Commission on April 1, 2014) | |
135
Table of Contents
| Exhibit Number |
Description of Exhibit | |
| 10.21 | First Amendment to Lease, dated December 31, 2014, by and between the Registrant and NS Wells Acquisition LLC (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K (File No. 001-36167) filed with the Commission on January 5, 2015) | |
| 10.22 | Second Amendment to Lease, dated October 22, 2015, by and between the Registrant and NS Wells Acquisition LLC (incorporated by reference to Exhibit 10.5 to the Registrant’s Quarterly Report on Form 10-Q (File No. 001-36167) filed with the Commission on November 9, 2015) | |
| Material Contracts—Research Agreements | ||
| 10.23† | Research Agreement, dated as of July 18, 2011, between the Registrant and the Multiple Myeloma Research Foundation, Inc. (incorporated by reference to Exhibit 10.14 to the Registrant’s Registration Statement on Form S-1 (File No. 333-191584) filed with the Commission on October 4, 2013) | |
| Material Contracts—Other Agreements | ||
| 10.24 | Controlled Equity OfferingSM Sales Agreement, dated December 7, 2015, by and between Karyopharm Therapeutics Inc. and Cantor Fitzgerald & Co. (incorporated by reference to Exhibit 1.1 to the Registrant’s Current Report on Form 8-K (File No. 001-36167) filed with the Commission on December 8, 2015) | |
| Additional Exhibits | ||
| 12.1 | Statements Regarding Calculation of Consolidated Ratios of Earnings to Fixed Charges and Ratios of Earnings to Combined Fixed Charges and Preferred Stock Dividends | |
| 21.1 | Subsidiaries of the Registrant | |
| 23.1 | Consent of Ernst & Young LLP (Independent registered public accounting firm for the Company) | |
| 23.2 | Consent of RSM US LLP (Independent registered public accounting firm for the Company) | |
| 31.1 | Certification of Chief Executive Officer pursuant to Rules 13a-14(a) or 15d-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |
| 31.2 | Certification of Executive Vice President and Chief Financial Officer pursuant to Rules 13a-14(a) or 15d-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |
| 32.1 | Certifications pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of The Sarbanes-Oxley Act of 2002, by Michael G. Kauffman, M.D., Ph.D., Chief Executive Officer of the Registrant, and Justin A. Renz, Executive Vice President and Chief Financial Officer of the Registrant | |
| 101.INS XBRL | Instance Document | |
| 101.SCH XBRL | Schema Document | |
| 101.CAL XBRL | Calculation Linkbase Document | |
| 101.LAB XBRL | Labels Linkbase Document | |
| 101.PRE XBRL | Presentation Linkbase Document | |
| 101.DEF XBRL | Definition Linkbase Document | |
| † | Confidential treatment has been granted as to portions of the exhibit. |
136