Table of Contents
UNITED STATES SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
| For the fiscal year ended December 31, 2005, or |
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
| For the transition period from to |
Commission File No.: 001-16753
AMN HEALTHCARE SERVICES, INC.
(Exact Name of Registrant as Specified in Its Charter)
| Delaware | 06-1500476 | |
| (State or Other Jurisdiction of Incorporation or Organization) |
(I.R.S. Employer Identification No.) | |
| 12400 High Bluff Drive, Suite 100 San Diego, California |
92130 | |
| (Address of principal executive offices) | (Zip Code) | |
Registrant’s Telephone Number, Including Area Code: (866) 871-8519
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class | Name of each exchange on which registered | |
| Common Stock, $0.01 par value |
New York Stock Exchange |
Securities registered pursuant to Section 12(g) of the Act:
None.
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes þ No ¨
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes ¨ No þ
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes þ No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§ 229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. þ
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, or a non-accelerated filer. See definition of “accelerated filer and large accelerated filer” in Rule 12b-2 of the Exchange Act. (Check one):
Large accelerated filer ¨ Accelerated filer þ Non-accelerated filer ¨
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ¨ No þ
The aggregate market value of the voting and non-voting common equity held by non-affiliates computed by reference to the price at which the common equity was last sold, or the average bid and asked price of such common equity, as of June 30, 2005 was $425,716,258 based on a closing sale price of $15.03 per share.
As of March 9, 2006, there were 32,130,241 shares of common stock, $0.01 par value, outstanding.
Documents Incorporated By Reference: Portions of the registrant’s definitive Proxy Statement for the annual meeting of shareholders to be held on April 12, 2006 have been incorporated by reference into Part II and Part III of this Form 10-K.
Table of Contents
| Item |
Page | |||
| PART I | ||||
| 1. |
Business | 1 | ||
| 1A. |
Risk Factors | 12 | ||
| 1B. |
Unresolved Staff Comments | 18 | ||
| 2. |
Properties | 18 | ||
| 3. |
Legal Proceedings | 18 | ||
| 4. |
19 | |||
| PART II | ||||
| 5. |
20 | |||
| 6. |
21 | |||
| 7. |
Management’s Discussion and Analysis of Financial Condition and Results of Operations |
23 | ||
| 7A. |
35 | |||
| 8. |
36 | |||
| 9. |
Changes In and Disagreements With Accountants on Accounting and Financial Disclosure |
65 | ||
| 9A. |
65 | |||
| 9B. |
67 | |||
| PART III | ||||
| 10. |
68 | |||
| 11. |
68 | |||
| 12. |
Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
68 | ||
| 13. |
68 | |||
| 14. |
68 | |||
| PART IV | ||||
| 15. |
Exhibits and Financial Statement Schedules | 69 | ||
| Signatures | 75 | |||
i
Table of Contents
PART I
| Item 1. | Business |
Our Company
AMN Healthcare Services, Inc. “AMN”, is the largest temporary healthcare staffing company in the United States. As the leading nationwide provider of travel nurse staffing services and a leading provider of locum tenens (temporary physician staffing) and physician permanent placement services, we recruit physicians, nurses and allied health professionals, our “healthcare professionals,” nationally and internationally and place them on variable lengths of assignments and in permanent positions at acute-care hospitals, physician practice groups and other healthcare facilities throughout the United States. With the acquisition of The MHA Group, Inc., and its subsidiaries (“MHA”) on November 2, 2005, we expanded our service lines to include temporary and permanent physician staffing and clearly distinguished AMN as the largest healthcare staffing company.
Our staffing services are marketed to two distinct customer bases: (1) healthcare professionals and (2) hospital and healthcare facilities. We use a multi-brand recruiting strategy to enhance our ability to successfully attract nursing and allied healthcare professionals in the United States and internationally. We market our nurse and allied healthcare professional staffing to our healthcare professionals under recruitment brands including American Mobile Healthcare, Medical Express, NurseChoice InDemand, NursesRx, Preferred Healthcare Staffing, Thera Tech Staffing, Med Travelers, RN Demand, and O’Grady Peyton International. Each brand has distinct clinician focus, market strengths and brand reputation. We market our travel nursing services to hospitals and healthcare facilities under one brand, AMN Healthcare, as a single staffing provider with access to healthcare professionals from several recruitment brands. We market allied services to our clients under the brand names Thera Tech Staffing and Med Travelers, and we market long term nursing services to our clients under the brand name O’Grady Peyton International. We market our locum tenens and physician permanent placement services under the brand names Staff Care, Inc. and Merritt, Hawkins & Associates, respectively, to both healthcare professionals and hospital and healthcare facilities and physician staffing groups.
At the end of 2005, we had healthcare professionals on assignment at over 1,500 different healthcare facility clients. We provide services to acute-care and sub-acute healthcare facilities, physician groups, dialysis centers, clinics and schools. Our hospital and healthcare facility clients utilize our services to cost-effectively manage shortages in their staff due to a variety of circumstances such as attrition, new unit openings, seasonal patient census variations, the physician and nurse staffing shortage and other short and long-term staffing needs. In addition to providing continuity of care and quality patient care, we believe hospitals and healthcare facilities contract with us due to our skilled permanent and temporary healthcare professionals, our ability to meet their specific staffing needs, our flexible staffing assignment lengths, our reliable and superior customer service, our ability to offer a large national network of permanent and temporary healthcare professionals and our ability to provide temporary staffing solutions while we assist the client in filling physician permanent staffing needs.
Physicians, nurses and allied healthcare professionals join us on temporary assignments for a wide variety of reasons that include: seeking flexible work opportunities, exploring different areas of the country, building their clinical skills and resume by working at prestigious healthcare facilities, escaping the demands and political environment of working as a permanent staff and working through life and career transitions.
Our large number of hospital and healthcare facility clients provides us with the opportunity to offer temporary or permanent positions in all 50 states and in a variety of work environments and clinical settings. In addition, we provide our temporary healthcare professionals with an attractive benefits package that may include free or subsidized housing, free or reimbursed travel, competitive wages, professional development opportunities, a 401(k) plan, and health and professional liability insurance. We believe that we attract temporary healthcare professionals due to our long-standing reputation for providing a high level of service, our numerous job opportunities, our benefit packages, our innovative marketing programs and word-of-mouth referrals from our thousands of current and former healthcare professionals.
1
Table of Contents
Industry Overview
Total healthcare expenditures in the United States were estimated at $1.9 trillion during 2005, representing approximately 15.6% of the U.S. gross domestic product, and grew approximately 7% over 2004 according to the Centers for Medicare & Medicaid Services. Over the next decade, an aging U.S. population and advances in medical technology are expected to drive increases in hospital patient populations and the consumption of healthcare services. As a result, total healthcare expenditures are projected to increase to approximately $3.6 trillion by 2014.
The temporary healthcare staffing industry accounted for approximately $10.0 billion in revenue in 2005 according to estimates by The Staffing Industry Report, and is comprised of approximately 62% nurse staffing, 12% locum tenens, and the balance in allied health and other healthcare professional staffing. The temporary healthcare staffing industry was estimated to have grown at 2.5% in 2005 and has grown each year at a compound annual growth rate of approximately 9% since 1997, except during 2003 and 2004 when the industry declined on an annual basis. We believe that the decline during 2003 and 2004 reflected hospitals’ increased focus on internal nurse recruitment efforts, over-utilization of permanent labor staff and greater reliance on cost control efforts to reduce outsourced staffing solutions. In 2005, increased job turnover among permanent staff at the hospitals contributed to higher utilization of temporary nurses.
We expect the temporary healthcare staffing industry to grow modestly in 2006 based on favorable economic conditions and an increase in hospital staff job openings and turnover. While this growth is expected to be positive and expand the opportunities available to healthcare professionals, the available supply of professionals is not expected to keep pace with the increase in demand.
Competition
The healthcare staffing industry is highly competitive. We compete in national, regional and local markets with full-service staffing companies and specialized temporary staffing agencies for both healthcare professionals and hospital and healthcare facility clients. We also compete with hospital systems that have developed their own recruitment departments and interim staffing pools to attract highly qualified healthcare professionals. We compete for these healthcare professionals on the basis of customer service and expertise, the quantity, diversity and quality of available assignments, compensation packages and, for our temporary nurses and allied healthcare professionals, the benefits that we provide to them while they are on assignment. We compete with other staffing companies for hospital and healthcare facility clients on the basis of the quality of our healthcare professionals, the timely availability of our professionals with requisite skills, the quality, breadth and price of our services, our customer service, our recruitment expertise and the geographic reach of our services.
We believe that larger, national firms enjoy distinct competitive advantages over smaller, local and regional competitors in the healthcare staffing industry. More established firms have a larger pool of available candidates, substantial word-of-mouth referral networks and more recognizable brand names, enabling them to attract a consistent flow of new applicants. Larger firms also generally have a deeper, more comprehensive infrastructure with a more established business framework and processes that provide the foundation for national recognition, such as the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) staffing agency certification. The greater financial resources of these larger firms also make it relatively easier to provide payroll and housing services for its temporary healthcare professionals, which is cash flow intensive.
Some of our competitors in the temporary nurse and locum tenens staffing sector include Cross Country Healthcare, InteliStaf Healthcare, CHG Healthcare Services, Inc., On Assignment, and Medical Doctor Associates.
2
Table of Contents
Demand and Supply Drivers
Demand Drivers
| • | Demographics and Advances in Medicine and Technology. As the U.S. population ages and medical technology advances result in longer life expectancy, it is likely that chronic illnesses and hospital populations will continue to increase. We believe that these factors will increase the demand for both temporary and permanent healthcare professionals. In addition, enhanced healthcare technology has increased the demand for specialty physicians and nurses who are qualified to operate advanced medical equipment and perform complex medical procedures. |
| • | Increased Hospital Revenue Opportunity. Hospital and healthcare facilities’ primary revenue source is generated by physicians. By using permanent physician search and locum tenens services to fill vacancies quicker, hospitals and healthcare facilities can generate additional revenue. With more physicians on staff, healthcare facilities have a need for more nurses and allied healthcare professionals to support the increased patient census. |
| • | Shift to Flexible Staffing Models. Nurse wages comprise the largest percentage of hospitals’ labor expenses. Cost containment initiatives and a focus on cost-effective healthcare service delivery may lead more hospitals and other healthcare facilities to adopt adjustable staffing models that include utilization of flexible staffing resources such as temporary healthcare professionals. |
| • | Physician and Nursing Shortage. Most regions of the United States are experiencing a pronounced shortage of physicians and registered nurses. The Bureau of Labor Statistics projects that the incremental job openings for physicians and surgeons from 2002 to 2012 will be 114,000, an increase of 19.5% over ten years. The U.S. Department of Health and Human Services reported that the registered nurse workforce is expected to be 29% below projected requirements by 2020. Faced with increasing demand and tight supply for physicians and nurses, hospitals are utilizing more temporary physicians and nurses to meet staffing requirements. Factors contributing to the supply shortage of healthcare professionals include: |
| — | Changes in Physician and Nurse Population. Approximately 30% of all physicians are 55 years and older and approximately 38% are considering retirement in the next one to three years. The average age of a registered nurse was estimated to be 47 years old in 2004, an increase of 10.6% since 1996. |
| — | Shortage of Medical and Nursing Schools. As a result of a shortage of qualified faculty and limited availability of medical and nursing schools to prospective healthcare professionals, the number of medical school and nursing school graduates is well below the number of new healthcare professionals needed in order to eliminate the projected shortage. |
| — | Nurses Leaving Patient Care Environments for Less Stressful and More Flexible Careers. Career opportunities for nurses have expanded beyond the traditional bedside role. Pharmaceutical companies, insurance companies, HMOs and hospital service and supply companies increasingly offer nurses attractive positions which involve less demanding work schedules and more varied career progression and opportunity. |
| — | Physicians Leaving Practices Due to Increased Burdens of Malpractice Insurance and Medical Insurance Reimbursement. Physicians are increasingly concerned over reimbursement levels from insurance companies and government agencies and mounting claims billing restrictions and paperwork. In addition, malpractice premiums have been increasing over the last several years. |
3
Table of Contents
| • | Seasonality. Hospitals in regions that experience significant seasonal fluctuations in population, such as Florida or Arizona during the winter months, must be able to efficiently adjust their staffing levels to accommodate the change in patient census. Many of these hospitals utilize temporary healthcare professionals to satisfy these seasonal staffing needs. |
| • | State Legislation Requiring Healthcare Facilities to Utilize More Nurses. In response to concerns by nursing and consumer organizations over the quality of care provided in healthcare facilities and the increased workloads and pressures placed upon nurses, legislation has been introduced at both the federal and state level that is expected to increase the demand for nurses by requiring minimum nurse-to-patient ratios. Specifically, effective from January 2004, California hospitals have been required to staff units at government mandated nurse-to-patient ratios. New Jersey has enacted legislation requiring hospitals to post daily staffing information including nurse-to-patient ratios for each unit and shift, and to provide this information upon request by a member of the public. Illinois, Hawaii, Rhode Island, Florida, New Jersey and Iowa have also introduced legislation for minimum nurse-to-patient ratios in various healthcare settings. |
Supply Drivers
| • | Traditional Reasons for a Healthcare Professional to Work on a Temporary Assignment. Temporary staffing allows healthcare professionals to explore new areas of the United States, work at prestigious hospitals, learn new skills, manage work/life balance, build their resumes, try out different clinical settings, allow for a transitional period between permanent jobs and avoid unwanted workplace politics that may accompany a permanent position. Other benefits to temporary healthcare professionals could include free or subsidized housing, competitive wages, professional liability insurance coverage, professional development opportunities, health insurance and completion bonuses for some assignments. All of these opportunities have been constant supply drivers which continue to attract new healthcare professionals into our industry. |
| • | Word-of-Mouth Referrals. New applicants are often referred to staffing companies by other healthcare professionals who have taken temporary assignments with or been placed in a permanent position by the Company. Growth in the number of healthcare professionals who are working on temporary assignments or have been placed in permanent positions by a staffing agency, as well as the increased number of hospital and healthcare facilities that utilize temporary healthcare professionals, creates more opportunities for referrals. |
| • | More Physicians Choosing Temporary Staffing Due to the Physician Shortage, Increased Reimbursement and Malpractice Concerns. Locum tenens provides physicians the opportunity to practice medicine without concern for malpractice costs or having to worry about insurance reimbursement. In addition, the current and expected physician shortage allows physicians to practice medicine with confidence that they can explore other clinical settings and be secure about future permanent employment. |
| • | More Nurses Choosing Traveling Due to the Nursing Shortage and Improving Economy. In times of nursing shortages and an improving economy, nurses with permanent jobs generally feel more secure about their employment prospects. They have a higher degree of confidence that they can leave their permanent position to take a travel assignment and have the ability to return to a permanent position in the future. Additionally, during a nursing shortage, permanent staff nurses are often required to assume greater responsibility and patient loads, work overtime and deal with increased pressures within the hospital. Consequently, many experienced nurses choose to leave their permanent employer and look for a more flexible and rewarding position. |
| • | Legislation Allowing Nurses to Become More Mobile. The Mutual Recognition Compact Legislation, promoted by the National Council of State Boards of Nursing, allows nurses to work more freely within states participating in the Compact Legislation without obtaining new state licenses. The recognition legislation began in 1999 and has been enacted in 20 states as of February 2006. |
4
Table of Contents
Growth Strategy
Our goal is to expand our leadership position within the healthcare staffing sector in the United States. The key components of our business strategy include:
| • | Strengthening and Expanding Our Relationships with Hospitals and Healthcare Facilities. We continue to strengthen and expand our existing relationships with our hospital and healthcare facility clients and to develop new relationships. Hospitals and healthcare facilities are seeking a strong business partner for outsourcing and recruiting who can fulfill the quantity, breadth and quality of their staffing needs and help them develop strategies for the most cost-effective staffing methods. In addition, over the last few years, hospitals and healthcare facilities have shown an interest in working with a limited number of vendors to increase efficiency. We believe that our size and proven ability to fill our clients’ staffing needs provide us with the opportunity to serve our client facilities that implement this vendor consolidation strategy. In addition, our recent acquisition of MHA has broadened the type of services we offer and will allow us to provide a more comprehensive staffing solution to our clients. Because we possess one of the largest national networks of available physician, nurse and allied health professionals, we are well positioned to offer our hospital and healthcare facility clients a wide spectrum of effective solutions to meet their staffing needs. |
| • | Expanding Our Network of Qualified Healthcare Professionals. Through our recruiting efforts both in the United States and internationally, we continue to expand our network of qualified healthcare professionals. We continue to build our supply of healthcare professionals through referrals from healthcare professionals who are currently working or have been placed by us in the past, as well as through advertising and internet sources. We have also conducted several research initiatives to assist us in segmenting the population of healthcare professionals and developed targeted advertising campaigns directed at these different segments. |
| • | Leveraging Our Business Model and Large Hospital and Healthcare Facility Client Base to Increase Productivity. We seek to increase our productivity through our proven multi-brand recruiting strategy, large network of healthcare professionals, established hospital and healthcare facility client relationships, proprietary information systems, innovative marketing and recruitment programs, training programs and centralized administrative support systems. Our multi-brand recruiting strategy for temporary nurses generally allows a recruiter in any of our nurse staffing brands to take advantage of all of our nationwide placement opportunities. In addition, our information systems and operational support and customer service personnel permit our recruiters to spend more time focused on the placement of our healthcare professionals. |
| • | Expanding Service Offerings Through New Staffing Solutions. In order to further enhance the growth in our business and improve our competitive position in the healthcare staffing sector, we continue to introduce new service offerings. As our hospital and healthcare facility clients’ needs change, we constantly explore what additional services we can provide to better serve them. During 2005, we introduced NurseChoice In Demand to address hospitals’ urgent need for registered nurses and, through our recent acquisition of MHA, we have significantly expanded and differentiated our service offerings by entering the physician staffing sector. |
| • | Providing Innovative Technology. We continue to be an innovation leader in healthcare staffing by providing on-line services and tools to both our hospital and healthcare facility clients and our healthcare professionals. Our on-line resource, Staffing Service Center, provides online resources for hospital and healthcare facility clients to streamline their communications and process flow to secure and manage staffing services. Another on-line resource, The Traveler Service Center, provides an on-line self-service resource for our healthcare professionals to track assignment information and complete key forms electronically. Both sites offer secure access and self-service features twenty-four hours a day, seven days a week. |
5
Table of Contents
| • | Building the Strongest Management Team to Optimize Our Business Model. In addition to a tenured senior sales and operations management team, we have continued to focus on training and professional development for all levels of management and have hired several additional experienced management members over the last few years. Our management team has been further broadened and strengthened through the addition of the MHA leadership team. |
| • | Capitalizing on Strategic Acquisition Opportunities. In order to enhance our competitive position, we will continue to selectively explore strategic acquisitions. After acquisitions, we have sought to leverage our hospital relationships and orders across our brands, integrate back-office functions and maintain brand differentiation for temporary healthcare professional recruitment purposes. While we intend to operate our recently acquired physician staffing businesses relatively separate from our nurse and allied businesses, we believe we have opportunities to cross-sell our comprehensive staffing solution to our hospital and healthcare facility clients and integrate certain back-office functions. |
Business Overview
Services Provided
Nurse and Allied Healthcare Staffing Segment
Hospitals and healthcare facilities generally obtain supplemental staffing for nurses and allied healthcare professionals from two external sources, local temporary (per diem) agencies and regional and national travel healthcare staffing companies. Per diem staffing involves the placement of locally based healthcare professionals on daily shift work on an as needed basis. Hospitals and healthcare facilities often give only a few hours notice of their per diem assignments, which require a quick turnaround from their staffing agencies of generally less than 24 hours. Travel staffing, on the other hand, has historically provided hospital and healthcare facilities with staffing solutions to address anticipated or longer-term staffing requirements, typically for 4 to 26 weeks. In contrast to per diem agencies, travel staffing companies select from a national (and in some cases international) skilled labor pool and provide pre-screened candidates to their hospital and healthcare facility clients, typically at a lower cost. Historically, we have focused on the travel segment of the temporary healthcare staffing industry for our nurse and allied healthcare professionals. In addition, we have expanded our service offerings to include assignment lengths of 2 weeks to 24 months placing both domestic and international healthcare professionals.
Nurses. We provide medical nurses, surgical nurses, specialty nurses, licensed practical or vocational nurses and advanced practice nurses in a wide range of specialties for travel assignments throughout the United States. We place our qualified nurse professionals with premier, nationally recognized hospitals and hospital systems. The majority of our assignments are in acute-care hospitals, including teaching institutions, trauma centers and community hospitals. Nurses comprise approximately 93% of the total nurse and allied health temporary healthcare professionals working for us. We typically place the majority of our nurses on 13-week assignments with hospitals and healthcare facilities under our AMN Healthcare brand. We also offer a longer-term staffing solution under our O’Grady Peyton International brand, typically 18 months, using our English speaking international nurses that we recruit primarily from foreign countries. During 2005, we launched a differentiated new service offering, NurseChoice InDemand, to address hospitals’ urgent need for registered nurses. NurseChoice InDemand is targeted to recruit and staff nurses who can begin assignments within one to two weeks in acute-care facilities in contrast to the three to five week lead time that may be required for travel nurses. Typical assignments are four to eight weeks and provide premium compensation packages to nurses.
Allied Health Professionals. We also provide allied health professionals under our Med Travelers and Thera Tech Staffing brands to acute-care hospitals and other healthcare facilities such as skilled nursing facilities, rehabilitation clinics and schools. Allied health professionals include such disciplines as physical therapists, surgical technologists, respiratory therapists, medical and radiology technologists, dialysis technicians, speech pathologists and rehabilitation assistants. Allied health professionals comprise approximately 7% of the total nurse and allied health temporary healthcare professionals working for us.
6
Table of Contents
Physician Staffing Segment
Hospitals, physician groups and healthcare facilities generally obtain physicians from two sources, permanent hire and outsourced temporary physician staffing. We provide both temporary and permanent physician staffing services.
Locum Tenens. We place physicians of all specialties on a temporary basis (locum tenens) under our Staff Care brand as independent contractors with all types of healthcare organizations throughout the United States, including hospitals, medical groups, occupational medical clinics, individual practitioners, networks, psychiatric facilities, government institutions, and managed care entities. Physicians are recruited nationwide and typically placed on multi-week contracts. While assignments can range from a few days up to one year, the average is 8 weeks in duration. The locum tenens business comprises approximately 84% of our total physician staffing segment based on revenue.
Permanent Placement. We provide permanent physician placement services under our Merritt, Hawkins & Associates brand to medical facilities throughout the United States. Our broad specialty offerings include over 40 specialist and sub-specialist opportunities. Permanent physician placement comprises approximately 16% of our total physician staffing segment based on revenue.
Offering Comprehensive Healthcare Staffing Solutions
We employ a focused marketing strategy for our hospital and healthcare facility clients and market and administer the majority of our nursing services under the single corporate brand of AMN Healthcare. Our physician, allied and international staffing services are marketed to our hospital and healthcare facility clients under their respective brands.
The following chart depicts our comprehensive healthcare staffing capabilities and focus on critical staffing needs:
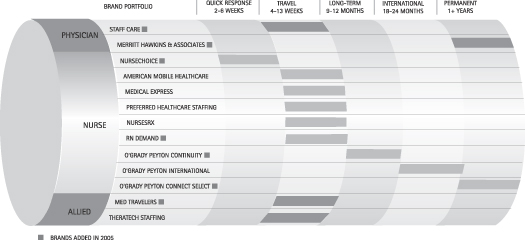
National Presence and Diversified Hospital and Healthcare Facility Client Base
We offer our healthcare professionals nationwide placement opportunities and provide staffing solutions to our hospital and healthcare facility clients that are located throughout the United States. We typically generate revenue in all 50 states. During 2005, the largest percentages of our revenue were concentrated in California, Arizona, Florida, New York, North Carolina and Massachusetts. Our physician permanent placement market has
7
Table of Contents
significant growth potential due to the increasing demand for physicians and the ability to cross-sell permanent placement services through our temporary service relationships. Our physician permanent placement brand, Merritt Hawkins & Associates has conducted over 30,000 physician search assignments since its founding and has worked in all 50 states.
We had temporary healthcare professionals on assignment at over 1,500 different healthcare facility clients at the end of 2005. The majority of our temporary healthcare professional assignments are at acute-care hospitals. In addition to acute-care hospitals, we provide services to sub-acute healthcare facilities, physician groups, dialysis centers, clinics and schools. Our clients include hospitals and healthcare systems such as Georgetown University Hospital, HCA, NYU Medical Center, Stanford Health Care, UCLA Medical Center and The University of Chicago Hospitals. No single client healthcare system comprised more than 10% of revenue and no single client facility comprised more than 3% of revenue for the year ended December 31, 2005.
Our Business Model
We have developed and continually refined our business model to achieve greater levels of productivity and efficiency. Our model is designed to optimize the communication with, and service to, both our healthcare professionals and our hospital and healthcare facility clients.
Marketing and Recruitment of New Healthcare Professionals
We believe that physician, nursing and allied health professionals are attracted to us because of our customer service and relationship-oriented approach, our competitive compensation and benefits package, and our large and diverse offering of work assignments that provide the opportunity to work at numerous attractive locations throughout the United States. We believe that our multi-brand recruiting strategy makes us more effective at reaching a larger number of healthcare professionals.
Screening, Licensing and Quality Management
Through our quality management and assurance departments, we screen all candidates prior to placement, and we continue to evaluate our temporary healthcare professionals after they are placed to ensure adequate performance and manage risk, as well as to determine feasibility for future placements. Our internal processes are designed to ensure that our healthcare professionals have the appropriate experience, credentials and skills for the assignments that they accept. Our experience has shown us that well-matched placements result in satisfied healthcare professionals and healthcare facility clients.
Sales, Marketing and Account Management
We market our nursing services to hospitals and healthcare facilities generally under one corporate brand name, AMN Healthcare, a single staffing provider with several recruitment sources of healthcare professionals. We utilize a team approach to service our hospital and healthcare facility clients. This team includes the Regional Client Service Director, Hospital Account Manager, Quality Management, and Clinical Liaison. We market our temporary and permanent physician placement services under the brand names Staff Care, Inc. and Merritt, Hawkins and Associates, respectively. We have a large base of professionals marketing our physician staffing services to our clients who make thousands of client contacts each month.
Placement
For the nurse and allied healthcare staffing segment, generally, orders are entered into our information network by our hospital account managers and are available to the recruiters at all of our recruitment brands.
8
Table of Contents
The hospital account managers develop a relationship with the healthcare facility, arrange telephone interviews between the temporary healthcare professional and the hospital, and confirm offers and placements with the hospital or healthcare facility. At the same time, our recruiters seek to develop and maintain strong and lasting relationships with our healthcare professionals.
In the case of our international temporary healthcare professionals, the recruiters and placement coordinators at our O’Grady Peyton International brand, including those located in the United Kingdom, Australia and South Africa, assist candidates in preparing for the United States nursing examination and subsequently obtaining a U.S. nursing license. These recruiters and other staff also assist our international temporary healthcare professionals to obtain petitions to become lawful permanent residents prior to their arrival in the United States. Our international temporary healthcare professionals are typically placed on longer-term, 18-month assignments as a result of our substantial investment in bringing them to work in the United States. Near completion of the 18-month assignment, our recruiters will work with these temporary healthcare professionals to explore their options for new assignments.
For the physician staffing segment, orders for temporary physicians or permanent placement requests are generated by our national marketing team. Our national presence and infrastructure enable us to provide physicians with a variety of attractive client locations, perquisites and opportunities for career development. Our recruiters and account representatives work together using proprietary information systems to fill orders and schedule physicians on temporary assignments. Our permanent placement recruiters work closely with our clients and marketing team to recruit and fill permanent placement requests. We also have the ability to cross-sell our permanent placement and temporary placement services to our clients.
Housing and Support Services
We offer substantially all of our temporary healthcare professionals free or subsidized housing while on assignment. For our nurse and allied placements, housing expenses are typically included in the hourly or weekly fees that we charge to our hospital and healthcare facility clients. For our locum tenens placements, housing costs are typically billed separately. We negotiate contracts with national property management and furniture rental companies to leverage our size and obtain more favorable pricing and terms.
Temporary Healthcare Professional Compensation
During 2005, approximately 94% of our working temporary healthcare professional employees were compensated directly by us, while approximately 6% were paid directly by the hospital or healthcare facility client.
Temporary Healthcare Professional Benefits
In our effort to attract and retain highly qualified temporary healthcare professionals, we offer a variety of benefits. These benefits may include: travel reimbursement; group medical, dental and life insurance; referral bonuses; completion bonuses; 401(k) plan and dependent care and medical reimbursement; and free continuing education.
Hospital Billing
To accommodate the needs of our hospital clients, for temporary healthcare professional staffing, we offer two types of billing: hours and days worked contracts and flat fee contracts. During 2005, we billed approximately 94% of working nurse and allied healthcare professionals based on hours and days worked contracts and approximately 6% based on flat rate contracts, and we billed substantially all of the working temporary physicians based on hours and days worked contracts.
9
Table of Contents
Hours and Days Worked Contracts. Under hours and days worked contracts, the temporary healthcare professional is either our employee for payroll and benefits purposes or an independent contractor paid directly by us on behalf of the hospital and healthcare facility clients. Under this arrangement, we bill our hospital and healthcare facility clients at an hourly or daily rate that effectively includes reimbursement for recruitment fees, compensation and benefits for the temporary healthcare professional and any applicable employer taxes. Housing or travel expenses are either included in the rate or billed separately. Overtime, shift differential and holiday hours worked are typically billed at a premium rate. In turn, we pay the temporary healthcare professional’s wages or contracted fees, housing and travel costs and benefits. Providing payroll services is a value-added and convenient service that hospitals and healthcare facilities generally expect from their supplemental staffing sources.
Flat Rate Contracts. With flat rate contracts, the temporary healthcare professional is compensated directly by the hospital or healthcare facility. We bill the hospital a “flat” weekly rate that includes reimbursement for recruitment fees, temporary healthcare professional benefits and typically housing expenses, which may be billed separately.
Information Systems
Our primary management information and communications systems are centralized and controlled in our corporate headquarters in San Diego, CA for nursing and in the MHA headquarters in Irving, TX for physicians. Our financial and payroll systems are centralized at these headquarters and our operational reporting is standardized at all of our offices.
We have developed and currently operate proprietary information systems that include integrated processes for healthcare professional and healthcare facility contract management, matching of healthcare professionals with clients and assignments, healthcare professional file submissions for placements, quality management tracking, controlling compensation packages and managing healthcare facility contract and billing terms. These systems provide our staff with fast, detailed information regarding individual healthcare professionals and hospital and healthcare facility clients.
Risk Management
We have developed an integrated risk management program that focuses on loss analysis, education and assessment in an effort to reduce our operational costs and risk exposure. We regularly analyze our losses on professional liability claims and workers compensation claims to identify trends. This allows us to focus our resources on those areas that may have the greatest impact on us and adjust our sales and operational approach to these areas. We have also developed educational materials for distribution to our temporary healthcare professionals that are targeted to address specific work-injury risks and documentation of clinical events.
In addition to our proactive measures, we engage in a peer review process of any incidents involving our temporary nurses and allied healthcare professionals. Upon notification of a nurse or allied healthcare professional’s involvement in an incident that may result in liability for us, our corporate team of registered nurses reviews the healthcare professional’s actions. Our peer review committee makes a prompt determination regarding whether the healthcare professional will continue the assignment and whether we will place him/her on future assignments. We also rely on our hospital and healthcare facility clients and the state professional associations’ investigation of incidents in determining continued and future assignments.
Regulation
The healthcare industry is subject to extensive and complex federal and state laws and regulations related to professional licensure, conduct of operations, payment for services and payment for referrals. Our business, however, is not directly impacted by or subject to the extensive and complex laws and regulations that generally
10
Table of Contents
govern the healthcare industry. The laws and regulations that are applicable to our hospital and healthcare facility clients could indirectly impact our business to a certain extent, but because we provide services on a contract basis and are paid directly by our hospital and healthcare facility clients, we do not have any direct Medicare or managed care reimbursement risk.
Some states require state licensure for businesses that employ, assign and/or place healthcare personnel to provide healthcare services at hospitals and other healthcare facilities. We are currently licensed in states that require such licenses and take measures to ensure compliance with all material state licensure requirements. In addition, we received our JCAHO Corporate Certification for AMN Healthcare and the nurse and allied brands of American Mobile Healthcare, Medical Express, NursesRx, Preferred Healthcare Staffing and Thera Tech Staffing based on a review of our compliance with national standards during the second quarter of 2005. We were the first healthcare staffing firm in the country to receive the prestigious JCAHO Certification as a corporate system with multiple staffing sites.
Most of the temporary healthcare professionals that we employ or independently contract with are required to be individually licensed or certified under applicable state laws. We take prudent steps to ensure that our healthcare professionals possess all necessary licenses and certifications.
We recruit nurses from Canada for placement in the United States. Canadian nurses can come to the United States on TN Visas under the North American Free Trade Agreement. TN Visas are renewable, one-year temporary work visas, which generally allow entrance into the United States provided the nurse presents at the border proof of waiting employment in the United States, evidence of the necessary healthcare practice licenses and a visa credentials assessment from the Commission on Graduates of Foreign Nursing Schools.
With respect to our recruitment of international temporary healthcare professionals through our O’Grady Peyton International brand, we must comply with certain United States immigration law requirements, including the Illegal Immigration Reform and Immigrant Responsibility Act of 1996. We primarily bring healthcare professionals to the United States as immigrants, or lawful permanent residents (commonly referred to as “green card” holders). We screen foreign healthcare professionals and assist them in preparing for the national nursing examination and subsequently obtaining a U.S. nursing license. We file petitions with the United States Citizenship and Immigration Service for a healthcare professional to become a permanent resident of the United States or obtain necessary work visas. Generally, such petitions are accompanied by proof that the healthcare professional has either passed the Commission on Graduates of Foreign Nursing Schools Examination or holds a full and unrestricted state license to practice professional nursing, as well as a contract between us and the healthcare professional demonstrating that there is a bona fide job offer.
Employees
As of December 31, 2005, we had approximately 1,700 corporate employees. During the fourth quarter of 2005, we had an average of over 6,500 nurse and allied healthcare professionals working on assignment. Since our acquisition of MHA on November 2, 2005 through December 31, 2005, days filled by our physician independent contractors totaled 29,570. Days filled is calculated by dividing the physician independent contractor hours filled during the period by 8 hours.
Additional Information
We maintain a corporate website at www.amnhealthcare.com/investors. Our Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K and amendments to these reports, are made available, free of charge, through this website as soon as reasonably practicable after being filed with or furnished to the Securities and Exchange Commission. The information found on our website is not part of this or any other report we file with or furnish to the Securities and Exchange Commission.
11
Table of Contents
| Item 1A. | Risk Factors |
The following risk factors should be read carefully in connection with evaluating us and the forward-looking statements contained in this Annual Report on Form 10-K. Any of the following risks could materially adversely affect our company, operating results, financial condition and the actual outcome of matters as to which forward- looking statements are made in this Annual Report on Form 10-K. Certain statements in “Risk Factors” constitute “forward-looking statements.” Our actual results could differ materially from those projected in the forward-looking statements as a result of certain factors and uncertainties set forth below and elsewhere in this Annual Report on Form 10-K. See “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations—Special Note Regarding Forward-Looking Statements.”
If we are unable to continue to recruit and retain healthcare professionals for our healthcare staffing business at reasonable costs, it could increase our operating costs and negatively impact our business.
We rely significantly on our ability to recruit and retain healthcare professionals who possess the skills, experience and licenses necessary to meet the requirements of our hospital, healthcare facility clients and physician practice groups. We compete for healthcare staffing personnel with other temporary healthcare staffing companies and with hospitals, healthcare facilities and physician practice groups based on the quantity, diversity and quality of assignments offered, compensation packages and the benefits that we provide to our healthcare professionals. We rely on our human capital intensive, relationship-oriented approach and national infrastructure to enable us to compete in the permanent physician staffing business. We must continually evaluate and expand our temporary and permanent healthcare professional network to keep pace with the needs of our hospital, healthcare facility clients and physician practice groups.
Currently, there is a shortage of qualified nurses, physicians and certain allied healthcare professionals in the United States, significant competition exists for these personnel, and salaries and benefits have risen. We may be unable to continue to increase the number of temporary and permanent healthcare professionals that we recruit, decreasing the potential for growth of our business. Our ability to recruit and retain temporary and permanent healthcare professionals depends on several factors, including our ability to provide our healthcare professionals with assignments and placements that they view as attractive and to provide our temporary healthcare professionals with competitive wages and benefits, including health insurance and housing. We cannot assure you that we will be successful in any of these areas as the costs of attracting healthcare professionals and providing them with attractive benefit packages may be higher than we anticipate, or we may be unable to pass these costs on to our hospital and healthcare facility clients. If we are unable to increase the rates that we charge our hospital and healthcare facility clients to cover these costs, our profitability could decline. Moreover, if we are unable to recruit temporary and permanent healthcare professionals, the quality of our services to our hospital and healthcare facility clients may decline and, as a result, we could lose clients.
Our operations may deteriorate if we are unable to continue to attract, develop and retain our sales and operations personnel.
Our success is dependent upon the performance of our sales and operations personnel. The number of individuals who meet our qualifications for these positions is limited, and we may experience difficulty in attracting qualified candidates. In addition, we commit substantial resources to the training, development and support of our personnel. Competition for qualified sales personnel in the line of business in which we operate is strong, and there is a risk that we may not be able to retain our sales personnel after we have expended the time and expense to recruit and train them.
12
Table of Contents
We operate in a highly competitive market and our success depends on our ability to remain competitive in obtaining and retaining hospital, healthcare facility and physician practice group clients and demonstrating the value of our services.
The temporary healthcare staffing business is highly competitive. We compete in national, regional and local markets with full-service staffing companies, specialized temporary staffing agencies and hospital systems that have developed their own interim staffing pools. Some of our large competitors in the temporary nurse and locum tenens staffing sectors include Cross Country Healthcare, InteliStaf Healthcare, CHG Healthcare Services, Inc., On Assignment, and Medical Doctor Associates.
We believe that the primary competitive factors in obtaining and retaining hospital, healthcare facility and physician practice group clients are identifying qualified healthcare professionals for specific job requirements, providing qualified employees in a timely manner, pricing services competitively and effectively monitoring employees’ job performance. Competition for hospital, healthcare facility and physician practice group clients and temporary and permanent healthcare professionals may increase in the future due to these factors or a shortage of qualified healthcare professionals in the marketplace and, as a result, we may not be able to remain competitive. To the extent competitors seek to gain or retain market share by reducing prices or increasing marketing expenditures, we could lose revenue or clients and our margins could decline, which could seriously harm our operating results and cause the price of our stock to decline. In addition, the development of alternative recruitment channels could lead our clients to bypass our services, which would also cause revenue and margins to decline.
Our business depends upon our ability to secure and fill new orders from our hospital, healthcare facility and physician practice group clients because our temporary healthcare staffing business does not have long-term, exclusive or guaranteed contracts with them, and economic conditions may adversely impact the number of new orders and contracts we receive.
We generally do not have long-term, exclusive or guaranteed order contracts for temporary healthcare staffing with our hospital, healthcare facility and physician practice group clients. The success of our business is dependent upon our ability to continually secure new contracts and orders from hospitals, healthcare facilities and physician practice groups and to fill those orders with our temporary healthcare professionals. Our hospital, healthcare facility and physician practice group clients are free to award contracts and place orders with our competitors and choose to use temporary healthcare professionals that our competitors offer them. Therefore, we must maintain positive relationships with our hospital, healthcare facility and physician practice group clients. If we fail to maintain positive relationships with our hospital, healthcare facility and physician practice group clients or are unable to provide a cost-effective staffing solution, we may be unable to generate new temporary healthcare professional orders and our business may be adversely affected.
Some hospitals and healthcare facility clients choose to outsource this contract and order function to staffing associations owned by member healthcare facilities or companies with vendor management services that may act as intermediaries with our client facilities. These organizations may impact our ability to obtain new clients and maintain our existing client relationships by impeding our ability to access and contract directly with healthcare facility clients. Additionally, we may experience pricing pressure or incremental fees from these organizations that may negatively impact our revenue and profitability.
Depressed economic conditions, such as increasing unemployment rates and low job growth, could also negatively influence our ability to secure new orders and contracts from clients. In times of economic downturn, permanent healthcare facility staff may be more inclined to work overtime and less likely to leave their positions, resulting in fewer available vacancies and less demand for our services. Fewer placement opportunities for our temporary healthcare professionals impairs our ability to recruit and place both temporary and permanent placement healthcare professionals and our revenues and profitability may decline as a result of this constricted demand and supply.
13
Table of Contents
The demand for our services, and therefore the profitability of our business, may be adversely affected by changes in the staffing needs due to fluctuations in hospital admissions or staffing preferences of our healthcare facility clients.
The temporary healthcare staffing industry grew from 1996 through 2002, declined in early 2003 and stabilized and grew modestly from late 2003 through 2005. Demand for our temporary healthcare staffing services is affected by the staffing needs and preferences of our healthcare facility clients, as well as by fluctuations in patient occupancy at our client healthcare facilities due to economic factors and seasonal fluctuations that are beyond our control.
Hospitals in certain geographical regions experience significant seasonal fluctuations in admissions, and must be able to adjust their staffing levels to accommodate the change in patient census. Our healthcare facility clients may choose to use temporary staff, additional overtime from their permanent staff or add new permanent staff in order to accommodate changes in their staffing needs. Many healthcare facilities will utilize temporary healthcare professionals to accommodate an increase in hospital admissions. Alternatively, if hospital admissions decrease, the demand for our temporary healthcare professionals may decline as healthcare facility clients typically will reduce their use of temporary staff before reducing the workload or undertaking layoffs of their regular employees. In addition, we may experience more competitive pricing pressure during periods of patient occupancy and hospital admission downturns, negatively impacting our revenue and profitability.
The ability of our hospital, healthcare facility and physician practice group clients to retain and increase the productivity of their permanent staff may affect the demand for our services.
If our hospital, healthcare facility and physician practice group clients retain and increase the productivity of their permanent staff, their need for our services may decline. Higher permanent staff retention rates and increased productivity of permanent staff members could result in increased efficiencies, thereby reducing the demand for both our temporary staffing and permanent placement services, which could negatively impact our revenue and profitability.
We operate in a regulated industry and changes in regulations or violations of regulations may result in increased costs or sanctions that could reduce revenue and profitability and may impact our ability to grow and operate our business.
The healthcare industry is subject to extensive and complex federal and state laws and regulations related to professional licensure, conduct of operations, costs and payment for services and payment for referrals.
Our business is generally not subject to the extensive and complex laws that apply to our hospital, healthcare facility and physician practice group clients, including laws related to Medicare, Medicaid and other federal and state healthcare programs. However, these laws and regulations could indirectly affect the demand or the prices paid for our services. For example, our hospital, healthcare facility and physician practice group clients could suffer civil and criminal penalties and be excluded from participating in Medicare, Medicaid and other healthcare programs if they fail to comply with the laws and regulations applicable to their businesses.
In addition, our hospital, healthcare facility and physician practice group clients could receive reduced reimbursements, or be excluded from coverage, because of a change in the rates or conditions set by federal or state governments. In turn, violations of or changes to these laws and regulations that adversely affect our hospital, healthcare facility and physician practice group clients could also adversely affect the prices and demand for our services. For example, legislation in Massachusetts limited the hourly rate paid to temporary nursing agencies for registered nurses, licensed practical nurses and certified nurses aides. While we are exempt from this regulation, in part, similar regulations may be enacted in other states in which we operate, and as a result revenue and margins could decrease. Furthermore, third party payers, such as health maintenance organizations, increasingly challenge the prices charged for medical care. Failure by hospitals, healthcare
14
Table of Contents
facilities and physician practice groups to obtain full reimbursement from those third party payers could reduce the demand or the price paid for our services.
We are also subject to certain laws and regulations applicable to healthcare staffing agencies and general temporary staffing services. Like all employers, we must also comply with various laws and regulations relating to pay practices, workers compensation and immigration. As we continue to grow, we believe that we are more likely to be a target of challenges to our pay practices, such as challenges to our employee classifications under the Fair Labor Standards Act. There is a risk that we could be subject to payment of additional wages, insurance and employment and payroll related taxes if certain of our corporate employees classified as exempt from overtime and minimum wage requirements are re-classified as non-exempt from overtime and minimum wage requirements. Because of the nature of our business, the impact of these laws and regulations may have a more pronounced effect on our business. These laws and regulations may also impede our ability to grow our operations.
We primarily draw our supply of healthcare professionals from the United States, but international supply channels have represented a small but growing temporary nurse supply source. Our ability to recruit healthcare professionals through these foreign supply channels may be impacted by government legislation limiting the number of immigrant visas that can be issued.
Additionally, we have incurred and will continue to incur additional legal and accounting expenses related to compliance with corporate governance and disclosure standards implemented by the Sarbanes-Oxley Act of 2002, the rules of the New York Stock Exchange and regulations of the Securities and Exchange Commission. Regulations promulgated in connection with Section 404 of the Sarbanes-Oxley Act of 2002 require an annual and quarterly review by management and evaluation of our internal control systems, in addition to an annual auditor attestation of the effectiveness of these systems, which commenced with our fiscal year ended on December 31, 2004 (exclusive of our recent acquisition of The MHA Group, Inc.). In addition, as of December 31, 2006, we will need to certify the sufficiency of the internal control systems of MHA. If we fail to comply with these laws and regulations, damages, civil and criminal penalties, injunctions and cease and desist orders may be imposed, which would negatively impact our business and operations. The increase in costs necessitated by compliance with the laws and regulations affecting our business reduces our overall profitability, and reduces the assets and resources available for utilization in the expansion of our business operations.
Our profitability is impacted by our ability to leverage our cost structure.
We have technology, operations and human capital infrastructures to support our existing business and contemplated growth. In the event that our business does not grow at the rate that we had anticipated, our inability to reduce these costs would impair our profitability. Additionally, if we are not able to capitalize on this infrastructure our earnings growth rate will be impacted.
The variation in pricing of the healthcare facility contracts under which we place temporary and permanent healthcare professionals impacts our profitability.
The pricing of our contracts with hospitals, healthcare facilities and physician practice groups may vary depending on circumstances, including geographic location, economic conditions and supply and demand factors. These pricing variables impact our gross margin and could result in decreased profitability if we are unable to renew existing accounts on economically favorable terms.
15
Table of Contents
We may not be able to successfully implement our strategic growth, acquisition and integration strategies.
An effective growth management strategy is necessary to organically grow our current operations, and if we do not successfully execute on this growth strategy, our profitability could decline. We continue to explore strategic acquisition opportunities to supplement our organic growth strategy. Acquisitions involve significant risks and uncertainties, including difficulties integrating acquired personnel and other corporate cultures into our business, the potential loss of key employees or customers of acquired companies, the assumption of liabilities and exposure to unforeseen liabilities of acquired companies and the diversion of management attention from existing operations. We may not be able to fully integrate the operations of the acquired businesses with our own in an efficient and cost-effective manner. Acquisitions may also require significant expenditures of cash and other resources and assumption of debt that may ultimately negatively impact our overall financial performance. In particular, we are still in the process of integrating our recent MHA acquisition.
Difficulties in maintaining our management information and communications systems may result in increased costs that reduce our profitability.
Our ability to deliver our staffing services to our hospital, healthcare facility and physician practice group clients and manage our internal systems depends to a large extent upon our access to and the performance of our management information and communications systems. These systems also maintain accounting and financial information, which we depend upon to fulfill our financial reporting obligations. If these systems do not adequately support our operations, these systems are damaged or if we are required to incur significant additional costs to repair, maintain or expand these systems, our business and financial results could be materially adversely affected. Although we have risk mitigation measures, these systems, and our access to these systems, are not impervious to floods, fire, storms, or other natural disasters, and the loss of systems information could result in disruption to our business.
The challenge to the classification of certain of our healthcare professionals as independent contractors could adversely impact our profitability.
Although there is a long-standing industry standard to treat physicians as independent contractors, there is a risk we could be subject to additional wage and insurance claims, employment and payroll-related taxes if federal or state taxing authorities re-classify our independent contractor physicians as employees, which would significantly reduce our profitability. In addition, many states have laws which prohibit non-physician owned companies from employing physicians which we refer to as the “corporate practice of medicine.” If our independent contractor physicians are classified as employees, we would be in violation of state laws that prohibit the corporate practice of medicine, which would have a substantial negative impact on our profitability.
The impact of medical malpractice and other claims asserted against us could subject us to substantial liabilities.
In recent years, our hospital, healthcare facility and physician practice group clients are subject to a number of legal actions alleging malpractice or related legal theories. Because our temporary and permanent healthcare professionals provide medical care and we provide credentialing of these healthcare professionals, claims may be brought against us and our healthcare professionals relating to the recruitment and qualification of these healthcare professionals and the quality of medical care provided by our temporary healthcare professionals while on assignment or after placement at our hospital, healthcare facility and physician practice group clients. We and the healthcare professional are at times named in these lawsuits regardless of our contractual obligations, the competency of the healthcare professional, the standard of care provided by the healthcare professional or the quality of service that we provided. In some instances, we are required to indemnify hospital, healthcare facility and physician practice group clients contractually against some or all of these potential legal actions. Also, because some of our temporary healthcare professionals are our employees, we may be subject to various employment claims and contractual disputes regarding the terms of a temporary healthcare professional’s employment.
16
Table of Contents
Because we are in the business of placing our temporary healthcare professionals in the workplaces of other companies, we are subject to possible claims by our temporary healthcare professionals alleging discrimination, sexual harassment and other similar activities by our hospital and healthcare facility clients. We maintain a policy for employment practices coverage. However, the cost of defending such claims, even if groundless, could be substantial and the associated negative publicity could adversely affect our ability to attract, retain and place qualified individuals in the future.
We maintain various types of insurance coverage, including professional liability, workers compensation and employment practices, through insurance carriers, and we also self-insure for these claims through accruals for retention reserves. We may experience increased insurance costs and reserve accruals and may not be able to pass on all or any portion of increased insurance costs to our hospital, healthcare facility and physician practice group clients, thereby reducing our profitability. Our insurance coverage and reserve accruals may not be sufficient to cover all claims against us, and we may be exposed to substantial liabilities.
Terrorist threats or attacks may disrupt or adversely affect our business operations.
Our business operations may be interrupted or adversely impacted in the United States and abroad in the event of a terrorist attack or heightened security alerts. Our temporary healthcare professionals may become reluctant to travel and may decline assignments based upon the perceived risk of terrorist activity, which would reduce our revenue and profitability. In addition, terrorist activity or threats may impede our access to our management and information systems resulting in loss of revenue. We do not maintain insurance coverage against terrorist attacks.
If we are unable to carry out our business strategy our profitability could be negatively impacted.
Our success is dependent on our ability to execute our business strategy, which necessarily involves the successful operation of a number of integral components and business objectives. Our ability to execute these business objectives is dependent upon a sufficient cash flow and capital structure to support the business. If we are unable to access credit on commercially reasonable terms or our cash flow is significantly impaired, our profitability could be negatively impacted.
The loss of key officers and management personnel could adversely affect our ability to remain competitive.
We believe that the success of our business strategy and our ability to operate profitably depends on the continued employment of our senior management team. We have employment agreements only with Steven C. Francis, our Executive Chairman, Susan R. Nowakowski, our President and Chief Executive Officer, and two non-executive officers. If these individuals or members of our senior management team become unable or unwilling to continue in their present positions, our business and financial results could be materially adversely affected.
We have a substantial amount of goodwill on our balance sheet that may have the effect of decreasing our earnings or increasing our losses in the event that we are required to recognize an impairment to goodwill.
As of December 31, 2005, we had $240.8 million of unamortized goodwill on our balance sheet, which represents the excess of the total purchase price of our acquisitions over the fair value of the net assets acquired. At December 31, 2005, goodwill represented 38.9% of our total assets.
SFAS No. 142, Goodwill and Other Intangible Assets requires that goodwill not be amortized but rather that it be reviewed annually for impairment. In the event impairment is identified, a charge to earnings would be recorded. Although an impairment charge to earnings for goodwill would not affect our cash flow, it would
17
Table of Contents
decrease our earnings or increase our losses, as the case may be, and our stock price could be adversely affected. We have reviewed our goodwill for impairment in accordance with the provisions of SFAS No. 142, and have not identified any impairment to goodwill.
We have a substantial accrual for self-insured retentions on our balance sheet, and any significant adverse adjustments in these accruals may have the effect of decreasing our earnings or increasing our losses.
We maintain accruals for self-insured retentions for professional liability, health insurance and workers compensation on our balance sheet. Increases to these accruals do not immediately affect our cash flow, but a significant increase to these self-insured retention accruals may decrease our earnings or increase our losses, as the case may be. We determine the adequacy of our self-insured retention accruals by evaluating our historical experience and trends, related to both insurance claims and payments, information provided to us by our insurance brokers and third party administrators, as well as industry experience and trends. If such information indicates that our accruals are overstated or understated, we reduce or provide for additional accruals, as appropriate.
| Item 1B. | Unresolved Staff Comments |
None.
| Item 2. | Properties |
We believe that our leased space is adequate for our current needs. In addition, we believe that adequate space can be obtained to meet our foreseeable business needs. In accordance with, and as required by, the terms of our New Credit Agreement, we have pledged substantially all of our assets and properties to our lenders under our New Credit Agreement to secure our obligations thereunder. Our principal leases as of December 31, 2005 are identified in the chart below:
| Location |
Square Feet | |
| San Diego, California (corporate headquarters) |
175,672 | |
| Irving, Texas |
125,909 | |
| Huntersville, North Carolina |
30,870 | |
| Ft. Lauderdale, Florida |
25,408 | |
| Westminster, Colorado |
19,427 | |
| Salt Lake City, Utah |
13,347 | |
| Atlanta, Georgia |
13,302 | |
| Irvine, California |
6,165 | |
| Savannah, Georgia |
4,780 | |
| London (United Kingdom) |
3,391 | |
| Sydney (Australia) |
2,788 | |
| Birmingham (United Kingdom) |
2,300 |
| Item 3. | Legal Proceedings |
We are subject to various claims and legal actions in the ordinary course of our business. Some of these matters include professional liability, tax, payroll and employee-related matters and inquiries and investigations by governmental agencies regarding our employment practices. We are not aware of any pending or threatened litigation that we believe is reasonably likely to have a material adverse effect on our results of operations, financial position or liquidity.
18
Table of Contents
Our hospital and healthcare facility clients may also become subject to claims, governmental inquiries and investigations and legal actions to which we may become a party relating to services provided by our professionals. From time to time, and depending upon the particular facts and circumstances, we may be subject to indemnification obligations under our contracts with our hospital and healthcare facility clients relating to these matters. At this time, we are not aware of any such pending or threatened litigation that we believe is reasonably likely to have a material adverse effect on our results of operations, financial position or liquidity.
| Item 4. | Submission of Matters to a Vote of Security Holders |
No matters were submitted to a vote of security holders during the fourth quarter of fiscal 2005.
19
Table of Contents
PART II
| Item 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Our common stock has traded on the New York Stock Exchange under the symbol “AHS” since our initial public offering on November 13, 2001. Prior to that time, there was no public trading market for our common stock. The following table sets forth, for the periods indicated, the high and low sales prices reported by the New York Stock Exchange.
| Sales Price | ||||||
| High |
Low | |||||
| Year Ended December 31, 2004 |
||||||
| First Quarter |
$ | 21.56 | $ | 17.00 | ||
| Second Quarter |
$ | 18.58 | $ | 14.49 | ||
| Third Quarter |
$ | 15.35 | $ | 11.26 | ||
| Fourth Quarter |
$ | 16.66 | $ | 10.70 | ||
| Year Ended December 31, 2005 |
||||||
| First Quarter |
$ | 16.85 | $ | 12.85 | ||
| Second Quarter |
$ | 16.55 | $ | 13.62 | ||
| Third Quarter |
$ | 17.46 | $ | 14.85 | ||
| Fourth Quarter |
$ | 20.73 | $ | 14.73 | ||
We completed secondary offerings of our common stock for 2,300,000 and 10,631,303 shares on April 18, 2005 and May 27, 2005, respectively. All of the 12,931,303 shares were sold by affiliates of Haas Wheat & Partners, L.P. (the “HWP Stockholders”), a private equity investment firm whose affiliates had owned shares of the company since 1999. We incurred issuance costs associated with the offerings of approximately $0.5 million during the second quarter of 2005, which were recorded in the Company’s stockholders’ equity.
As of March 9, 2006, there were 32,130,241 shares of our common stock issued and outstanding that were held by 27 stockholders of record. On March 9, 2006, the last reported sale price of our common stock on the New York Stock Exchange was $19.49 per share.
On November 2, 2005, we issued 2.3 million shares of common stock in connection with our acquisition of MHA, and we issued an additional 0.7 million shares on March 9, 2006 for payment of earn-out amounts as provided in the acquisition agreement. The issuance is exempt from the registration requirements of the Securities Act of 1933, as amended (the “Securities Act”), pursuant to Section 4(2) thereof and Regulation D promulgated thereunder (“Regulation D”), based upon representations that the Company has obtained from each MHA shareholder receiving such shares, including that such shareholder is an “accredited investor” as such term is defined in Rule 501(a) of Regulation D. Concurrently with the filing of this Form 10-K, on March 10, 2006, we will file a registration statement on Form S-3 to register the 2.3 million shares of common stock in connection with our acquisition of MHA and the additional 0.7 million shares for payment of the earn-out amounts as provided in the acquisition agreement.
We have not paid any dividends in the past and currently do not expect to pay cash dividends or make any other distributions in the future. We expect to retain our future earnings, if any, for use in the operation and expansion of our business. Any future determination to pay dividends will be at the discretion of our board of directors and will depend upon our financial condition, results of operations, capital requirements and such other factors as our board deems relevant. In addition, our ability to declare and pay dividends on our common stock is subject to covenants in our credit facility. See “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations—Liquidity and Capital Resources.”
20
Table of Contents
Additional information regarding our stock option plans and plan activity for the years ended December 31, 2005, 2004 and 2003 is provided in our consolidated financial statements in this Annual Report on Form 10-K in “Notes to Consolidated Financial Statements, Note 9. Stockholders’ Equity” and is incorporated by reference to the Proxy Statement under the heading “Equity Compensation Plan Information at December 31, 2005” to be distributed in connection with our Annual Meeting of Stockholders to be held on April 12, 2006.
Item 6. Selected Financial Data
The selected financial and operating data presented below should be read in conjunction with “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations” and “Item 8. Financial Statements and Supplemental Data” appearing elsewhere in this Annual Report on Form 10-K. Our statements of operations data for the years ended December 31, 2005, 2004 and 2003, and the balance sheet data at December 31, 2005 and 2004 are derived from, and are qualified by reference to, the audited financial statements included elsewhere in this Annual Report on Form 10-K. The statements of operations data for the years ended December 31, 2002 and 2001 and the balance sheet data at December 31, 2003, 2002 and 2001 are derived from our audited financial statements that do not appear herein. Because of our acquisition of MHA in November 2005 and the consolidated statement of operations for year ended 2005 only include the result of operations of MHA since the date of acquisition, our historical results are not necessarily indicative of our results of operations to be expected in the future.
| Years Ended December 31, |
|||||||||||||||||
| 2005 |
2004 |
2003 |
2002 |
2001 |
|||||||||||||
| (dollars and shares in thousands, except per share data) | |||||||||||||||||
| Consolidated Statements of Operations: |
|||||||||||||||||
| Revenue |
$ | 705,843 | $ | 629,016 | $ | 714,209 | $ | 775,683 | $ | 517,794 | |||||||
| Cost of revenue |
535,608 | 484,654 | 552,052 | 586,900 | 388,284 | ||||||||||||
| Gross profit |
170,235 | 144,362 | 162,157 | 188,783 | 129,510 | ||||||||||||
| Operating expenses: |
|||||||||||||||||
| Selling, general and administrative, excluding non-cash stock-based compensation |
117,184 | 101,436 | 92,500 | 97,666 | 71,483 | ||||||||||||
| Non-cash stock-based compensation(1) |
142 | 750 | 874 | 874 | 31,881 | ||||||||||||
| Depreciation and amortization |
6,179 | 5,837 | 4,819 | 3,839 | 7,713 | ||||||||||||
| Transaction costs(2) |
— | — | — | 139 | 1,955 | ||||||||||||
| Total operating expenses |
123,505 | 108,023 | 98,193 | 102,518 | 113,032 | ||||||||||||
| Income from operations |
46,730 | 36,339 | 63,964 | 86,265 | 16,478 | ||||||||||||
| Other expense (income), net: |
|||||||||||||||||
| Interest expense (income), net |
9,565 | 8,440 | 2,303 | (343 | ) | 13,933 | |||||||||||
| Loss on extinguishment of debt |
— | — | — | — | 8,265 | ||||||||||||
| Total other expense (income), net |
9,565 | 8,440 | 2,303 | (343 | ) | 22,198 | |||||||||||
| Income (loss) before income taxes |
37,165 | 27,899 | 61,661 | 86,608 | (5,720 | ) | |||||||||||
| Income tax expense (benefit) |
14,931 | 10,553 | 23,869 | 34,252 | (1,334 | ) | |||||||||||
| Net income (loss) |
$ | 22,234 | $ | 17,346 | $ | 37,792 | $ | 52,356 | $ | (4,386 | ) | ||||||
| Net income (loss) per common share: |
|||||||||||||||||
| Basic |
$ | 0.76 | $ | 0.61 | $ | 1.04 | $ | 1.23 | $ | (0.14 | ) | ||||||
| Diluted |
$ | 0.69 | $ | 0.55 | $ | 0.95 | $ | 1.12 | $ | (0.14 | ) | ||||||
| Weighted average common shares outstanding: |
|||||||||||||||||
| Basic |
29,130 | 28,248 | 36,456 | 42,534 | 30,641 | ||||||||||||
| Diluted |
32,118 | 31,369 | 39,785 | 46,805 | 30,641 | ||||||||||||
21
Table of Contents
| (1) | Non-cash stock-based compensation represents compensation expense related to our stock option plans to reflect the difference between the fair market value and the exercise price of stock options previously issued to our officers. See “Item 8. Financial Statements and Supplementary Data—Notes to Consolidated Financial Statements—Note 9.” |
| (2) | Transaction costs represent costs incurred in connection with our initial public offering in 2001, and our acquisition of Healthcare Resource Management Corporation in 2002. |
| As of December 31, | |||||||||||||||
| 2005 |
2004 |
2003 |
2002 |
2001 | |||||||||||
| (dollars in thousands) | |||||||||||||||
| Consolidated Balance Sheet Data: |
|||||||||||||||
| Cash, cash equivalents and short term investments |
$ | 19,110 | $ | 3,908 | $ | 4,687 | $ | 40,135 | $ | 31,968 | |||||
| Total assets |
618,387 | 286,960 | 304,532 | 348,774 | 308,929 | ||||||||||
| Total long-term debt, including current portion |
205,000 | 101,723 | 138,900 | — | — | ||||||||||
| Total stockholders’ equity |
193,200 | 136,776 | 116,097 | 295,824 | 271,905 | ||||||||||
22
Table of Contents
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The following discussion should be read in conjunction with, and is qualified in its entirety by, our consolidated financial statements and the notes thereto and other financial information included elsewhere in this Annual Report on Form 10-K. Certain statements in this “Management’s Discussion and Analysis of Financial Condition and Results of Operations” are “forward-looking statements.” See “Special Note Regarding Forward-Looking Statements” below.
Overview
We are the largest temporary healthcare staffing company in the United States. As the leading nationwide provider of travel nurse staffing services and a leading provider of locum tenens (temporary physician staffing) and physician permanent placement services, we recruit physicians, nurses, and allied healthcare professionals, our “healthcare professionals”, nationally and internationally and place them on variable lengths of assignments and in permanent positions at acute-care hospitals, physician groups and other healthcare facilities throughout the United States. With the acquisition of The MHA Group, Inc., and its subsidiaries (“MHA”) on November 2, 2005, we expanded our service lines to include temporary and permanent physician staffing and clearly distinguished AMN as the largest healthcare staffing company.
For the year ended December 31, 2005, we recorded revenue of $705.8 million, as compared to revenue of $629.0 million and $714.2 million for the years ended December 31, 2004 and 2003, respectively. We recorded net income of $22.2 million for the year ended December 31, 2005, as compared to net income of $17.3 million and $37.8 million for the years ended December 31, 2004 and 2003, respectively.
Both our temporary healthcare staffing services and permanent placement services are marketed to two distinct customer bases: (1) healthcare professionals and (2) hospitals, healthcare facilities and physician practice group clients. We use distinct brands to market our differentiated services throughout the healthcare staffing spectrum.
We use a multi-brand recruiting strategy to enhance our ability to successfully attract nursing and allied healthcare professionals in the United States and internationally. We market our nurse and allied healthcare professional staffing to our healthcare professionals under recruitment brands including American Mobile Healthcare, Medical Express, NurseChoice InDemand, NursesRx, Preferred Healthcare Staffing, Thera Tech Staffing, Med Travelers, RN Demand, and O’Grady Peyton International. Each brand has distinct clinician focus, market strengths and brand reputation. We market our travel nursing services to hospitals and healthcare facilities under one brand, AMN Healthcare, as a single staffing provider with access to healthcare professionals from several recruitment brands. We market allied services to our clients under the brand names Thera Tech Staffing and Med Travelers, and we market long-term nursing services to our clients under the brand name O’Grady Peyton International. We market our locum tenens and physician permanent placement services under the brand names Staff Care, Inc. and Merritt, Hawkins & Associates, respectively, to both healthcare professionals and hospital and healthcare facilities and physician staffing groups.
Physicians, nurses and allied healthcare professionals join us on temporary assignments for a wide variety of reasons that include: seeking flexible work opportunities, exploring different areas of the country, building their clinical skills and resume by working at prestigious healthcare facilities, escaping the demands and political environment of working as a permanent staff and working through life and career transitions.
Our large number of hospital and healthcare facility clients provides us with the opportunity to offer temporary or permanent positions in all 50 states and in a variety of work environments and clinical settings. In addition, we provide our temporary healthcare professionals with an attractive benefits package that may include free or subsidized housing, free or reimbursed travel, competitive wages, professional development opportunities, a 401(k) plan, and health and professional liability insurance. We believe that we attract temporary healthcare
23
Table of Contents
professionals due to our long-standing reputation for providing a high level of service, our numerous job opportunities, our benefit packages, our innovative marketing programs and word-of-mouth referrals from our thousands of current and former temporary healthcare professionals.
Our clients include hospitals and healthcare systems such as Georgetown University Hospital, HCA, NYU Medical Center, Stanford Health Care, UCLA Medical Center and The University of Chicago Hospitals. We also provide services to military facilities, sub-acute healthcare facilities, physician practice groups, dialysis centers, clinics and schools.
Our hospital and healthcare facility clients utilize our services to cost-effectively manage shortages in their staff due to a variety of circumstances, such as attrition, the Family Medical Leave Act (FMLA), new unit openings, seasonal patient census variations and other short-term, long-term and permanent staffing needs. In addition to providing continuity of care and quality patient care, we believe hospitals and healthcare facilities contract with us due to our high-quality temporary healthcare professionals, our ability to meet their specific staffing needs, our flexible staffing assignment lengths, our reliable and deep infrastructure, our superior customer service, our ability to offer a large national network of temporary healthcare professionals, and our ability to provide temporary staffing solutions while we assist the facility in filling permanent staffing needs.
We completed secondary offerings of our common stock for 2,300,000 and 10,631,303 shares on April 18, 2005 and May 27, 2005, respectively. All of the 12,931,303 shares were sold by affiliates of Haas Wheat & Partners, L.P. (the “HWP Stockholders”), a private equity investment firm whose affiliates had owned shares of the company since 1999.
On November 2, 2005, we completed the acquisition of The MHA Group, Inc., a Texas corporation, and subsidiaries (“MHA”). MHA, through its wholly-owned subsidiaries, provides temporary physician, nurse and allied healthcare staffing services and physician and allied healthcare permanent placement services. The purchase price is comprised of $160.0 million of initial consideration plus acquisition costs of $2.7 million and an earn-out payment of $47.3 million based on MHA’s financial performance for the twelve months ended December 31, 2005, which was paid by March 10, 2006. The initial $160.0 million of consideration and the earn-out payment were paid approximately 75% in cash and 25% in unregistered shares of the Company’s common stock, par value $0.01 per share. At the closing of the acquisition of MHA, we issued 2.3 million shares of common stock and issued an additional 0.7 million shares on March 9, 2006 for payment of the earn-out amounts.
In connection with the acquisition, we amended our existing credit facility. Our amended and restated credit facility (“The Second Amended and Restated Credit Agreement” or “New Credit Agreement”) provides for, among other things, a $75 million secured revolving credit facility, a $30 million letter of credit sub-facility, a $15 million swing-line sub-facility, all maturing in November 2010, and a new $205 million secured term loan facility maturing in November 2011. The new secured term loan facility was used to pay off existing borrowings of $87.8 million of term debt and provide financing for the acquisition and related transaction costs. We wrote off $1.2 million of deferred financing costs, net of accumulated amortization, as a result of the refinancing and incurred financing costs in connection with the New Credit Agreement of $4.8 million, which will be amortized over the term of the New Credit Agreement. The six year, $205 million, term loan portion of our New Credit Agreement is subject to quarterly amortization of principal with an amount equal to 1.25% of the initial aggregate principal amount of the facility payable quarterly through September 30, 2007 (except in the case of the initial quarterly payment on June 30, 2006 of 2.5%) and 2.5% of the initial aggregate principal amount of the facility payable quarterly from December 31, 2007 through December 31, 2010 with any remaining amounts payable in 2011. These quarterly payments begin on June 30, 2006 with an initial payment of $5.1 million.
Recent Trends
It is estimated that from 1997 through 2005, the temporary healthcare staffing industry grew at a compound annual growth rate of approximately 9%, growing each year except 2003 and 2004 in which the industry declined
24
Table of Contents
on an annual basis. During the decline, the locum tenens market was estimated to have grown by approximately 17% and 11% in 2003 and 2004, respectively, while the travel nursing staffing market was estimated to have declined by approximately 9% in 2003 and 2004. It is estimated that from 2004 to 2005, the locum tenens and travel nurse staffing markets grew by approximately 12% and 1%, respectively, as compared to the overall temporary healthcare industry growth rate of approximately 2.5%. We believe that the growth of the locum tenens market reflects the growing physician shortage, the relative immaturity of the market for temporary physicians, and the financial justification for use of temporary physicians by hospitals and healthcare facilities to generate incremental revenue.
The temporary healthcare staffing industry is expected to grow by approximately 5% in 2006. We believe that this expected growth is based on favorable economic conditions and an increase in hospital staff job openings and turnover. While this growth is positive and is expected to expand the opportunities available to healthcare professionals, the available supply of professionals is not expected to keep pace with the increase in demand.
Critical Accounting Principles and Estimates
We have identified the following critical accounting policies that affect the more significant judgments and estimates used in the preparation of our consolidated financial statements. The preparation of our financial statements in conformity with accounting principles generally accepted in the United States of America requires us to make estimates and judgments that affect our reported amounts of assets and liabilities, revenue and expenses, and related disclosures of contingent assets and liabilities. On an on going basis, we evaluate our estimates, including those related to asset impairment, accruals for self-insurance and compensation and related benefits, allowance for doubtful accounts and contingencies and litigation. These estimates are based on the information that is currently available to us and on various other assumptions that we believe to be reasonable under the circumstances. Actual results could vary from these estimates under different assumptions or conditions.
We believe that the following critical accounting policies affect the more significant judgments and estimates used in the preparation of our consolidated financial statements:
1) Goodwill and Intangible Assets
We have recorded goodwill resulting from our past acquisitions. Commencing with the adoption of Statement of Financial Accounting Standards (“SFAS”) No. 142, Goodwill and Other Intangible Assets, on January 1, 2002, we ceased amortizing goodwill and have performed annual impairment analyses to assess the recoverability of the goodwill and intangible assets, in accordance with the provisions of SFAS No. 142. Upon our annual impairment analyses on December 31, 2005 and December 31, 2004, we determined that there was no impairment of goodwill and intangible assets. If we are required to record an impairment charge in the future, it could have an adverse impact on our results of operations. As of December 31, 2005 and December 31, 2004, we had $240.8 million and $135.4 million, respectively, of goodwill, net of accumulated amortization, and $121.2 million and $3.5 million, respectively, of intangible assets recorded on our consolidated balance sheets. The increase in goodwill and intangible assets is primarily due to our acquisition of MHA in November 2005.
2) Professional Liability Reserve
We maintain an accrual for professional liability self-insured retention limits, net of our insurance recoverable, which is included in accounts payable and accrued expenses and other long term liabilities in our consolidated balance sheets. We determine the adequacy of this accrual by evaluating our historical experience and trends, loss reserves established by our insurance carriers and third party administrators, as well as through the use of independent actuarial studies. We obtain updated actuarial studies on a regular basis that use actual claims data to determine the appropriate reserves for
25
Table of Contents
incurred, but not reported, professional liability claims for each year. As of December 31, 2005 and December 31, 2004, we had $13.9 million and $7.0 million, respectively, accrued for professional liability retention of which $1.9 and $2.2 was classified as a current liability, respectively. The increase in the professional liability accrual was primarily related to the accrual added as a result of the acquisition of MHA, offset by payments made for claims related to prior periods.
3) Self-Insured Health Insurance Claims Reserve
We maintain an accrual for incurred, but not reported, claims arising from self-insured health benefits we provide to our temporary nurse and allied healthcare professionals, which is included in accrued compensation and benefits in our consolidated balance sheets. We determine the adequacy of this accrual by evaluating our historical experience and trends related to both health insurance claims and payments, information provided to us by our insurance broker and third party administrator and industry experience and trends. If such information indicates that our accruals are overstated or understated, we reduce or provide for additional accruals. Our accrual at December 31, 2005 was based on (i) a monthly average of our actual historical health insurance claim amounts and (ii) the average period of time from the date the claim is incurred to the date that it is reported to us and paid. We believe this is the best estimate of the amount of incurred, but not reported, self-insured health benefit claims at year-end. As of December 31, 2005 and December 31, 2004, we had $2.4 million and $2.3 million, respectively, accrued for incurred, but not reported, health insurance claims. The increase in the accrual was primarily related to an increase in the average number of temporary healthcare professionals on assignment. Historically, our accrual for health insurance has been adequate to provide for incurred claims and has fluctuated with increases or decreases in the average number of temporary healthcare professionals on assignment, changes in our claims experience and changes in the reporting and processing time for claims.
4) Workers Compensation Reserve
We maintain an accrual for workers compensation self-insured retention limits, which is included in accrued compensation and benefits and other long term liabilities in our consolidated balance sheets. We determine the adequacy of these accruals by evaluating our historical experience and trends, loss reserves established by our insurance carriers and third party administrators, as well as through the use of independent actuarial studies. We obtain updated actuarial studies on a semi-annual basis that use actual claims data to determine the appropriate reserve both for reported claims and incurred, but not reported, claims for each policy year. The actuarial study for workers compensation provides us with the estimated losses for prior policy years and an estimated percentage of payroll compensation to be accrued for the current year. We record our accruals based on the amounts provided in the actuarial study, and we believe this is the best estimate of our liability for reported claims and incurred, but not reported, claims. As of December 31, 2005 and December 31, 2004, we had $10.1 million and $8.1 million, respectively, accrued for workers compensation claims, of which $3.0 million and $2.7 million was classified as a current liability, respectively. The increase is due to the fact that claim payments made against the reserve during 2005 for the current and prior years lagged behind the additions to the reserve as reserves continue to remain outstanding for workers compensation claims incurred during the course of the last four years. We have recently experienced a slight decrease in workers compensation rates based on recent favorable historical claims experience that slightly offsets these increases.
5) Allowance for Doubtful Accounts
We maintain an allowance for doubtful accounts for estimated credit losses resulting from collection risks, including the inability of our customers to make required payments. This results in a provision for bad debt expense. The allowance for doubtful accounts is reported as a reduction of accounts
26
Table of Contents
receivable in our consolidated balance sheets. We determine the adequacy of this allowance by evaluating the credit risk for individual customer receivables, considering the financial condition of each customer and historical payment trends, delinquency trends, credit histories of customers and current economic conditions. If the financial condition of our customers were to deteriorate, resulting in an impairment of their ability to make payments, additional allowances would be provided. As of December 31, 2005 and December 31, 2004, our allowance for doubtful accounts was $2.4 million and $1.7 million, respectively. The increase was primarily related to the increase in accounts receivable resulting from the acquisition of MHA. The MHA allowance for doubtful accounts of $0.5 million represents the reserve on new receivables generated from the acquisition date through December 31, 2005.
6) Contingent Liabilities
We are subject to various claims and legal actions in the ordinary course of our business. Some of these matters include payroll and employee-related matters and investigations by governmental agencies regarding our employment practices. As we become aware of such claims and legal actions, we provide accruals if the exposures are probable and estimable. If an adverse outcome of such claims and legal actions is reasonably possible, we assess materiality and provide disclosure, as appropriate. We may also become subject to claims, governmental inquiries and investigations and legal actions relating to services provided by our temporary healthcare professionals, and we maintain accruals for these matters if the amounts are probable and estimable. We are currently not aware of any such pending or threatened litigation that would be considered reasonably likely to have a material adverse effect on our consolidated financial position, results of operations or liquidity.
Results of Operations
The following table sets forth, for the periods indicated, certain statements of operations data as a percentage of revenue. Our results of operations include a nurse and allied healthcare staffing segment and a physician staffing segment. We completed our acquisition of MHA in November 2005, therefore the consolidated statement of operations for the year ended December 31, 2005 only includes the results of operations of MHA and the physician staffing segment since the date of acquisition. Accordingly, reporting segment information would not be meaningful, and our historical results are not necessarily indicative of our results of operations to be expected in the future.
| Years Ended December 31, |
|||||||||
| 2005 |
2004 |
2003 |
|||||||
| Consolidated Statements of Operations: |
|||||||||
| Revenue |
100.0 | % | 100.0 | % | 100.0 | % | |||
| Cost of revenue |
75.9 | 77.0 | 77.3 | ||||||
| Gross profit |
24.1 | 23.0 | 22.7 | ||||||
| Selling, general and administrative, excluding non-cash stock-based compensation |
16.6 | 16.1 | 13.0 | ||||||
| Non-cash stock-based compensation |
0.0 | 0.1 | 0.1 | ||||||
| Depreciation and amortization |
0.9 | 1.0 | 0.7 | ||||||
| Income from operations |
6.6 | 5.8 | 8.9 | ||||||
| Interest expense (income), net |
1.3 | 1.3 | 0.3 | ||||||
| Income before income taxes |
5.3 | 4.5 | 8.6 | ||||||
| Income tax expense |
2.1 | 1.7 | 3.3 | ||||||
| Net income |
3.2 | % | 2.8 | % | 5.3 | % | |||
Comparison of Results for the Year Ended December 31, 2005 to the Year Ended December 31, 2004 .
Revenue. Revenue increased 12%, to $705.8 million for 2005 from $629.0 million for 2004. Of the $76.8 million increase, $53.3 million was attributable to the acquisition of MHA in November 2005, $14.6 million was attributable to the increase in the average number of temporary healthcare professionals on
27
Table of Contents
assignment, $6.2 million was attributable to the increase in revenue generated per traveler due primarily to an increase in the average bill rates charged to hospital and healthcare facility clients, and $4.5 million was attributable to a shift in the mix from flat rate contracts to hours and days worked contracts. The increase was partially offset by one less day in 2005 which reduced revenue by $1.8 million.
Cost of Revenue. Cost of revenue increased 11%, to $535.6 million for 2005 from $484.7 million for 2004. Of the $50.9 million increase, $36.5 million was attributable to the acquisition of MHA in November 2005, $11.3 million was attributable to the increase in the average number of temporary healthcare professionals on assignment, $0.9 million was attributable to net increases in compensation provided to our temporary healthcare professionals, $3.6 million was attributable to the shift in the mix from flat rate contracts to hours and days worked contracts, and partially offset by a decrease of $1.4 million attributable to one less day in 2005.
Gross Profit. Gross profit increased 18%, to $170.2 million for 2005 from $144.4 million for 2004, representing gross margins of 24.1% and 23.0%, respectively. The increase in gross margin was primarily attributable to an increase in the spread between bill rates and pay rates and the addition of the higher gross margin in the physician staffing segment through the acquisition of MHA in November 2005.
Selling, General and Administrative Expenses. Selling, general and administrative expenses, excluding non-cash stock-based compensation, increased 16%, to $117.2 million for 2005 from $101.4 million for 2004. Of the $15.8 million increase, $11.7 million was attributable to the acquisition of MHA in November 2005, with the remaining $4.1 million increase primarily attributable to increases in employee expenses from a combination of normal growth in costs per employee and selective headcount additions, partially offset by decreases in professional liability insurance and professional services costs.
Non-Cash Stock-Based Compensation. We recorded non-cash compensation charges of $0.1 million in 2005 and $0.8 million in 2004 in connection with our stock option plans to reflect the difference between the fair market value at the measurement date and the exercise prices of previously issued stock options, which are amortized over their respective vesting periods. The decrease relates to the cancellation and completed vesting of previously issued stock options issued at exercise prices below fair market value.
Amortization and Depreciation. Amortization expense was $0.6 million in 2005 and $0.2 million in 2004. The increase was primarily attributable to the amortization of identifiable amortizable intangible assets obtained from the acquisition of MHA in November 2005. Depreciation expense of $5.6 million was consistent for 2005 and 2004.
Interest Expense, Net. Interest expense, net, was $9.6 million for 2005 as compared to $8.4 million for 2004. The increase was primarily due to a $1.2 million write-off of deferred financing costs from the refinancing of our credit facility in connection with the acquisition of MHA in November 2005.
Income Tax Expense. Income tax expense increased to $14.9 million for 2005 from $10.6 million for 2004, reflecting effective income tax rates of 40.2% and 37.8% for these periods, respectively. The increase in the effective income tax rate was primarily attributable to increases in the state tax provision.
Comparison of Results for the Year Ended December 31, 2004 to the Year Ended December 31, 2003
Revenue. Revenue decreased 12%, to $629.0 million for 2004 from $714.2 million for 2003. This decrease is comparable to the decrease in the number of temporary healthcare professionals on assignment, which decreased 12% to an average of 6,225 for 2004 from 7,113 for 2003. Of the $85.2 million decrease, $89.3 million was attributable to the decline in the average number of temporary healthcare professionals on assignment and $2.6 million was attributable to a shift in the mix from hours and days worked contracts to flat rate contracts. These decreases were partially offset by improvements in contract terms, which included increases in bill rates charged to hospital and healthcare facility clients, of approximately $5.0 million, and the additional day from leap year in 2004, which contributed $1.7 million.
28
Table of Contents
Cost of Revenue. Cost of revenue decreased 12%, to $484.7 million for 2004 from $552.1 million for 2003. Of the $67.4 million decrease, $69.1 million was attributable to the decline in the average number of temporary healthcare professionals on assignment, partially offset by an increase of $0.4 million attributable to net increases in compensation provided to our temporary healthcare professionals and by an increase of $1.3 million attributable to the extra day in 2004.
Gross Profit. Gross profit decreased 11%, to $144.4 million for 2004 from $162.2 million for 2003, representing gross margins of 23.0% and 22.7%, respectively. The increase in gross margin was primarily attributable to decreased health insurance, housing and retirement costs as a percentage of revenue, partially offset by increases in compensation provided to our temporary healthcare professionals.
Selling, General and Administrative Expenses. Selling, general and administrative expenses, excluding non-cash stock-based compensation, increased 10%, to $101.4 million for 2004 from $92.5 million for 2003. The $8.9 million increase was primarily attributable to an increase in expenses related to corporate facilities as we occupied a larger corporate facility for a full year compared to a half year in 2003 and corporate employee and professional services increases related to additional compliance requirements in connection with the Sarbanes-Oxley Act of 2002. In addition, we recorded an increase in our professional liability insurance reserve as we have experienced negative trends in our malpractice claims development. These increases were partially offset by a $1.2 million charge in the fourth quarter of 2003 related to vested stock options purchased in our October 2003 tender offer that was not incurred during 2004.
Non-Cash Stock-Based Compensation. We recorded non-cash compensation charges of $0.8 million in 2004 and $0.9 million in 2003 in connection with our stock option plans to reflect the difference between the fair market value at the measurement date and the exercise prices of previously issued stock options, which are amortized over their respective vesting periods.
Amortization and Depreciation. Amortization expense was $0.2 million in 2004 and $0.4 million in 2003. Depreciation expense increased to $5.6 million for 2004 from $4.4 million for 2003. This increase was primarily attributable to internally developed software placed into service in 2004 and 2003 and additions of leasehold improvements and assets acquired in connection with the consolidation of several San Diego, California locations into a new corporate headquarters facility during the second half of 2003.
Interest Expense, Net. Interest expense, net, was $8.4 million for 2004 as compared to $2.3 million for 2003, due primarily to interest charges related to borrowings initiated under our credit facility in October 2003 to fund our tender offer and the amortization of deferred financing costs associated with those borrowings. In addition, interest expense was also higher due to the write-off of $0.5 million of deferred financing costs during 2004 related to $24.3 million in voluntary prepayments on our long-term debt.
Income Tax Expense. Income tax expense decreased to $10.6 million for 2004 from $23.9 million for 2003, reflecting effective income tax rates of 37.8% and 38.7% for these periods, respectively. The reduction in the effective income tax rate was primarily attributable to changes in the state tax provision in 2004.
Liquidity and Capital Resources
Historically, our primary liquidity requirements have been for acquisitions, working capital requirements and debt service under our credit facility. We have funded these requirements through internally generated cash flow and funds borrowed under our credit facility. At December 31, 2005, $205 million was outstanding under our credit facility. We believe that cash generated from operations and available borrowings under our revolving credit facility will be sufficient to fund our operations for the next 12 months. We expect to be able to finance future acquisitions either with cash provided from operations, borrowings under our revolving credit facility, bank loans, debt or equity offerings, or some combination of the foregoing. The following discussion provides further details of our liquidity and capital resources.
29
Table of Contents
Operating Activities:
Historically, our principal working capital need has been for accounts receivable. At December 31, 2005 and December 31, 2004, our Days Sales Outstanding (“DSO”) was 57 days and 63 days, respectively. Excluding the impact of the acquisition of MHA, DSO was 59 days at December 31, 2005. The decrease in DSO was related to the acquisition of MHA in November 2005, which historically has lower DSO than AMN, as well as improvements in billing and collection processes. Our principal sources of cash to fund our working capital needs are cash generated from operating activities and borrowings under our revolving credit facility. Net cash provided by operations increased $5.1 million to $44.1 million in 2005 from $39.0 million in 2004. This increase in net cash provided by operations was driven by increased earnings compared to fiscal 2004 and the tax effects of temporary differences that give rise to significant portions of deferred income taxes.
Investing Activities:
We continue to have relatively low capital investment requirements. Capital expenditures were $3.8 million, $5.1 million and $13.0 million in 2005, 2004 and 2003, respectively. In 2005, our capital expenditures were $3.0 million for purchased and internally developed software, $0.8 million for computers, furniture and equipment, leasehold improvements and other expenditures. The higher level of capital expenditures in 2003 was primarily related to leasehold improvements for our new corporate headquarters. We expect our future capital expenditure requirements to be similar to 2005, in relation to revenue.
Our business acquisition expenditures were $111.5 million in 2005 compared to $0 in 2004 and 2003. Our 2005 expenditures were primarily related to our acquisition of MHA in November 2005. This acquisition was financed through a combination of bank debt, cash provided by operations and AMN common stock.
Financing Activities:
On November 2, 2005, we acquired MHA for an initial purchase price of $160.0 million plus acquisition costs of $2.7 million, and an earn-out payment of $47.3 million of additional consideration based on the twelve months ended December 31, 2005 performance of MHA. The initial $160.0 million of consideration and the earn-out payment were paid approximately 75% in cash and 25% in unregistered shares of the Company’s common stock. We paid $35.9 million in cash and issued 0.7 million shares of stock by March 10, 2006 related to the earn-out. In addition, as part of the acquisition, $15.0 million of the initial consideration was held back for possible contingencies. As of December 31, 2005, $0.4 million of the $15.0 million was paid to the selling shareholders, with the balance due in March 2007, net of any indemnification claims.
In connection with the acquisition, we amended and restated our existing credit facility. Our new credit facility, the Second Amended and Restated Credit Agreement (“New Credit Agreement”), provides for, among other things, a $75.0 million secured revolving credit facility, a $30.0 million letter of credit sub-facility, a $15.0 million swing-line sub-facility, all maturing in November 2010, and a new $205.0 million secured term loan facility maturing in November 2011. The new secured term loan facility was used to pay off existing borrowings of $87.8 million of term debt and provide financing for the cash portion of the initial $145.0 million of consideration, net of the $15.0 million holdback, and related acquisition and financing costs of $2.7 million and $4.8 million, respectively. We funded the $35.9 million cash portion of the earn-out payment on March 10, 2006 with cash on hand and borrowings under our revolving credit facility.
The revolving credit facility portion of our New Credit Agreement carries an unused fee of between 0.5% and 0.375% per annum based on our current leverage ratio, and there are no mandatory reductions in the revolving commitment under the revolving credit facility. Borrowings under this revolving credit facility bear interest at floating rates based upon either a LIBOR or a prime interest rate option selected by us, plus a spread of 1.50% to 2.25% and 0.50% to 1.25%, respectively, to be determined based on our current leverage ratio. Amounts available under our revolving credit facility may be used for working capital, capital expenditures, permitted acquisitions and general corporate purposes, subject to various limitations.
30
Table of Contents
The six year, $205 million term loan portion of our New Credit Agreement is subject to quarterly amortization of principal (in equal installments), with an amount equal to 1.25% of the initial aggregate principal amount of the facility payable quarterly through September 30, 2007 (except in the case of the initial quarterly payment on June 30, 2006 of 2.5%) and 2.5% of the initial aggregate principal amount of the facility payable quarterly from December 31, 2007 through September 30, 2010 with any remaining amounts payable in 2011. These quarterly payments begin on June 30, 2006 with an initial payment of $5.1 million. Voluntary prepayments of the term loan portion of the credit facility are applied as we may elect, including ratably to the remaining quarterly amortization payments. Borrowings under this term loan facility bear interest at floating rates based upon either a LIBOR or a prime interest rate option selected by us, plus a spread of 1.75% or 2.00% and 0.75% or 1.00%, respectively, to be determined based on our current leverage ratio.
We are required to make additional mandatory prepayments on the term loan with the proceeds of asset dispositions, extraordinary receipts, debt issuances and certain equity issuances. We also are required to make mandatory prepayments on the term loan within ninety days after the end of each fiscal year, commencing with the fiscal year ended December 31, 2006 in an amount equal to 50% of our excess cash flow (as defined in the Second Amended and Restated Credit Agreement), less any voluntary prepayments made during the fiscal year. These mandatory prepayment amounts, if any, are applied ratably to the remaining quarterly amortization payments.
We are required to maintain a maximum leverage ratio as of the end of each fiscal quarter of not more than 3.75 to 1.00 for the fiscal quarter ending December 31, 2005, decreasing throughout the term of the agreement to ultimately arrive at a ratio of 2.00 to 1.00 for the fiscal quarter ending March 31, 2009 and thereafter. We are also required to maintain a minimum fixed charge coverage ratio as of the end of each fiscal quarter of not less than 2.00 to 1.00 for the fiscal quarter ending December 31, 2005, decreasing throughout the term of the agreement to ultimately arrive at a ratio of 1.25 to 1.00 for the fiscal quarter ending September 30, 2008 and thereafter. We are also subject to limitations on the amount of our annual capital expenditures and on the amount of consolidated total assets and consolidated EBITDA that may be owned or attributable to our foreign subsidiaries. We were in compliance with these requirements at December 31, 2005.
Under our New Credit Agreement, our subsidiaries are not permitted to pay dividends or distributions to us, except for certain permitted dividends and distributions, including those related to taxes, certain reporting obligations under federal and state law and certain other ordinary course operating expenses, subject to the limitations contained in our New Credit Agreement.
We are also required to maintain interest rate protection on at least 50% of the term loan portion of our New Credit Agreement beginning May 2006 until November 2008. In October 2003, we entered into an interest rate swap agreement to minimize our exposure to interest rate fluctuations on the first $30 million of our outstanding variable rate debt under our existing credit facility whereby we pay a fixed rate of 2.65% and receive a floating three-month LIBOR. This agreement expires in September 2006, and no initial investment was made to enter into this agreement.
In June 2005, we entered into two additional interest rate swap agreements. The first agreement has a notional amount of $20 million and became effective in September 2005, whereby we pay a fixed rate of 3.99% and receive a floating three-month LIBOR. The agreement expires in March 2007. The second agreement will become effective in September 2006, with a notional amount of $15 million, whereby we pay a fixed rate of 4.09% and receive a floating three-month LIBOR. This agreement will expire in September 2007.
In November 2005, we entered into five additional interest rate swap agreements for notional amounts of $15 million, $10 million, $30 million, $35 million and $50 million, whereby we pay a fixed rate of 4.82%, 4.95%, 4.87%, 4.94%, and 4.97%, respectively, and receive a floating three-month LIBOR. These agreements expire in December 2007, June 2008, December 2008, December 2009 and December 2010, respectively.
At December 31, 2005 and 2004, the interest rate swap agreements had a fair value of ($0.1) million and $0.7 million, respectively, which is included in other assets and liabilities in the accompanying consolidated
31
Table of Contents
balance sheets. We have formally documented the hedging relationships and account for these arrangements as cash flow hedges.
As of December 31, 2005 and 2004, our existing credit facility also served to collateralize certain letters of credit aggregating $9.6 million and $7.2 million, respectively, issued by us in the normal course of business.
Contractual Obligations
The following table summarizes our contractual obligations as of December 31, 2005 (in thousands):
| Fiscal Year | |||||||||||||||||||||
| 2006 |
2007 |
2008 |
2009 |
2010 |
Thereafter |
Total | |||||||||||||||
| Long-term debt (1) |
$ | 23,363 | $ | 25,218 | $ | 31,854 | $ | 30,489 | $ | 54,781 | $ | 97,916 | $ | 263,621 | |||||||
| Capital lease obligations (2) |
494 | 493 | 479 | 464 | 158 | — | 2,088 | ||||||||||||||
| Operating lease obligations (3) |
16,327 | 17,820 | 17,417 | 17,389 | 17,149 | 85,102 | 171,204 | ||||||||||||||
| Earn-out payable in cash (4) |
35,879 | — | — | — | — | — | 35,879 | ||||||||||||||
| Cash holdback (5) |
2,362 | 12,238 | — | — | — | — | 14,600 | ||||||||||||||
| Total contractual obligations |
$ | 78,425 | $ | 55,769 | $ | 49,750 | $ | 48,342 | $ | 72,088 | $ | 183,018 | $ | 487,392 | |||||||
| (1) | Amounts represent contractual amounts due, including interest. |
| (2) | Amounts represent contractual amounts due, including interest, with initial or remaining lease terms in excess of one year. |
| (3) | Amounts represent minimum contractual amounts, with initial or remaining lease terms in excess of one year. We have assumed no escalations in rent or changes in variable expenses other than as stipulated in lease contracts. |
| (4) | Amount represents the earn-out payable in cash in connection with the MHA acquisition. |
| (5) | Amounts represent the cash holdback payable in cash in connection with the MHA acquisition. |
Off-Balance Sheet and Other Financing Arrangements
At December 31, 2005 and 2004, we did not have any relationships with unconsolidated entities or financial partnerships, such as entities often referred to as structured finance, variable interest or special purpose, which would have been established for the purpose of facilitating off-balance-sheet arrangements or other contractually narrow or limited purposes. In addition, we do not engage in trading activities involving non-exchange traded contracts. As such, we are not materially exposed to any financing, liquidity, market or credit risk that could arise if we had engaged in such relationships. We do not have relationships or transactions with persons or entities that derive benefits from their non-independent relationship with us or our related parties other than what is disclosed in “Item 8. Financial Statements and Supplementary Data—Notes to Consolidated Financial Statements—Note 10.”
Potential Fluctuations in Quarterly Results and Seasonality
Due to the regional and seasonal fluctuations in the hospital patient census and nurse staffing needs of our hospital and healthcare facility clients and due to seasonal preferences for destinations of our temporary healthcare professionals, revenue, earnings and the number of temporary healthcare professionals on assignment are subject to moderate seasonal fluctuations. Many of our hospital and healthcare facility clients are located in areas that experience seasonal fluctuations in population during the winter and summer months. These facilities
32
Table of Contents
adjust their staffing levels to accommodate the change in this seasonal demand and many of these facilities utilize temporary healthcare professionals to satisfy these seasonal staffing needs. This historical seasonality of revenue and earnings may vary due to a variety of factors and the results of any one quarter are not necessarily indicative of the results to be expected for any other quarter or for any year.
Inflation
Although inflation has abated during the last several years, the rate of inflation in healthcare related services continues to exceed the rate experienced by the economy as a whole. Our contracts typically provide for an annual increase in the fees paid to us by our clients based on increases in various inflation indices allowing us to pass on inflation costs to our clients.
Recent Accounting Pronouncements
In December 2004, the Financial Accounting Standards Board (“FASB”), issued Statement No. 123 (Revised), Share-Based Payment, (“FAS 123R”), which amends Statement No. 123, Accounting for Stock-Based Compensation, and supersedes Accounting Principles Board (“APB”) Opinion No. 25, Accounting for Stock Issued to Employees. FAS 123R requires the measurement of compensation cost related to all share-based payments to employees, including grants of employee stock options, using a fair-value-based method and the recording of such cost in our consolidated statements of operations. Additionally, FAS 123R requires the estimated forfeitures be considered in determining compensation cost. The accounting provisions of FAS 123R are effective for the first interim or annual reporting period that begins after June 15, 2005. FAS 123R, which provides certain changes to the method for valuing share-based compensation among other changes, will apply to new awards and to awards that are outstanding on the effective date and are subsequently modified or cancelled. Compensation expense for outstanding awards for which the requisite service had not been rendered as of the effective date will be recognized over the remaining service period using the compensation cost calculated for pro forma disclosure purposes under FAS 123R. At December 31, 2005, of the $11.9 million unamortized compensation expense before the effect of income taxes related to outstanding unvested options, as determined in accordance with FAS 123, $5.1 million is expected to be recorded during fiscal 2006. We will likely incur additional expense during 2006 related to new awards granted during 2006 that cannot yet be quantified. We adopted FAS 123R on January 1, 2006 using the modified prospective method and we will value share-based awards granted after the effective date using the Black-Scholes option pricing model, which is consistent with the valuation method previously used for footnote disclosure purposes in accordance with FAS 123.
Special Note Regarding Forward-Looking Statements
This Annual Report on Form 10-K contains “forward-looking statements” within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. We based these forward-looking statements on our current expectations and projections about future events. Our actual results could differ materially from those discussed in, or implied by, these forward-looking statements. Forward-looking statements are identified by words such as “believe,” “anticipate,” “expect,” “intend,” “plan,” “will,” “may” and other similar expressions. In addition, any statements that refer to expectations, projections or other characterizations of future events or circumstances are forward-looking statements. The following factors could cause our actual results to differ materially from those implied by the forward-looking statements in this Annual Report:
| • | our ability to continue to recruit qualified temporary and permanent healthcare professionals at reasonable costs; |
| • | our ability to retain qualified temporary healthcare professionals for multiple assignments at reasonable costs; |
| • | our ability to attract and retain sales and operational personnel; |
33
Table of Contents
| • | our ability to enter into contracts with hospitals, healthcare facility clients, affiliated healthcare networks and physician practice groups on terms attractive to us and to secure orders related to those contracts; |
| • | our ability to demonstrate the value of our services to our healthcare and facility clients; |
| • | changes in the timing of hospital, healthcare facility and physician practice group clients’ orders for temporary healthcare professionals; |
| • | the general level of patient occupancy at our hospital and healthcare facility clients’ facilities; |
| • | the overall level of demand for services offered by temporary and permanent healthcare staffing providers; |
| • | the ability of our hospital, healthcare facility and physician practice group clients to retain and increase the productivity of their permanent staff; |
| • | the variation in pricing of the healthcare facility contracts under which we place temporary healthcare professionals; |
| • | our ability to successfully implement our strategic growth, acquisition and integration strategies; |
| • | our ability to leverage our cost structure; |
| • | the performance of our management information and communication systems; |
| • | the effect of existing or future government legislation and regulation; |
| • | our ability to grow and operate our business in compliance with legislation and regulations; |
| • | the challenge to the classification of certain of our healthcare professionals as independent contractors; |
| • | the impact of medical malpractice and other claims asserted against us; |
| • | the disruption or adverse impact to our business as a result of a terrorist attack; |
| • | our ability to carry out our business strategy and maintain sufficient cash flow and capital structure to support our business; |
| • | the loss of key officers and management personnel that could adversely affect our ability to remain competitive; |
| • | the effect of recognition by us of an impairment to goodwill; and |
| • | the effect of adjustments by us to accruals for self-insured retentions. |
Other factors that could cause actual results to differ from those implied by the forward-looking statements in this Annual Report on Form 10-K are more fully described in the “Risk Factors” section and elsewhere in this Annual Report on Form 10-K. We undertake no obligation to update the forward-looking statements in this filing. References in this Annual Report on Form 10-K to “AMN Healthcare,” the “Company,” “we,” “us” and “our” refer to AMN Healthcare Services, Inc. and its wholly owned subsidiaries.
34
Table of Contents
Item 7A. Quantitative and Qualitative Disclosures about Market Risk
Market risk is the risk of loss arising from adverse changes in market rates and prices, such as interest rates, foreign currency exchange rates and commodity prices.
During 2005 and 2004, our primary exposure to market risk was interest rate risk associated with our debt instruments. See “Item 7. Management’s Discussion and Analysis—Liquidity and Capital Resources—Financing Activities” for further description of our debt instruments and interest rate swaps. Excluding the effect of our interest rate swap arrangements, a 1% change in interest rates on our variable rate debt would have resulted in interest expense fluctuating approximately $1.1 million in 2005 and $1.5 million in 2004.
Our international operations create exposure to foreign currency exchange rate risks. We believe that our foreign currency risk is immaterial.
35
Table of Contents
Item 8. Financial Statements and Supplementary Data
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
36
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders
AMN Healthcare Services, Inc.:
We have audited the accompanying consolidated balance sheets of AMN Healthcare Services, Inc. and subsidiaries (the Company) as of December 31, 2005 and 2004, and the related consolidated statements of operations, stockholders’ equity and comprehensive income, and cash flows for each of the years in the three-year period ended December 31, 2005. These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these consolidated financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of AMN Healthcare Services, Inc. and subsidiaries as of December 31, 2005 and 2004, and the results of their operations and their cash flows for each of the years in the three-year period ended December 31, 2005, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the effectiveness of the Company’s internal control over financial reporting as of December 31, 2005, based on criteria established in Internal Control–Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO), and our report dated March 9, 2006 expressed an unqualified opinion on management’s assessment of, and the effective operation of, internal control over financial reporting.
/s/ KPMG LLP
San Diego, California
March 9, 2006
37
Table of Contents
CONSOLIDATED BALANCE SHEETS
(in thousands, except par value)
| December 31, 2005 |
December 31, 2004 |
|||||||
| ASSETS | ||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 19,110 | $ | 3,908 | ||||
| Accounts receivable, net of allowance of $2,375 and $1,752 at |
154,926 | 108,825 | ||||||
| Prepaid expenses |
12,763 | 11,703 | ||||||
| Income tax receivable |
8,311 | — | ||||||
| Deferred income taxes, net |
31,305 | 1,210 | ||||||
| Other current assets |
1,848 | 1,759 | ||||||
| Total current assets |
228,263 | 127,405 | ||||||
| Fixed assets, net |
20,164 | 17,833 | ||||||
| Deferred income taxes, net |
— | 508 | ||||||
| Deposits and other assets |
7,964 | 2,265 | ||||||
| Goodwill, net |
240,844 | 135,449 | ||||||
| Intangible assets, net |
121,152 | 3,500 | ||||||
| Total assets |
$ | 618,387 | $ | 286,960 | ||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY | ||||||||
| Current liabilities: |
||||||||
| Bank overdraft |
$ | — | $ | 1,093 | ||||
| Accounts payable and accrued expenses |
19,092 | 8,309 | ||||||
| Accrued compensation and benefits |
32,208 | 24,595 | ||||||
| Income taxes payable |
— | 790 | ||||||
| Current portion of notes payable |
10,250 | 4,863 | ||||||
| Deferred revenue |
7,610 | — | ||||||
| Other current liabilities |
59,018 | 351 | ||||||
| Total current liabilities |
128,178 | 40,001 | ||||||
| Notes payable, less current portion |
194,750 | 96,860 | ||||||
| Deferred income taxes, net |
65,132 | — | ||||||
| Other long-term liabilities |
37,127 | 13,323 | ||||||
| Total liabilities |
425,187 | 150,184 | ||||||
| Commitments and contingencies |
||||||||
| Stockholders’ equity: |
||||||||
| Common stock, $0.01 par value; 200,000 shares authorized; 43,747 and 43,221 shares issued at December 31, 2005 and 2004, respectively |
437 | 432 | ||||||
| Additional paid-in capital |
355,762 | 352,456 | ||||||
| Treasury stock, at cost (12,551 and 14,877 shares at December 31, 2005 and 2004, respectively) |
(210,529 | ) | (249,538 | ) | ||||
| Retained earnings |
47,784 | 33,155 | ||||||
| Accumulated other comprehensive income (loss) |
(254 | ) | 271 | |||||
| Total stockholders’ equity |
193,200 | 136,776 | ||||||
| Total liabilities and stockholders’ equity |
$ | 618,387 | $ | 286,960 | ||||
See accompanying notes to consolidated financial statements.
38
Table of Contents
CONSOLIDATED STATEMENTS OF OPERATIONS
(in thousands, except per share amounts)
| Years Ended December 31, | |||||||||
| 2005 |
2004 |
2003 | |||||||
| Revenue |
$ | 705,843 | $ | 629,016 | $ | 714,209 | |||
| Cost of revenue |
535,608 | 484,654 | 552,052 | ||||||
| Gross profit |
170,235 | 144,362 | 162,157 | ||||||
| Operating expenses: |
|||||||||
| Selling, general and administrative, excluding non-cash stock-based compensation |
117,184 | 101,436 | 92,500 | ||||||
| Non-cash stock-based compensation |
142 | 750 | 874 | ||||||
| Depreciation and amortization |
6,179 | 5,837 | 4,819 | ||||||
| Total operating expenses |
123,505 | 108,023 | 98,193 | ||||||
| Income from operations |
46,730 | 36,339 | 63,964 | ||||||
| Interest expense (income), net |
9,565 | 8,440 | 2,303 | ||||||
| Income before income taxes |
37,165 | 27,899 | 61,661 | ||||||
| Income tax expense |
14,931 | 10,553 | 23,869 | ||||||
| Net income |
$ | 22,234 | $ | 17,346 | $ | 37,792 | |||
| Net income per common share: |
|||||||||
| Basic |
$ | 0.76 | $ | 0.61 | $ | 1.04 | |||
| Diluted |
$ | 0.69 | $ | 0.55 | $ | 0.95 | |||
| Weighted average common shares outstanding: |
|||||||||
| Basic |
29,130 | 28,248 | 36,456 | ||||||
| Diluted |
32,118 | 31,369 | 39,785 | ||||||
See accompanying notes to consolidated financial statements.
39
Table of Contents
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY AND COMPREHENSIVE INCOME
Years Ended December 31, 2005, 2004 and 2003
(in thousands)
| Common Stock |
Additional Paid-in Capital |
Treasury Stock |
Retained Earnings (Accumulated Deficit) |
Accumulated Other Comprehensive Income (Loss) |
|||||||||||||||||||||
| Shares |
Amount |
Total |
|||||||||||||||||||||||
| Balance, December 31, 2002 |
42,991 | $ | 430 | $ | 352,541 | $ | (35,164 | ) | $ | (21,983 | ) | $ | — | $ | 295,824 | ||||||||||
| Repurchase of common stock into treasury |
— | — | (3,872 | ) | (214,264 | ) | — | — | (218,136 | ) | |||||||||||||||
| Exercise of stock options |
6 | — | 52 | — | — | — | 52 | ||||||||||||||||||
| Stock-based compensation |
— | — | 874 | — | — | — | 874 | ||||||||||||||||||
| Comprehensive income (loss): |
|||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | (111 | ) | (111 | ) | ||||||||||||||||
| Unrealized loss for derivative financial instruments, net of tax |
— | — | — | — | — | (198 | ) | (198 | ) | ||||||||||||||||
| Net income |
— | — | — | — | 37,792 | — | 37,792 | ||||||||||||||||||
| Total comprehensive income |
37,483 | ||||||||||||||||||||||||
| Balance, December 31, 2003 |
42,997 | 430 | 349,595 | (249,428 | ) | 15,809 | (309 | ) | 116,097 | ||||||||||||||||
| Transaction costs related to 2003 repurchase of common stock into treasury |
— | — | — | (110 | ) | — | — | (110 | ) | ||||||||||||||||
| Exercise of stock options |
224 | 2 | 2,041 | — | — | — | 2,043 | ||||||||||||||||||
| Income tax benefit from stock option exercises |
— | — | 70 | — | — | — | 70 | ||||||||||||||||||
| Stock-based compensation |
— | — | 750 | — | — | — | 750 | ||||||||||||||||||
| Comprehensive income (loss): |
|||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | (8 | ) | (8 | ) | ||||||||||||||||
| Unrealized loss for derivative financial instruments, net of tax |
— | — | — | — | — | 588 | 588 | ||||||||||||||||||
| Net income |
— | — | — | — | 17,346 | — | 17,346 | ||||||||||||||||||
| Total comprehensive income |
17,926 | ||||||||||||||||||||||||
| Balance, December 31, 2004 |
43,221 | 432 | 352,456 | (249,538 | ) | 33,155 | 271 | 136,776 | |||||||||||||||||
| Issuance costs of common stock |
— | — | — | — | (544 | ) | — | (544 | ) | ||||||||||||||||
| Issuance of treasury stock |
— | — | — | 39,009 | (7,061 | ) | — | 31,948 | |||||||||||||||||
| Exercise of stock options |
526 | 5 | 2,855 | — | — | — | 2,860 | ||||||||||||||||||
| Income tax benefit from stock option exercises |
— | — | 309 | — | — | — | 309 | ||||||||||||||||||
| Stock-based compensation |
— | — | 142 | — | — | — | 142 | ||||||||||||||||||
| Comprehensive income (loss): |
|||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | (82 | ) | (82 | ) | ||||||||||||||||
| Unrealized gain for derivative financial instruments, net of tax |
— | — | — | — | — | (443 | ) | (443 | ) | ||||||||||||||||
| Net income |
— | — | — | — | 22,234 | — | 22,234 | ||||||||||||||||||
| Total comprehensive income |
21,709 | ||||||||||||||||||||||||
| Balance, December 31, 2005 |
43,747 | $ | 437 | $ | 355,762 | $ | (210,529 | ) | $ | 47,784 | $ | (254 | ) | $ | 193,200 | ||||||||||
See accompanying notes to consolidated financial statements.
40
Table of Contents
CONSOLIDATED STATEMENTS OF CASH FLOWS
(in thousands)
| Years Ended December 31, |
||||||||||||
| 2005 |
2004 |
2003 |
||||||||||
| Cash flows from operating activities: |
||||||||||||
| Net income |
$ | 22,234 | $ | 17,346 | $ | 37,792 | ||||||
| Adjustments to reconcile net income to net cash provided by operating activities, net of effects from acquisition: |
||||||||||||
| Depreciation and amortization |
6,179 | 5,837 | 4,819 | |||||||||
| Provision for (recovery of) bad debts |
1,738 | 173 | (315 | ) | ||||||||
| Noncash interest expense |
2,747 | 1,449 | 550 | |||||||||
| Provision for deferred income taxes |
19,017 | 4,086 | 6,040 | |||||||||
| Non-cash stock-based compensation |
142 | 750 | 874 | |||||||||
| Stock-based compensation in connection with tender offer |
— | — | 1,128 | |||||||||
| (Gain) loss on disposal or sale of fixed assets |
(9 | ) | 81 | 236 | ||||||||
| Changes in assets and liabilities, net of effects from acquisition: |
||||||||||||
| Accounts receivable |
(474 | ) | 8,394 | 17,379 | ||||||||
| Prepaid expenses and other current assets |
1,829 | 2,792 | (1,800 | ) | ||||||||
| Deposits and other assets |
(1,463 | ) | (370 | ) | (223 | ) | ||||||
| Accounts payable and accrued expenses |
(1,204 | ) | (764 | ) | (2,864 | ) | ||||||
| Accrued compensation and benefits |
560 | (2,423 | ) | (2,411 | ) | |||||||
| Income taxes payable |
(10,467 | ) | (1,152 | ) | 444 | |||||||
| Other liabilities |
3,261 | 2,839 | 3,496 | |||||||||
| Net cash provided by operating activities |
44,090 | 39,038 | 65,145 | |||||||||
| Cash flows from investing activities: |
||||||||||||
| Purchase and development of fixed assets |
(3,818 | ) | (5,061 | ) | (13,013 | ) | ||||||
| Cash paid for acquisitions, net of cash received |
(111,508 | ) | — | — | ||||||||
| Cash paid under deferred purchase agreement |
— | — | (1,000 | ) | ||||||||
| Net cash used in investing activities |
(115,326 | ) | (5,061 | ) | (14,013 | ) | ||||||
| Cash flows from financing activities: |
||||||||||||
| Capital lease repayments |
(364 | ) | (339 | ) | (304 | ) | ||||||
| Proceeds from issuance of notes payable |
205,000 | — | 145,000 | |||||||||
| Payment of financing costs |
(4,904 | ) | (258 | ) | (4,628 | ) | ||||||
| Payments on notes payable |
(107,218 | ) | (37,177 | ) | (6,100 | ) | ||||||
| Repurchase of common stock and options, including transaction costs |
— | (110 | ) | (219,264 | ) | |||||||
| Proceeds from issuance of common stock, net of issuance costs |
2,316 | 2,043 | 52 | |||||||||
| Change in bank overdraft, net of effects of acquisition |
(8,310 | ) | 1,093 | (1,225 | ) | |||||||
| Net cash provided by (used in) financing activities |
86,520 | (34,748 | ) | (86,469 | ) | |||||||
| Effect of exchange rate changes on cash |
(82 | ) | (8 | ) | (111 | ) | ||||||
| Net increase (decrease) in cash and cash equivalents |
15,202 | (779 | ) | (35,448 | ) | |||||||
| Cash and cash equivalents at beginning of year |
3,908 | 4,687 | 40,135 | |||||||||
| Cash and cash equivalents at end of year |
$ | 19,110 | $ | 3,908 | $ | 4,687 | ||||||
| Supplemental disclosures of cash flow information: |
||||||||||||
| Cash paid for interest (net of $39, $32 and $0 capitalized in 2005, 2004 and 2003, respectively) |
$ | 7,070 | $ | 7,354 | $ | 2,003 | ||||||
| Cash paid for income taxes |
$ | 6,354 | $ | 7,584 | $ | 17,385 | ||||||
| Supplemental disclosures of noncash investing and financing activities: |
||||||||||||
| Fixed assets acquired through capital leases |
$ | 591 | $ | 28 | $ | 207 | ||||||
| Net change in foreign currency translation adjustment and unrealized gain (loss) on derivative financial instruments, net of tax |
$ | (525 | ) | $ | 580 | $ | (309 | ) | ||||
| Fair value of assets acquired in acquisitions, net of cash received |
$ | 84,141 | $ | — | $ | — | ||||||
| Goodwill |
105,395 | — | — | |||||||||
| Intangible assets |
115,650 | — | — | |||||||||
| Liabilities assumed |
(57,807 | ) | — | — | ||||||||
| Holdback provision |
(13,904 | ) | — | — | ||||||||
| Accrued earn-out |
(45,831 | ) | — | — | ||||||||
| Deferred tax liability |
(44,188 | ) | — | — | ||||||||
| Treasury stock issued |
(31,948 | ) | — | — | ||||||||
| Net cash paid for acquisitions |
$ | 111,508 | $ | — | $ | — | ||||||
See accompanying notes to consolidated financial statements.
41
Table of Contents
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2005, 2004 and 2003
(1) Summary of Significant Accounting Policies
(a) General
AMN Healthcare Services, Inc. was incorporated in Delaware on November 10, 1997. AMN Healthcare Services, Inc. and its subsidiaries recruit and place physicians, nurses and allied health professionals nationally and internationally on a temporary or permanent basis at acute-care hospitals and other healthcare facilities throughout the United States. AMN Healthcare Services, Inc. and its subsidiaries collectively are herein referred to as “the Company”.
On November 2, 2005, the Company completed its acquisition of The MHA Group, Inc. and subsidiaries, a Texas corporation (“MHA”). MHA, through its wholly-owned subsidiaries, provides temporary physician, nurse and allied healthcare staffing services as well as physician and allied healthcare permanent placement services.
(b) Principles of Consolidation
The accompanying consolidated financial statements include the accounts of AMN Healthcare Services, Inc. and its subsidiaries. All significant intercompany balances and transactions have been eliminated in consolidation.
(c) Cash and Cash Equivalents
The Company considers all highly liquid investments with an original maturity of three months or less to be cash equivalents. Cash and cash equivalents include currency on hand, deposits with financial institutions and highly liquid investments. At December 31, 2005 and 2004, the Company held $310,000 and $303,000, respectively, in a collateral trust account restricted for use related to a professional liability insurance agreement. Cash and cash equivalents were $19,110,000 and $3,908,000 at December 31, 2005 and 2004, respectively.
(d) Fixed Assets
Furniture, equipment, leasehold improvements and software are recorded at cost less accumulated amortization and depreciation. Equipment acquired under capital leases is recorded at the present value of the future minimum lease payments. Major additions and improvements are capitalized and maintenance and repairs are expensed when incurred. Depreciation on furniture, equipment and software is calculated using the straight-line method based on the estimated useful lives of the related assets (generally three to five years). Leasehold improvements and equipment obtained under capital leases are amortized over the shorter of the term of the lease or their estimated useful life. Amortization of equipment obtained under capital leases is included with depreciation expense in the accompanying consolidated financial statements.
Costs incurred to develop internal-use software during the application development stage are capitalized and recorded at cost, subject to an impairment test as described below. Application development stage costs generally include costs associated with internal-use software configuration, coding, installation and testing. Costs of significant upgrades and enhancements that result in additional functionality also are capitalized, whereas costs incurred for maintenance and minor upgrades and enhancements are expensed as incurred. Capitalized costs are amortized using the straight-line method over three or five years once placed into service. The Company assesses potential impairment of capitalized internal-use software quarterly or whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. Recoverability of assets to be held and used is measured by a comparison of the carrying amount of an asset to the future undiscounted net cash
42
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
flows that are expected to be generated by the asset. If such assets are considered to be impaired, the impairment to be recognized is measured by the amount by which the carrying amount of the assets exceeds the fair value of the assets. Assets to be disposed of are reported at the lower of the carrying amount or fair value less costs to sell.
(e) Goodwill
The excess of purchase price and related costs over the fair value of net assets of entities acquired is recorded as goodwill. In accordance with SFAS No. 142, Goodwill and Other Intangible Assets, the Company evaluates goodwill annually for impairment at the reporting unit level and whenever circumstances occur indicating that goodwill might be impaired. The performance of the test involves a two-step process. The first step of the impairment test involves comparing the fair value of the Company’s reporting units with the reporting unit’s carrying amount, including goodwill. The Company generally determines the fair value of its reporting units using the expected present value of future cash flows, giving consideration to the market valuation approach. If the carrying amount of the Company’s reporting units exceeds the reporting unit’s fair value, the Company performs the second step of the goodwill impairment test to determine the amount of impairment loss. The second step of the goodwill impairment test involves comparing the implied fair value of the Company’s reporting unit’s goodwill with the carrying amount of that goodwill. At December 31, 2005 and 2004, the Company performed the annual impairment test and determined there was no impairment of goodwill.
(f) Intangible Assets
Intangible assets consist of identifiable intangible assets acquired through the Company’s acquisition of The MHA Group, Inc. (“MHA”) in November 2005, debt issuance costs related to the Company’s credit facility and other noncompete covenants from previous acquisitions. Identifiable intangible assets acquired through the acquisition of MHA include tradenames and trademarks, customer relationships, noncompete agreements and staffing databases. Amortizable intangible assets, which do not include those tradenames and trademarks with an indefinite life, are amortized using the straight-line method over their useful lives. Debt issuance costs are deferred and amortized to interest expense using the effective interest method over the respective term of the credit facility. Noncompete covenants, including those acquired through the acquisition of MHA, as well as other acquisitions, are amortized using the straight-line method over the life of the related agreements.
(g) Insurance Reserves
The Company maintains an accrual for incurred, but not reported, claims arising from self-insured health benefits provided to the Company’s temporary healthcare professionals, which is included in accrued compensation and benefits in the consolidated balance sheets. The Company determines the adequacy of this accrual by evaluating its historical experience and trends related to both health insurance claims and payments, information provided by their insurance broker and third party administrator, as well as industry experience and trends. If such information indicates that the accruals are overstated or understated, the Company reduces or provides for additional accruals. The Company’s accrual at December 31, 2005 was based on (i) a monthly average of the Company’s actual historical health insurance claim amounts and (ii) the average period of time from the date the claim is incurred to the date that it is reported to the Company and paid. The Company believes this is the best estimate of the amount of incurred, but not reported, self-insured health benefit claims at year-end. As of December 31, 2005 and December 31, 2004, the Company had $2.4 million and $2.3 million, respectively, accrued for incurred, but not reported, health insurance claims.
The Company maintains an accrual for professional liability self-insured retention limits, net of insurance recoverable, which is included in accounts payable and accrued expenses in the consolidated balance sheets. The
43
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
Company determines the adequacy of this accrual by evaluating its historical experience and trends, loss reserves established by the Company’s insurance carriers, management and third-party administrators, as well as through the use of independent actuarial studies. The Company obtains updated actuarial studies on a regular basis that use actual claims data to determine the appropriate reserves for incurred, but not reported, professional liability claims for each year. As of December 31, 2005 and December 31, 2004, the Company had $13.9 million and $7.0 million, respectively, accrued for professional liability retention of which the current portion is $1.9 million and $2.2 million, respectively. The increase in the reserve is primarily due to the acquisition of MHA which is also self-insured for professional liability.
The Company maintains an accrual for workers compensation self-insured retention limits, which is included in accrued compensation and benefits in the consolidated balance sheets. The Company determines the adequacy of this accrual by evaluating its historical experience and trends, loss reserves established by the Company’s insurance carriers and third party administrators, as well as through the use of independent actuarial studies. The Company obtains updated actuarial studies on a semi-annual basis that use actual claims data to determine the appropriate reserve both for reported claims and incurred, but not reported, claims for each policy year. The actuarial study for workers compensation provides the Company with the estimated losses for prior policy years and an estimated percentage of payroll compensation to be accrued for current years. The Company records its accruals based on the amounts provided in the actuarial study and believes this is the best estimate of the Company’s liability for reported claims and incurred, but not reported, claims as of December 31, 2005 and December 31, 2004. As of December 31, 2005 and December 31, 2004, the Company had $10.1 million and $8.1 million, respectively, accrued for workers compensation claims of which the current portion is $3.0 million and $2.7 million, respectively.
(h) Accounts Receivable and Allowance for Doubtful Accounts
The Company maintains an allowance for doubtful accounts for estimated credit losses resulting from collection risks, including the inability of customers to make required payments. This results in a provision for bad debt expense. The allowance for doubtful accounts is reported as a reduction of accounts receivable in the consolidated balance sheets. The adequacy of this allowance is determined by evaluating the credit risk for individual customer receivables, considering the financial condition of each customer and historical payment trends, delinquency trends, credit histories of customers and current economic conditions. If the financial condition of a customer were to deteriorate, resulting in an impairment of their ability to make payments, additional allowances would be provided.
(i) Concentration of Credit Risk
The majority of the Company’s business activity is with hospitals located throughout the United States. Credit is extended based on the evaluation of each entity’s financial condition, and collateral is generally not required. Credit losses have been within management’s expectations. No single client healthcare system exceeded 10% of revenue for the years ended December 31, 2005, 2004 and 2003.
The Company’s cash and cash equivalents are also financial instruments that are exposed to concentration of credit risk. The Company places its cash balances with high-credit quality and federally insured institutions. Cash balances with any one institution may be in excess of federally insured limits or may be invested in a non-federally insured money market account.
44
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
(j) Revenue Recognition
Revenue consists of fees earned from the permanent and temporary placement of healthcare professionals. Revenue is recognized when earned and realizable and therefore when the following criteria have been met: (a) persuasive evidence of an arrangement exists; (b) services have been rendered; (c) the fee is fixed or determinable; and (d) collectibility is reasonably assured. For temporary placements, revenue is recognized in the period in which services are provided based on hours worked by the temporary healthcare professionals. For permanent placements, revenue is recognized over the estimated maximum period of performance on a straight-line basis. Any fees that are billable on a contingent basis are recognized once the contingency is resolved over the remaining estimated maximum period of performance. Billings in excess of revenue are recorded as deferred revenue in the accompanying consolidated balance sheets.
(k) Advertising Expenses
Advertising costs are expensed as incurred. Advertising expenses were $8,166,000, $8,132,000 and $8,463,000 for the years ended December 31, 2005, 2004 and 2003, respectively.
(l) Income Taxes
The Company records income taxes using the asset and liability method. Deferred tax assets and liabilities are recognized for the future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax basis. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in operations in the period the changes are enacted. If it is more likely than not that some portion or all of a deferred tax asset will not be realized, a valuation allowance is recognized.
(m) Impairment of Long-Lived Assets
Long-lived assets and certain identifiable intangibles are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. Recoverability of assets to be held and used is measured by a comparison of the carrying amount of an asset to the future undiscounted cash flows that are expected to be generated by the asset. If such assets are considered to be impaired, the impairment to be recognized is measured by the amount by which the carrying amount of the assets exceeds the fair value of the assets. Assets to be disposed of are reported at the lower of the carrying amount or fair value less costs to sell.
(n) Fair Value of Financial Instruments
The carrying amounts of cash and cash equivalents, accounts receivable, income tax receivable, bank overdraft, accounts payable and accrued expenses, accrued compensation and benefits, income taxes payable and other current liabilities approximate their respective fair values due to the short-term nature and liquidity of these financial instruments. The carrying amounts of notes payable approximate their fair value, as the instruments’ interest rates are comparable to rates currently offered for similar debt instruments of comparable maturities. Derivative financial instruments are recorded at fair value based on dealer quotes. The long-term portion of the acquisition price holdback liability is recorded at its fair value, using the discounted cash flow method. The fair value of the long-term portion of the Company’s self insurance accruals cannot be estimated as the Company cannot reasonably determine the timing of future payments.
45
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
(o) Stock-Based Compensation
The Company applies the intrinsic value-based method of accounting prescribed by Accounting Principles Board (APB) Opinion No. 25, Accounting for Stock Issued to Employees, and related interpretations including FASB Interpretation No. 44, Accounting for Certain Transactions Involving Stock Compensation, an Interpretation of APB Opinion No. 25, and EITF 00-23, Issues Related to the Accounting for Stock Compensation under APB Opinion No. 25 and FASB Interpretation No. 44, to account for its stock option plans. Under this method, compensation expense for fixed plans is recognized only if, on the date of grant, the then current market price of the underlying stock exceeds the exercise price, and is recorded on a straight-line basis over the applicable vesting period. Compensation expense for variable plans is measured at the end of each reporting period until the related performance criteria are met and is measured based on the excess of the then current market price of the underlying stock over the exercise price. Compensation expense previously recorded for unvested employee stock-based compensation awards that are forfeited upon employee termination is reversed in the period of forfeiture. SFAS No. 123, Accounting for Stock-Based Compensation, established accounting and disclosure requirements using a fair value-based method of accounting for stock-based employee compensation plans. As allowed by SFAS No. 123, the Company has elected to continue to apply the intrinsic value-based method of accounting described above, and has adopted the disclosure requirements of SFAS No. 123, as amended by SFAS No. 148, Accounting for Stock-Based Compensation-Transition and Disclosure.
The following table compares net income and net income per share as reported by the Company to the pro forma amounts that would be reported had compensation expense been recognized for the Company’s stock-based compensation plans in accordance with SFAS No. 123 (in thousands, except per share amounts):
| Years Ended December 31, | |||||||||
| 2005 |
2004 |
2003 | |||||||
| As reported: |
|||||||||
| Net income |
$ | 22,234 | $ | 17,346 | $ | 37,792 | |||
| Stock-based employee compensation, net of tax |
$ | 85 | $ | 466 | $ | 1,227 | |||
| Net income per common share: |
|||||||||
| Basic |
$ | 0.76 | $ | 0.61 | $ | 1.04 | |||
| Diluted |
$ | 0.69 | $ | 0.55 | $ | 0.95 | |||
| Pro forma: |
|||||||||
| Net income, as reported |
$ | 22,234 | $ | 17,346 | $ | 37,792 | |||
| Incremental stock-based employee compensation per SFAS 123, net of tax |
3,575 | 2,003 | 2,062 | ||||||
| Pro forma net income |
$ | 18,659 | $ | 15,343 | $ | 35,730 | |||
| Pro forma net income per common share: |
|||||||||
| Basic |
$ | 0.64 | $ | 0.54 | $ | 0.98 | |||
| Diluted |
$ | 0.58 | $ | 0.49 | $ | 0.90 | |||
46
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
The weighted average per share fair value of options granted during 2005, 2004 and 2003 was $6.99, $7.39 and $5.21, respectively, on the date of grant. Fair value was determined using the Black-Scholes option-pricing model with the following weighted-average assumptions:
| 2005 |
2004 |
2003 | ||||
| Expected life |
5 years | 5 years | 5 years | |||
| Risk-free interest rate |
3.98% | 3.50% | 2.62% | |||
| Volatility |
48% | 54% | 61% | |||
| Dividend yield |
0% | 0% | 0% |
(p) Net Income per Common Share
Basic net income per common share is calculated by dividing net income by the weighted average number of common shares outstanding during the reporting period.
Options to purchase 567,000, 651,000 and 655,000 shares of common stock in 2005, 2004 and 2003, respectively, were not included in the calculations of diluted net income per common share because the effect of these instruments was anti-dilutive.
The following table sets forth the computation of basic and diluted net income per common share for the years ended December 31, 2005, 2004 and 2003, respectively (in thousands, except per share amounts):
| Years Ended December 31, | |||||||||
| 2005 |
2004 |
2003 | |||||||
| Net income |
$ | 22,234 | $ | 17,346 | $ | 37,792 | |||
| Weighted average common shares outstanding—basic |
29,130 | 28,248 | 36,456 | ||||||
| Net income per common share—basic |
$ | 0.76 | $ | 0.61 | $ | 1.04 | |||
| Weighted average common shares outstanding—basic |
29,130 | 28,248 | 36,456 | ||||||
| Plus dilutive stock options |
2,988 | 3,121 | 3,329 | ||||||
| Weighted average common shares outstanding—diluted |
32,118 | 31,369 | 39,785 | ||||||
| Net income per common share—diluted |
$ | 0.69 | $ | 0.55 | $ | 0.95 | |||
(q) Comprehensive Income
SFAS No. 130, Reporting Comprehensive Income, establishes standards for the reporting of comprehensive income and its components. Comprehensive income (loss) includes items such as hedge effective gains and losses on derivative contracts and foreign currency translation adjustments. For the years ended December 31, 2005, 2004 and 2003, comprehensive income was $21,709,000, $17,926,000 and $37,483,000 and included an unrealized gain (loss) on interest rate swap arrangements, net of tax, of $(443,000), $588,000 and $(198,000), respectively, and a foreign currency translation adjustment loss of $82,000, $8,000 and $111,000, respectively.
(r) Derivative Instruments
SFAS No. 133, Accounting for Derivative Instruments and Hedging Activities, requires that all derivative instruments be recorded on the balance sheet at fair value. Gains or losses resulting from changes in the values of
47
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
those derivatives are accounted for depending upon the use of the derivative and whether it qualifies for hedge accounting. The Company uses derivative instruments to manage the fluctuations in cash flows resulting from interest rate risk on variable-rate debt financing.
In October 2003, in connection with the amendment to the Credit Agreement, the Company entered into interest rate swap arrangements to minimize exposure to interest rate fluctuations on $30 million of the outstanding variable rate debt under the existing credit facility, where the Company pays a fixed rate of 2.65% and receives a floating three-month LIBOR. This agreement expires in September 2006, and no initial investment was made to enter into this agreement. In June 2005, the Company entered into two additional interest rate swaps. The first agreement has a notional amount of $20 million and became effective in September 2005, whereby the Company pays a fixed rate of 3.99% and receives a floating three-month LIBOR. The agreement expires in March 2007. The second agreement will become effective in September 2006, with a notional amount of $15 million whereby the Company pays a fixed rate of 4.09% and receives a floating three-month LIBOR. This agreement will expire in September 2007. In November 2005 the Company entered into five additional interest rate swap agreements for notional amounts of $15 million, $10 million, $30 million, $35 million and $50 million, whereby the Company pays fixed rates of 4.82%, 4.95%, 4.87%, 4.94%, and 4.97%, respectively, and receives a floating three-month LIBOR. These agreements expire in December 2007, June 2008, December 2008, December 2009 and December 2010, respectively.
At December 31, 2005 and 2004, the interest rate swap agreements had a fair value of ($0.1) million and $0.7 million, respectively, which is included in other assets and liabilities in the accompanying consolidated balance sheets. The Company has formally documented the hedging relationships and accounts for these arrangements as cash flow hedges. The Company recognizes all derivatives on the balance sheet at fair value based on dealer quotes. Gains or losses resulting from changes in the values of these arrangements are recorded in other comprehensive income, net of tax, until the hedged item is recognized in earnings. The Company also formally assesses, both at the hedge’s inception and on an ongoing basis, whether the derivatives that are used in the hedging transactions are highly effective in offsetting changes in fair values or cash flows of the hedged items. When it is determined that a derivative is not highly effective as a hedge or that it has ceased to be a highly effective hedge, the Company discontinues hedge accounting prospectively and recognizes subsequent changes in market value in earnings.
(s) New Accounting Pronouncements
In December 2004, the FASB issued Statement No. 123 (Revised), Share-Based Payment, (“FAS 123R”), which amends Statement No. 123, Accounting for Stock-Based Compensation, and supersedes Accounting Principles Board (“APB”) Opinion No. 25, Accounting for Stock Issued to Employees. FAS 123R requires the measurement of compensation cost related to all share-based payments to employees, including grants of employee stock options, using a fair-value-based method and the recording of such cost in the Company’s consolidated statements of operations. Additionally, FAS 123R requires that estimated forfeitures be considered in determining compensation cost. The accounting provisions of FAS 123R are effective for the first interim or annual reporting period that begins after June 15, 2005. FAS 123R, which provides certain changes to the method for valuing share-based compensation, among other changes, will apply to new awards and to awards that are outstanding on the effective date that are subsequently modified or cancelled. Compensation expense for outstanding awards for which the requisite service had not been rendered as of the effective date will be recognized over the remaining service period using compensation cost similar to that calculated for pro forma disclosure purposes under FAS 123. Of the $11.9 million of unamortized compensation expense at December 31, 2005, before the effect of income taxes related to outstanding unvested options, as determined in accordance with FAS 123, $5.1 million is expected to be recorded during fiscal 2006. The Company will likely incur additional expense during 2006 related to new awards granted during 2006 that cannot yet be quantified. The Company
48
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
adopted FAS 123R on January 1, 2006 using the modified prospective method, and the Company will value share-based awards granted after the effective date using the Black-Scholes option pricing model, which is consistent with the valuation method previously used for footnote disclosure purposes in accordance with FAS 123.
(t) Segment Information
SFAS No. 131, Disclosures about Segments of an Enterprise and Related Information, establishes annual and interim reporting standards for an enterprise’s operating segments and related disclosures about its products, services, geographic areas and major customers. An operating segment is defined as a component of an enterprise that engages in business activities from which it may earn revenue and incur expenses, and for which discrete financial information is regularly evaluated by the chief operating decision maker in deciding how to allocate resources and assess performance.
The Company provides hospital and healthcare facilities with temporary staffing for physicians, nurses and allied healthcare professionals and permanent physician placement services through the use of several brand names, each having their own marketing and supply distinction. The Company’s operating segments are identified in the same manner as they are reported internally and used by the Company’s chief operating decision maker for the purposes of evaluating performance and allocating resources. For all periods presented, except for fiscal year 2005, the Company believes it operated in a single segment, healthcare staffing for hospitals and healthcare facilities. With the acquisition of MHA in November 2005, the Company has two reportable operating segments: nurse and allied healthcare staffing segment and physician staffing segment.
The Company’s management relies on internal management reporting processes that provide revenue and segment operating income for making financial decisions and allocating resources. Segment operating income includes income from operations before depreciation, amortization of intangible assets and amortization of stock compensation expense. Management believes that segment operating income is an appropriate measure of evaluating the operational performance of the Company’s segments. However, this measure should be considered in addition to, not as a substitute for, or superior to, income from operations or other measures of financial performance prepared in accordance with generally accepted accounting principles. The Company’s management does not evaluate, manage or measure performance of segments using asset information; accordingly, asset information by segment is not prepared or disclosed. The information in the following table is derived from the segment’s internal financial information as used for corporate management purposes.
49
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
The following table provides a reconciliation of revenue and segment operating income by reportable segment to consolidated results (in thousands):
| Years Ended December 31, | |||||||||
| 2005 |
2004 |
2003 | |||||||
| Revenue |
|||||||||
| Nurse and allied healthcare staffing |
$ | 658,843 | $ | 629,016 | $ | 714,209 | |||
| Physician staffing |
47,000 | — | — | ||||||
| $ | 705,843 | $ | 629,016 | $ | 714,209 | ||||
| Segment Operating Income |
|||||||||
| Nurse and allied healthcare staffing |
$ | 48,256 | $ | 42,926 | $ | 69,657 | |||
| Physician staffing |
4,795 | — | — | ||||||
| 53,051 | 42,926 | 69,657 | |||||||
| Depreciation and amortization |
6,179 | 5,837 | 4,819 | ||||||
| Non-cash stock-based compensation |
142 | 750 | 874 | ||||||
| Interest expense, net |
9,565 | 8,440 | 2,303 | ||||||
| Income before income taxes |
$ | 37,165 | $ | 27,899 | $ | 61,661 | |||
(u) Use of Estimates
The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make a number of estimates and assumptions relating to the reporting of assets and liabilities and the disclosure of contingent assets and liabilities at the dates of the financial statements and the reported amounts of revenue and expenses during the reporting periods. Actual results could differ from those estimates.
(v) Reclassifications
Certain amounts in the 2004 and 2003 consolidated financial statements have been reclassified to conform to the 2005 presentation.
(2) Acquisitions
MHA Acquisition
On November 2, 2005, the Company completed its acquisition of MHA. The acquisition established AMN as the largest provider of healthcare staffing services in the United States. The strategic combination has broadened the type of services the Company offers and will allow the Company to provide a more comprehensive staffing solution to clients. Because the Company possesses one of the largest national networks of available physician, nurse and allied health professionals, the Company is well positioned to offer our hospital and healthcare facility clients a spectrum of effective solutions to meet their staffing needs.
The acquisition was recorded using the purchase method of accounting. Thus, the results of operations from MHA are included in the Company’s consolidated financial statements from the acquisition date. The total purchase price of $210.0 million consisted of (i) an initial price of $160.0 million, paid approximately 75% in cash, excluding a $15.0 million holdback for potential claims indemnified by the MHA shareholders, and approximately 25% in unregistered shares of the Company’s common stock, (ii) contingent purchase price of
50
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
$47.3 million, paid approximately 75% in cash and 25% in unregistered share of the Company’s common stock, and (iii) $2.7 million of direct acquisition costs. The purchase price included contingent consideration based on the financial performance of MHA for the twelve months ended December 31, 2005. The earn-out of $47.3 million was finalized on December 31, 2005 and recorded as additional purchase price at its fair value. The holdback, net of any indemnified claims made by the selling shareholders, will be released to the selling shareholders in March 2007. In addition to cash consideration paid, the Company issued 2.3 million unregistered shares of common stock in connection with the acquisition of MHA, and issued an additional 0.7 million unregistered shares on March 9, 2006 for payment of earn-out amounts as provided in the acquisition agreement. The cash and stock components of the earn-out and holdback, as well as the stock portion of the initial purchase price, have been recorded at their fair values, including discounts for restrictions on the marketability of the stock and the timing of expected future cash payments. The allocation of the purchase price to the assets acquired and liabilities assumed based on their estimated fair values was as follows (in thousands):
| Purchase Price: |
||||
| Cash paid for MHA common stock |
$ | 108,140 | ||
| Cash holdback |
13,904 | |||
| Equity issued for MHA common stock |
31,948 | |||
| Earn-out—cash |
35,164 | |||
| Earn-out—equity |
10,667 | |||
| Transaction costs |
2,712 | |||
| Total purchase price of acquisition |
$ | 202,535 | ||
| Assets Acquired: |
||||
| Net assets acquired |
$ | 27,240 | ||
| Identifiable intangible assets |
115,600 | |||
| Deferred tax liability and other liabilities |
(45,188 | ) | ||
| Goodwill |
104,883 | |||
| Total assets acquired |
$ | 202,535 | ||
Intangible assets include amounts recognized for the fair value of tradenames and trademarks, customer relationships, non-compete agreements, and staffing databases. The following table summarizes the fair value and useful life of each intangible asset acquired:
| Fair Value |
Useful Life | ||||
| (in thousands) | (in years) | ||||
| Identifiable intangible assets subject to amortization: |
|||||
| Staffing databases |
$ | 1,600 | 5 | ||
| Customer relationships |
32,000 | 14 | |||
| Tradenames and trademarks |
1,200 | 5 | |||
| Noncompete agreements |
900 | 5 | |||
| 35,700 | |||||
| Identifiable intangible assets not subject to amortization: |
|||||
| Tradenames and trademarks |
79,900 | indefinite | |||
| Total identifiable intangible assets acquired |
$ | 115,600 | |||
Of the total $104.9 million of the purchase price allocated to goodwill, $96.2 million and $8.7 million was allocated to the Company’s physician staffing segment and nurse and allied healthcare staffing segment, respectively. Goodwill represents the excess of the purchase price over the fair value of the net tangible and
51
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
intangible assets acquired, and is not deductible for tax purposes. Goodwill will not be amortized and will be tested for impairment at least annually. The Company’s total goodwill at December 31, 2005 was $240.8 million, including the MHA earn-out liability.
The following summary presents pro forma consolidated results of operations for the years ended December 31, 2005 and 2004 as if the MHA acquisition described above had occurred on January 1, 2005 and 2004. The following unaudited pro forma financial information gives effect to certain adjustments, including the reduction in compensation expense related to non-recurring executive salary expense and non-recurring professional service fees, the amortization of intangible assets and interest expense on acquisition related debt and accretion of fair valued liabilities. The pro forma financial information is not necessarily indicative of the operating results that would have occurred had the acquisition been consummated as of the date indicated, nor are they necessarily indicative of future operating results.
| (Unaudited) | ||||||
| Year ended December 31, | ||||||
| 2005 |
2004 | |||||
| (in thousands, except per share amounts) | ||||||
| Revenue |
$ | 959,821 | $ | 862,311 | ||
| Income from operations |
$ | 64,018 | $ | 46,266 | ||
| Net income |
$ | 28,880 | $ | 18,024 | ||
| Net income per common share: |
||||||
| Basic |
$ | 0.91 | $ | 0.58 | ||
| Diluted |
$ | 0.83 | $ | 0.52 | ||
| Weighted average common shares: |
||||||
| Basic |
31,733 | 31,226 | ||||
| Diluted |
34,789 | 34,416 | ||||
OGP Europe Acquisition
On April 19, 2005, the Company completed the acquisition of O’Grady-Peyton International (Europe) Limited (OGP Europe) for a total purchase price of $0.5 million, including $0.1 million net liabilities assumed, which resulted in the recording of $0.5 million of goodwill and $0.1 million of identified intangible assets. The acquisition was recorded using the purchase method of accounting. Thus, the results of operations of OGP Europe are included in the Company’s consolidated financial statements from the acquisition date.
(3) Tender Offer
On October 16, 2003, the Company completed a tender offer for $180,000,000, or 9,722,222 shares of its outstanding common stock and 376,029 employee stock options at a price of $18.00 per share. In connection with the tender offer, the Company amended its then current credit facility. The tender offer was financed with a $130,000,000 term loan under the Company’s amended credit facility, $15,000,000 of borrowings under the Company’s revolving credit facility and $35,000,000 of cash on hand. The Company also paid $110,000 and $4,433,000 in transaction costs in 2004 and 2003, respectively, associated with the tender offer and the amendment of the credit facility, which were funded with cash on hand. See Notes 7 and 9(a).
52
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
(4) Goodwill and Identifiable Intangible Assets
As of December 31, 2005 and 2004, the Company had the following acquired intangible assets (in thousands):
| December 31, 2005 |
December 31, 2004 |
|||||||||||||
| Gross Carrying Amount |
Accumulated Amortization |
Gross Carrying Amount |
Accumulated Amortization |
|||||||||||
| Intangible assets subject to amortization: |
||||||||||||||
| Staffing databases |
$ | 1,600 | $ | (52 | ) | $ | — | $ | — | |||||
| Customer relationships |
32,000 | (368 | ) | — | — | |||||||||
| Tradenames and trademarks |
1,200 | (39 | ) | — | — | |||||||||
| Noncompete agreements |
1,150 | (222 | ) | $ | 400 | $ | (318 | ) | ||||||
| Deferred financing costs |
7,576 | (1,593 | ) | 5,619 | (2,201 | ) | ||||||||
| $ | 43,526 | $ | (2,274 | ) | $ | 6,019 | $ | (2,519 | ) | |||||
| Intangible assets not subject to amortization: |
||||||||||||||
| Goodwill (1) |
$ | 251,296 | $ | (10,452 | ) | $ | 145,901 | $ | (10,452 | ) | ||||
| Tradenames and trademarks |
79,900 | — | — | — | ||||||||||
| $ | 331,196 | $ | (10,452 | ) | $ | 145,901 | $ | (10,452 | ) | |||||
(1) Goodwill accumulated amortization represents amortization expense recorded prior to the Company’s adoption of SFAS No. 142, Goodwill and Other Intangible Assets, on January 1, 2002.
During 2004, the Company wrote off $1,144,000 of fully amortized intangible assets related to the expired noncompete agreements, and incurred credit facility amendment fees of $258,000 which were capitalized as deferred financing costs.
Aggregate amortization expense for intangible assets was $2,902,000 and $1,697,000 for the years ended December 31, 2005 and 2004, respectively. Amortization of deferred financing costs is included in interest expense. Based on the current amount of intangibles subject to amortization, the estimated amortization expense as of December 31, 2005 is as follows (in thousands):
| Amount | |||
| Year ending December 31, 2006 |
$ | 4,168 | |
| Year ending December 31, 2007 |
4,153 | ||
| Year ending December 31, 2008 |
4,153 | ||
| Year ending December 31, 2009 |
4,144 | ||
| Year ending December 31, 2010 |
3,936 | ||
| Thereafter |
20,698 | ||
| $ | 41,252 | ||
As of December 31, 2005 and 2004, the Company had unamortized goodwill of $240,844,000 and $135,449,000, respectively. Of the $105,395,000 increase in goodwill, $104,883,000 was related to the acquisition of MHA in November 2005, and $512,000 was related to the acquisition of O’Grady-Peyton International (Europe) Limited in April 2005.
53
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
(5) Balance Sheet Details
The consolidated balance sheets detail is as follows as of December 31, 2005 and 2004 (in thousands):
| December 31, |
||||||||
| 2005 |
2004 |
|||||||
| Fixed assets: |
||||||||
| Furniture and equipment |
$ | 13,580 | $ | 10,688 | ||||
| Software |
20,469 | 17,370 | ||||||
| Leasehold improvements |
4,942 | 4,527 | ||||||
| 38,991 | 32,585 | |||||||
| Accumulated depreciation and amortization |
(18,827 | ) | (14,752 | ) | ||||
| Fixed assets, net |
$ | 20,164 | $ | 17,833 | ||||
| Accrued compensation and benefits: |
||||||||
| Accrued payroll |
$ | 13,196 | $ | 11,833 | ||||
| Accrued bonuses |
8,376 | 3,397 | ||||||
| Accrued health insurance reserve |
2,373 | 2,274 | ||||||
| Accrued workers compensation reserve |
3,240 | 2,683 | ||||||
| Other |
5,023 | 4,408 | ||||||
| Accrued compensation and benefits |
$ | 32,208 | $ | 24,595 | ||||
| Other current liabilities: |
||||||||
| Acquisition earn-out liability |
$ | 46,096 | $ | — | ||||
| Acquisition purchase price holdback liability |
2,290 | — | ||||||
| Facility deposits |
6,789 | — | ||||||
| Other |
3,843 | 351 | ||||||
| Other current liabilities |
$ | 59,018 | $ | 351 | ||||
| Other long-term liabilities: |
||||||||
| Acquisition purchase price holdback liability |
$ | 11,356 | $ | — | ||||
| Workers compensation reserve |
7,104 | 5,375 | ||||||
| Professional liability reserve |
12,008 | 4,775 | ||||||
| Other |
6,659 | 3,173 | ||||||
| Other long-term liabilities |
$ | 37,127 | $ | 13,323 | ||||
54
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
(6) Income Taxes
The provision for income taxes for the years ended December 31, 2005, 2004 and 2003 consists of the following (in thousands):
| December 31, | |||||||||||
| 2005 |
2004 |
2003 | |||||||||
| Current income taxes: |
|||||||||||
| Federal |
$ | (6,535 | ) | $ | 5,543 | $ | 14,816 | ||||
| State |
2,080 | 871 | 3,013 | ||||||||
| Foreign |
576 | 53 | — | ||||||||
| Total |
(3,879 | ) | 6,467 | 17,829 | |||||||
| Deferred income taxes: |
|||||||||||
| Federal |
18,245 | 4,171 | 5,591 | ||||||||
| State |
604 | (55 | ) | 449 | |||||||
| Foreign |
(39 | ) | (30 | ) | — | ||||||
| Total |
18,810 | 4,086 | 6,040 | ||||||||
| Provision for income taxes |
$ | 14,931 | $ | 10,553 | $ | 23,869 | |||||
The Company’s income tax expense differs from the amount that would have resulted from applying the federal statutory rate of 35% to pretax income because of the effect of the following items during the years ended December 31, 2005, 2004 and 2003 (in thousands):
| December 31, | ||||||||||
| 2005 |
2004 |
2003 | ||||||||
| Tax expense at federal statutory rate |
$ | 13,008 | $ | 9,765 | $ | 21,582 | ||||
| State taxes, net of federal benefit |
1,659 | 974 | 2,132 | |||||||
| Other, net |
264 | (186 | ) | 155 | ||||||
| Income tax expense |
$ | 14,931 | $ | 10,553 | $ | 23,869 | ||||
55
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
The tax effects of temporary differences that give rise to significant portions of deferred tax assets and deferred tax liabilities are presented below as of December 31, 2005 and 2004 (in thousands):
| December 31, |
||||||||
| 2005 |
2004 |
|||||||
| Deferred tax assets: |
||||||||
| Stock compensation |
$ | 15,535 | $ | 17,480 | ||||
| Deferred revenue |
4,559 | — | ||||||
| Allowance for doubtful accounts |
954 | 205 | ||||||
| Deferred compensation |
606 | 414 | ||||||
| Accrued expenses, net |
6,288 | 4,772 | ||||||
| Deferred rent |
1,123 | — | ||||||
| Net operating losses |
7,276 | — | ||||||
| State taxes |
358 | — | ||||||
| Other |
464 | 10 | ||||||
| Total deferred tax assets |
$ | 37,163 | $ | 22,881 | ||||
| Deferred tax liabilities: |
||||||||
| Intangibles |
$ | (63,587 | ) | $ | (13,284 | ) | ||
| Fixed assets, net |
(4,481 | ) | (4,112 | ) | ||||
| Prepaid expenses |
(2,820 | ) | (3,715 | ) | ||||
| State taxes |
— | (52 | ) | |||||
| Total deferred tax liabilities |
$ | (70,888 | ) | $ | (21,163 | ) | ||
| Valuation allowance |
$ | (102 | ) | — | ||||
| Net deferred tax assets |
$ | (33,827 | ) | $ | 1,718 | |||
56
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
Management believes it is more likely than not that the results of future operations will generate sufficient taxable income to realize the deferred tax assets, excluding state net operating loss carryforwards and foreign tax credit carryforwards, and, accordingly, has not provided a valuation allowance for these assets except for the items mentioned below.
As of December 31, 2005, the Company has federal and state net operating loss carryforwards of $14,248,000 and $41,428,000, respectively, that are set to expire at various dates between 2009 and 2025. Management believes it is not more likely than not that the Company will generate sufficient taxable income to utilize $562,000 of these state losses prior to the expiration of these state net operating loss carryforwards, and therefore the Company has established a valuation allowance of $28,000 for these state net operating loss carryforwards.
As of December 31, 2005, the Company has foreign tax credit carryforwards of $74,000 that are set to expire in 2014. Management believes it is not more likely than not that the Company will generate sufficient foreign source income to utilize these foreign tax credit carryforwards, and therefore the Company has established a valuation allowance of $74,000 for these foreign tax credit carryforwards.
As of December 31, 2005, the Company has California research and development credit carryforwards of $16,000 that generally do not expire. Management believes it is more likely than not that the Company will generate sufficient taxable income to utilize these California research and development credit carryforwards, and therefore the Company has not provided a valuation allowance for these assets.
As of December 31, 2005, pursuant to APB No. 23, “Accounting for Income Taxes – Special Areas”, the Company did not provide for United States income taxes or foreign withholding taxes on undistributed earnings from certain non-U.S. subsidiaries that will be permanently reinvested outside the United States. The Company intends to reinvest its foreign earnings indefinitely under APB-23. Should the Company repatriate foreign earnings, the Company would have to adjust the income tax provision in the period management determined that the Company would repatriate earnings.
(7) Notes Payable and Related Derivative Instruments and Credit Agreement
In January 2003, the Company amended its Amended and Restated Credit Agreement (“Credit Agreement”) by increasing the funds available for borrowing under the revolving credit facility from $50 million to $75 million and extending the maturity date from November 16, 2004 to December 31, 2006. The Credit Agreement also included up to $10 million of borrowings under letter of credit obligations and up to $10 million of borrowings under swing-line loans, both sub-facilities of the revolving credit facility, which remained unchanged in this amendment.
In October 2003, the Company amended the Credit Agreement to provide for a new $130 million term loan, increase funds available under the letter of credit sub-facility to $15 million and extend the maturity date through October 2, 2008.
In July 2004, the Company amended the Credit Agreement to provide for increased flexibility under its financial covenants, increase funds available under the letter of credit sub-facility to $30 million and add a 25 basis point increase in the interest rate margin in the event of a downgrade in the Company’s credit rating. Since the amendment date, the Company has not had a downgrade in its credit rating. Additionally, as a result of the amendment, the Company incurred amendment fees of $258,000. These costs were deferred and are amortized using the effective interest method over the remaining term of the credit facility.
57
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
In November 2005, in connection with the acquisition of MHA, the Company amended and restated its existing credit facility. Our new credit facility, the Second Amended and Restated Credit Agreement (“New Credit Agreement”), provides for, among other things, a $75 million secured revolving credit facility, a $30 million letter of credit sub-facility, a $15 million swing-line sub-facility, all maturing in November 2010, and a new $205 million secured term loan facility maturing in November 2011. The new secured term loan facility was used to pay off existing borrowings of $87.8 million of term debt and provide financing for the acquisition. In connection with the pay off, the Company wrote off $1.2 million of deferred financing costs, which is recorded in interest expense.
The revolving credit facility portion of the New Credit Agreement carries an unused fee of between 0.5% and 0.375% per annum based on our current leverage ratio, and there are no mandatory reductions in the revolving commitment under the revolving credit facility. Borrowings under this revolving credit facility bear interest at floating rates based upon either a LIBOR or a prime interest rate option selected by us, plus a spread of 1.50% to 2.25% and 0.50% to 1.25%, respectively, to be determined based on our current leverage ratio. Amounts available under the Company’s revolving credit facility may be used for working capital, capital expenditures, permitted acquisitions and general corporate purposes, subject to various limitations.
The six year, $205 million term loan portion of our New Credit Agreement is subject to quarterly amortization of principal, with an amount equal to 1.25% of the initial aggregate principal amount of the facility payable quarterly through September 30, 2007 (except in the case of the initial quarterly payment on June 30, 2006 of 2.5%) and 2.5% of the initial aggregate principal amount of the facility payable quarterly from December 31, 2007 through September 30, 2010 with any remaining amounts payable in 2011. These quarterly payments begin on June 30, 2006 with an initial payment of $5.1 million. Voluntary prepayments of the term loan portion of the credit facility are applied as we may elect, including ratably to the remaining quarterly amortization payments. Borrowings under this term loan facility bear interest at floating rates based upon either a LIBOR or a prime interest rate option selected by us, plus a spread of 1.75% or 2.00% and 0.75% or 1.00%, respectively, to be determined based on our current leverage ratio.
In October 2003, September 2004 and October 2005, the Company established standby letters of credit of $3.7 million, $2.9 million and $2.4 million, respectively, as collateral in relation to its workers compensation insurance agreement. In September 2004 and December 2004, the Company established standby letters of credit of $0.1 million and $0.5 million, respectively, as collateral in relation to its professional liability insurance agreement. Each of these letters of credit bears interest at a fixed rate of 1.50% to 2.25% based on the Company’s leverage ratio. Total outstanding standby letters of credit at December 31, 2005 and 2004 was $9.6 million and $7.2 million, respectively.
58
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
Notes payable balances as of December 31, 2005 and 2004 consisted of the following:
| December 31, |
||||||||
| 2005 |
2004 |
|||||||
| $205,000,000 Term Loan due September 30, 2011 with variable interest rates. The weighted average interest rate at December 31, 2005 and 2004 was 6.4% and 5.2%, respectively |
$ | 205,000 | $ | 101,723 | ||||
| Less current portion of notes payable |
(10,250 | ) | (4,863 | ) | ||||
| Long-term portion of notes payable |
$ | 194,750 | $ | 96,860 | ||||
| Annual maturities of long-term debt are as follows (in thousands): |
||||||||
| 2006 |
$ | 10,250 | ||||||
| 2007 |
12,813 | |||||||
| 2008 |
20,500 | |||||||
| 2009 |
20,500 | |||||||
| 2010 |
46,125 | |||||||
| 2011 |
94,812 | |||||||
| $ | 205,000 | |||||||
The Company is required to make additional mandatory prepayments on the term loan with the proceeds of asset dispositions, extraordinary receipts, debt issuances and certain equity issuances. The Company is also required to make mandatory prepayments on the term loan within ninety days after the end of each fiscal year, commencing with the fiscal year ended December 31, 2006 in an amount equal to 50% of our excess cash flow (as defined in the New Credit Agreement), less any voluntary prepayments made during the fiscal year. These mandatory prepayment amounts, if any, are applied ratably to the remaining quarterly amortization payments.
The Company’s outstanding debt instruments at December 31, 2005 and 2004 were secured by all assets of the Company and the common stock of its subsidiaries. The Company’s New Credit Agreement contains various financial ratio covenants, including a minimum fixed charge coverage ratio and maximum leverage ratio, as well as restrictions on assumption of additional indebtedness, declaration of dividends, dispositions of assets, consolidation into another entity, capital expenditures in excess of specified amounts and allowable investments.
The Company is required to maintain interest rate protection on at least 50% of the term loan portion of its New Credit Agreement beginning May 2006 until November 2008. In October 2003, the Company entered into an interest rate swap agreement to minimize exposure to interest rate fluctuations on $30 million of its outstanding variable rate debt under the existing credit facility whereby the Company pays a fixed rate of 2.65% and receives a floating three-month LIBOR. This agreement expires in September 2006, and no initial investment was made to enter into this agreement. In June 2005, the Company entered into two additional interest rate swap agreements. The first agreement has a notional amount of $20 million and became effective in September 2005, whereby the Company pays a fixed rate of 3.99% and receives a floating three-month LIBOR. The agreement expires in March 2007. The second agreement will become effective in September 2006, with a notional amount of $15 million whereby the Company pays a fixed rate of 4.09% and receives a floating three-month LIBOR. This agreement will expire in September 2007. In November 2005, the Company entered into five additional interest rate swap agreements for notional amounts of $15 million, $10 million, $30 million, $35 million and $50 million, whereby the Company pays a fixed rate of 4.82%, 4.95%, 4.87%, 4.94%, and 4.97%, respectively, and receives a floating three-month LIBOR. These agreements expire in December 2007, June 2008, December
59
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
2008, December 2009 and December 2010, respectively. At December 31, 2005 and 2004, the interest rate swap agreements had a fair value of ($0.1) million and $0.7 million, respectively, which is included in other assets and liabilities in the accompanying consolidated balance sheets. The Company has formally documented the hedging relationships and accounts for these arrangements as cash flow hedges.
(8) Retirement Plans
The Company maintains the Healthcare Staffing Retirement Savings Plan (the AMN Plan), a plan that complies with the Internal Revenue Code Section (IRC) 401(k) provisions. The AMN Plan covers all employees that meet certain age and other eligibility requirements. An annual discretionary matching contribution is determined by the Compensation and Stock Plan Committee of the Board of Directors each year and may be up to a maximum 6% of eligible compensation paid to all participants during the plan year. The amount of the employer contributions were $2,341,000, $2,204,000, and $2,982,000 for the years ended December 31, 2005, 2004 and 2003, respectively. In 2005, the Company applied $951,000 of outstanding 401(k) forfeiture balances under the AMN Plan against current employer match contributions of $2,341,000, thereby reducing the Company’s recognized contributions for the year.
In January 2002, the Company established the Executive Nonqualified Excess Plan of AMN Healthcare, Inc. The Executive Nonqualified Excess Plan is not intended to be tax qualified and is an unfunded plan. This plan is primarily composed of deferred compensation and all related income and losses attributable thereto. Discretionary matching contributions to the plan are made that vest incrementally so that the employee is fully vested in the match following five years of employment with the Company. The Company established the 2005 Amended and Restated Executive Nonqualified Excess Plan effective January 1, 2005, to comply with newly enacted legislation. The Company amended the 2005 Amended and Restated Executive Nonqualified Excess Plan effective November 1, 2005. The 2005 Amended and Restated Executive Nonqualified Excess Plan provides discretion to the Compensation and Stock Plan Committee in determining an employee’s eligibility for participation in the plan and increased plan participation eligibility to include additional key employees. Eligible compensation was increased to 80% of an employee’s base salary and 100% of an employee’s bonus. Investment options are determined based on an underlying private placement insurance contract. An annual discretionary matching contribution is determined by the Compensation and Stock Plan Committee of the Board of Directors each year. The amount of the employer contributions was $69,000, $65,000 and $54,000 for the years ended December 31, 2005, 2004 and 2003, respectively.
(9) Stockholders’ Equity
(a) Stock Option Plans
In July 2001, the 2001 Stock Option Plan was established to provide a means to attract and retain employees. In May 2004, the 2001 Stock Option Plan was renamed the Stock Option Plan, and an additional 2,000,000 options were authorized for issuance to increase the maximum number of options to be granted under the plan to 4,178,000. Subject to certain conditions, unless the plan is otherwise modified, a maximum of 544,500 options may be granted to any one person in any calendar year. Exercise prices will be determined at the time of grant and will be no less than fair market value of the underlying common stock on the date of grant. Unless otherwise provided at the time of the grant, the options shall vest and become exercisable in increments of 25% on each of the first four anniversaries of the date of grant. The plan expires on the tenth anniversary of the effective date. At December 31, 2005 and 2004, respectively, 356,001 and 1,282,126 shares of common stock were reserved for future grants related to the Stock Option Plan.
60
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
In November 1999, the Company established two performance stock option plans (the 1999 Plans) to provide for the grant of options to the Company’s upper management. Options for a maximum of 4,040,000 shares of common stock were authorized at an exercise price of $3.80 per option for grants within 120 days of the 1999 Recapitalization and not less than the fair market value in the case of subsequent grants. During 2000, options for an additional 1,493,000 shares were reserved under the 1999 Plans. At December 31, 2005 and 2004, 351,274 shares of common stock were reserved for future grants related to the 1999 Plans. Options under the 1999 Plans began vesting at 25% per year beginning in the year 2000 provided certain earnings performance criteria were met and the grantee remained an employee. If the Company did not meet the performance criteria for a particular year, the portion of the option which was eligible to become vested terminated. Pursuant to the amended provisions of the 1999 Plans, all options previously granted under the 1999 Plans became fully vested upon the November 2001 common stock offering and at December 31, 2005 are fully exercisable. All previously granted options under the 1999 Plans expire in 2009.
In accordance with the provisions of SFAS No. 123, the Company applies APB Opinion No. 25 and related interpretations in accounting for its 1999 Plans and the Stock Option Plan. Accordingly, because the 1999 Plans were performance-based and certain grants under the Stock Option Plan were granted at less than fair market value, the Company recorded compensation expense of $142,000 in 2005, $750,000 in 2004 and $874,000 in 2003. Additionally, in 2003, the Company recorded compensation expense of $1,128,000 associated with the settlement of options in the tender offer, which is included in selling, general and administrative expenses in the accompanying consolidated statements of operations. See Note 3.
A summary of stock option activity under the 1999 Plans and the Stock Option Plan are as follows:
| 1999 Plans |
Stock Option Plan | |||||||||||
| Options Outstanding |
Weighted- Average Exercise Price |
Options Outstanding |
Weighted- Average Exercise Price | |||||||||
| Outstanding at December 31, 2002 |
4,578,000 | $ | 4.65 | 1,204,000 | $ | 16.93 | ||||||
| Granted |
— | — | 777,000 | 9.68 | ||||||||
| Exercised (1) |
(316,000 | ) | 3.80 | (66,000 | ) | 9.38 | ||||||
| Canceled |
— | — | (14,000 | ) | 22.62 | |||||||
| Outstanding at December 31, 2003 |
4,262,000 | $ | 4.71 | 1,901,000 | $ | 14.19 | ||||||
| Granted |
— | — | 1,079,000 | 14.56 | ||||||||
| Exercised |
— | — | (224,000 | ) | 9.13 | |||||||
| Canceled |
— | — | (248,000 | ) | 12.62 | |||||||
| Outstanding at December 31, 2004 |
4,262,000 | $ | 4.71 | 2,508,000 | $ | 14.96 | ||||||
| Granted |
— | — | 987,000 | 14.95 | ||||||||
| Exercised |
(440,000 | ) | 4.52 | (86,000 | ) | 10.14 | ||||||
| Canceled |
— | — | (60,000 | ) | 16.19 | |||||||
| Outstanding at December 31, 2005 |
3,822,000 | $ | 4.73 | 3,349,000 | $ | 15.06 | ||||||
| Exercisable at December 31, 2005 |
3,822,000 | $ | 4.73 | 1,100,000 | $ | 16.10 | ||||||
(1) Includes 376,000 options at a weighted average exercise price of $4.70 purchased in connection with the self-tender offer in October 2003.
61
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
The following table summarizes options outstanding and exercisable as of December 31, 2005:
| Options Outstanding |
Options Exercisable | |||||||||||||
| Range Of Exercise Price |
Number Outstanding |
Weighted- Average Remaining Contractual Life (Years) |
Weighted- Average Exercise Price |
Number Outstanding |
Weighted- Average Remaining Contractual Life (Years) |
Weighted- Average Exercise Price | ||||||||
| 1999 Plans |
$ 3.80 | 2,588,000 | 4 | $ 3.80 | 2,588,000 | 4 | $ 3.80 | |||||||
| 6.68 | 1,234,000 | 5 | 6.68 | 1,234,000 | 5 | 6.68 | ||||||||
| 3,822,000 | 3,822,000 | |||||||||||||
| Stock Option Plan |
$ 6.89 - $ 9.19 | 34,000 | 6 | $ 9.09 | 34,000 | 6 | $ 9.09 | |||||||
| 9.20 - 11.49 | 628,000 | 7 | 9.68 | 300,000 | 7 | 9.68 | ||||||||
| 11.50 - 13.79 | 210,000 | 8 | 12.10 | 97,000 | 7 | 12.02 | ||||||||
| 13.80 - 16.08 | 1,908,000 | 9 | 14.94 | 245,000 | 8 | 14.94 | ||||||||
| 16.09 - 18.38 | 3,000 | 9 | 16.32 | 1,000 | 9 | 16.32 | ||||||||
| 20.69 - 22.98 | 566,000 | 6 | 22.85 | 423,000 | 6 | 22.85 | ||||||||
| 3,349,000 | 1,100,000 | |||||||||||||
(b) Stock Repurchase Program
In November 2002, the Company’s board of directors approved a stock repurchase program authorizing a repurchase of up to $100 million of the Company’s common stock on the open market at prevailing market prices from time to time through December 2003. Stock repurchases are subject to prevailing market conditions and other considerations, including limitations under applicable securities laws. Under the terms of the program, the Company repurchased 5,154,200 shares at an average purchase price of $14.29 per share, or an aggregate of $73.7 million. As of December 31, 2005, there were no authorized stock repurchase programs.
(10) Related Party Transactions
(a) Majority stockholder
During 2004 and 2003, the Company paid an affiliate of the controlling stockholders $10,000 and $30,000, respectively, for out of pocket expenses related to meetings of the Board of Directors, which is included in selling, general and administrative expenses in the accompanying consolidated statements of operations.
The Company completed secondary offerings of its common stock for 2,300,000 and 10,631,303 shares on April 18, 2005 and May 27, 2005, respectively. All of the 12,931,303 shares were sold by affiliates of Haas Wheat & Partners, L.P., a private equity investment firm whose affiliates had owned shares of the company since 1999. Robert B. Haas, who exercised sole voting and dispositive power over the 12,931,303 shares by virtue of his control over Haas Wheat & Partners, L.P. and its affiliates, served as the Chairman of the Company’s Board of Directors until May 4, 2005. The Company’s Presiding Director, Douglas D. Wheat, serves as President of Haas Wheat & Partners, L.P.
(b) Minority stockholders
During 2005, a family member of MHA received a non-interest bearing loan of $55,000 prior to the acquisition date, of which $16,000 is included in other current assets in the accompanying consolidated balance sheet for the year ended December 31, 2005.
62
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
(11) Commitments and Contingencies
(a) Legal
The Company is subject to various claims and legal actions in the ordinary course of business. Some of these matters include payroll and employee-related matters and investigations by governmental agencies regarding employment practices. As the Company becomes aware of such claims and legal actions, the Company provides accruals if the exposures are probable and estimable. If an adverse outcome of such claims and legal actions is reasonably possible, the Company assesses materiality and provides disclosure, as appropriate. The Company may also become subject to claims, governmental inquiries and investigations and legal actions relating to services provided by the Company’s temporary healthcare professionals, and maintain accruals for these matters if the amounts are probable and estimable. The Company is currently not aware of any such pending or threatened litigation that would be considered reasonably likely to have a material adverse effect on the Company’s consolidated financial position, results of operations or liquidity.
(b) Leases
The Company leases certain office facilities and equipment under various operating and capital leases over the next five years and thereafter. Future minimum lease payments under noncancelable operating leases (with initial or remaining lease terms in excess of one year) and future minimum capital lease payments as of December 31, 2005 are as follows (in thousands):
| Capital Leases |
Operating Leases | ||||||
| Years ending December 31: |
|||||||
| 2006 |
$ | 494 | $ | 16,327 | |||
| 2007 |
493 | 17,820 | |||||
| 2008 |
479 | 17,417 | |||||
| 2009 |
464 | 17,389 | |||||
| 2010 |
158 | 17,149 | |||||
| Thereafter |
— | 85,102 | |||||
| Total minimum lease payments |
$ | 2,088 | $ | 171,204 | |||
| Less amount representing interest (at rates ranging from 3.20% to 12.75%) |
(190 | ) | |||||
| Present value of minimum lease payments |
1,898 | ||||||
| Less current installments of obligations under capital leases |
(417 | ) | |||||
| Obligations under capital leases, excluding current installments |
$ | 1,481 | |||||
Fixed assets obtained through capital leases as of December 31, 2005 and 2004 are as follows (in thousands):
| December 31, |
||||||||
| 2005 |
2004 |
|||||||
| Fixed assets |
$ | 2,203 | $ | 1,634 | ||||
| Accumulated amortization |
(400 | ) | (820 | ) | ||||
| Fixed assets, net |
$ | 1,803 | $ | 814 | ||||
63
Table of Contents
AMN HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS – (Continued)
Obligations under capital leases are included in other current and other long-term liabilities in the accompanying financial statements. Rent expense was $11,839,000, $10,682,000, and $8,295,000 for the years ended December 31, 2005, 2004 and 2003, respectively.
(12) Quarterly Financial Data (Unaudited)
| Year Ended December 31, 2005 | |||||||||||||||
| First Quarter |
Second Quarter |
Third Quarter |
Fourth Quarter |
Total Year | |||||||||||
| (In thousands, except per share data) | |||||||||||||||
| Revenue |
$ | 156,842 | $ | 160,689 | $ | 166,883 | $ | 221,429 | $ | 705,843 | |||||
| Gross profit |
$ | 35,717 | $ | 37,168 | $ | 39,544 | $ | 57,806 | $ | 170,235 | |||||
| Net income |
$ | 3,993 | $ | 4,416 | $ | 6,848 | $ | 6,977 | $ | 22,234 | |||||
| Net income per share: |
|||||||||||||||
| Basic |
$ | 0.14 | $ | 0.15 | $ | 0.24 | $ | 0.23 | $ | 0.76 | |||||
| Diluted |
$ | 0.13 | $ | 0.14 | $ | 0.22 | $ | 0.21 | $ | 0.69 | |||||
| Year Ended December 31, 2004 | |||||||||||||||
| First Quarter |
Second Quarter |
Third Quarter |
Fourth Quarter(a) |
Total Year | |||||||||||
| (In thousands, except per share data) | |||||||||||||||
| Revenue |
$ | 161,265 | $ | 153,368 | $ | 156,083 | $ | 158,300 | $ | 629,016 | |||||
| Gross profit |
$ | 35,829 | $ | 34,982 | $ | 36,700 | $ | 36,851 | $ | 144,362 | |||||
| Net income |
$ | 4,559 | $ | 4,323 | $ | 3,930 | $ | 4,534 | $ | 17,346 | |||||
| Net income per share: |
|||||||||||||||
| Basic |
$ | 0.16 | $ | 0.15 | $ | 0.14 | $ | 0.16 | $ | 0.61 | |||||
| Diluted |
$ | 0.15 | $ | 0.14 | $ | 0.13 | $ | 0.14 | $ | 0.55 | |||||
64
Table of Contents
Item 9. Changes In and Disagreements With Accountants on Accounting and Financial Disclosure
None.
Item 9A. Controls and Procedures
(1) Evaluation of Disclosure Controls and Procedures
We carried out an evaluation, under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, of the effectiveness of our disclosure controls and procedures, as defined in Rules 13a-15(e) and 15d-15(e) of the Securities Exchange Act of 1934. Based on that evaluation, our Chief Executive Officer and Chief Financial Officer have concluded that our disclosure controls and procedures as of December 31, 2005 were effective to ensure that information required to be disclosed by us in reports that we file or submit under the Securities Exchange Act of 1934 is recorded, processed, summarized and reported within the time periods specified in the Securities and Exchange Commission’s rules and forms.
(2) Management’s Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Exchange Act Rules 13a-15(f). Under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting based on the framework in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate. Based on our evaluation under the framework in Internal Control—Integrated Framework, our management concluded that our internal control over financial reporting was effective as of December 31, 2005.
We acquired The MHA Group, Inc. and Subsidiaries (the “acquired entity”) during 2005. Management excluded from its assessment of the effectiveness of our internal control over financial reporting as of December 31, 2005, the acquired entity’s internal control over financing reporting associated with total consolidated assets of $72.5 million and total revenue of $53.3 million included in the consolidated financial statements of the Company and our subsidiaries as of and for the year ended December 31, 2005.
Our management’s assessment of the effectiveness of our internal control over financial reporting as of December 31, 2005 has been audited by KPMG LLP, an independent registered public accounting firm, as stated in their report which is included herein.
(3) Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting that occurred during the quarter ended December 31, 2005 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
65
Table of Contents
(4) Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders
AMN Healthcare Services, Inc.:
We have audited management’s assessment, included in the accompanying Management’s Annual Report on Internal Control Over Financial Reporting (Item 9A.(2)), that AMN Healthcare Services, Inc. and subsidiaries (the Company) maintained effective internal control over financial reporting as of December 31, 2005, based on criteria established in Internal Control–Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). AMN Healthcare Services, Inc.’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting. Our responsibility is to express an opinion on management’s assessment and an opinion on the effectiveness of the Company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, evaluating management’s assessment, testing and evaluating the design and operating effectiveness of internal control, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, management’s assessment that AMN Healthcare Services, Inc. and subsidiaries maintained effective internal control over financial reporting as of December 31, 2005, is fairly stated, in all material respects, based on criteria established in Internal Control–Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Also, in our opinion, AMN Healthcare Services, Inc. maintained, in all material respects, effective internal control over financial reporting as of December 31, 2005, based on criteria established in Internal Control–Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO).
The Company acquired The MHA Group, Inc. and subsidiaries (the “acquired entity”) during 2005, and management excluded from its assessment of the effectiveness of the Company’s internal control over financial reporting as of December 31, 2005, the acquired entity’s internal control over financial reporting associated with total assets of $73.5 million and total revenues of $53.3 million included in the consolidated financial statements of the Company as of and for the year ended December 31, 2005. Our audit of internal control over financial
66
Table of Contents
reporting of the Company also excluded an evaluation of the internal control over financial reporting of the acquired entity.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of AMN Healthcare Services, Inc. and subsidiaries as of December 31, 2005 and 2004, and the related consolidated statements of operations, stockholders’ equity and comprehensive income, and cash flows for each of the years in the three-year period ended December 31, 2005, and our report dated March 9, 2006 expressed an unqualified opinion on those consolidated financial statements.
/s/ KPMG LLP
San Diego, California
March 9, 2006
None.
67
Table of Contents
PART III
Item 10. Directors and Executive Officers of the Registrant
Information required by this item, other than the following information concerning our Code of Ethics for Senior Financial Officers, is incorporated by reference to the Proxy Statement under the headings “Nominees for the Board of Directors” and “Non-Director Executive Officers” to be distributed in connection with our Annual Meeting of Stockholders to be held on April 12, 2006.
We have adopted a Code of Ethics for Senior Financial Officers that applies to our principal executive officer, principal financial officer, principal accounting officer or any person performing similar functions, which is posted on our website at www.amnhealthcare.com/investors. We intend to publish any amendment to, or waiver from, the Code of Ethics for Senior Financial Officers on our website.
Item 11. Executive Compensation
Information required by this item is incorporated by reference to the Proxy Statement under the heading “Executive Compensation and Related Information” to be distributed in connection with our Annual Meeting of Stockholders to be held on April 12, 2006.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
Information required by this item is incorporated by reference to the Proxy Statement under the heading “Security Ownership of Certain Beneficial Owners and Management” to be distributed in connection with our Annual Meeting of Stockholders to be held on April 12, 2006.
Item 13. Certain Relationships and Related Transactions
Information required by this item is incorporated by reference to the Proxy Statement under the heading “Certain Relationships and Related Transactions” to be distributed in connection with our Annual Meeting of Stockholders to be held on April 12, 2006.
Item 14. Principal Accountant Fees and Services
Information required by this item is incorporated by reference to the Proxy Statement under the heading “Independent Registered Public Accounting Firm” to be distributed in connection with our Annual Meeting of Stockholders to be held on April 12, 2006.
68
Table of Contents
PART IV
Item 15. Exhibits and Financial Statement Schedules
(a) Documents filed as part of the report.
| (1) Consolidated Financial Statements |
| Report of Independent Registered Public Accounting Firm |
| Consolidated Balance Sheets |
| Consolidated Statements of Operations |
| Consolidated Statements of Stockholders’ Equity and Comprehensive Income |
| Consolidated Statements of Cash Flows |
| Notes to Consolidated Financial Statements |
| (2) Financial Statement Schedules |
| Schedule II—Valuation and Qualifying Accounts |
| (3) Exhibits |
| Exhibit Number |
Description | |
| 2.1 | Acquisition Agreement, dated as of October 5, 2005, by and among AMN Healthcare Services, Inc., Cowboy Acquisition Corp., The MHA Group, Inc. and James C. Merritt and Joseph E. Hawkins (incorporated by reference to the exhibits filed with the Registrant’s Current Report on Form 8-K filed on October 6, 2005). | |
| 2.2 | Amendment No. 1 to Acquisition Agreement, dated as of October 21, 2005, by and among AMN Healthcare Services, Inc., Cowboy Acquisition Corp., The MHA Group, Inc. and James C. Merritt and Joseph E. Hawkins (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2005). | |
| 2.3 | Amendment No. 2 to Acquisition Agreement, dated as of October 21, 2005, by and among AMN Healthcare Services, Inc., Cowboy Acquisition Corp., The MHA Group, Inc. and James C. Merritt and Joseph E. Hawkins (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2005). | |
| 3.1 | Amended and Restated Certificate of Incorporation of AMN Healthcare Services, Inc.*** | |
| 3.3 | Second Amended and Restated By-laws of AMN Healthcare Services, Inc. (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2005). | |
| 4.1 | Specimen Stock Certificate.*** | |
| 4.2 | Registration Rights Agreement, dated as of November 16, 2001, among the Registrant, HWH Capital Partners, L.P., HWH Nightingale Partners, L.P., HWP Nightingale Partners II, L.P., HWP Capital Partners II, L.P., BancAmerica Capital Investors SBIC I, L.P., the Francis Family Trust dated May 24, 1996 and Steven Francis.*** | |
| 4.3 | Amendment No. 1 to the Registration Rights Agreement dated November 16, 2001, dated April 18, 2005 (incorporated by reference to the exhibits filed with the Registrant’s Current Report on Form 8-K filed on April 22, 2005). | |
| 4.4 | Amended and Restated Registration Rights Agreement, dated as of November 2, 2005, among AMN Healthcare Services, Inc., Steven Francis, the Francis Family Trust dated May 24, 1996, James C. Merritt and Joseph E. Hawkins (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2005). | |
69
Table of Contents
| 4.5 | Second Amended and Restated Credit Agreement by and among Bank of America, N.A., AMN Healthcare, Inc., as borrower, AMN Healthcare Services, Inc., AMN Services, Inc., O’Grady-Peyton International (USA), Inc., International Healthcare Recruiters, Inc. and AMN Staffing Services, Inc., The MHA Group Inc., Merritt, Hawkins & Associates, Med Travelers, Inc., RN Demand, Inc., MHA Allied Consulting, Inc., as guarantors, dated November 2, 2005 (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2005). | |
| 10.1 | Office Lease, dated as of April 2, 2002, between Kilroy Realty, L.P. and AMN Healthcare, Inc.**** | |
| 10.2 | AMN Holdings, Inc. 1999 Performance Stock Option Plan, as amended. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.3 | AMN Holdings, Inc. 1999 Super-Performance Stock Option Plan, as amended. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.4 | AMN Healthcare Services, Inc. 2001 Stock Option Plan. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.5 | 1999 Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, between the Registrant and Steven Francis. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.6 | Amendment, dated as of December 13, 2000, to the 1999 Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, between the Registrant and Steven Francis. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.7 | Amendment No. 2, dated as of July 24, 2001, to the 1999 Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, as amended December 13, 2000, between the Registrant and Steven Francis. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.8 | 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, between the Registrant and Steven Francis. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.9 | Amendment, dated as of December 13, 2000, to the Super-Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, between the Registrant and Steven Francis. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.10 | Amendment No. 2, dated as of July 24, 2001, to the 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, as amended December 13, 2000, between the Registrant and Steven Francis. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.11 | 1999 Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.12 | Amendment, dated as of December 13, 2000, to the 1999 Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.13 | Amendment No. 2, dated as of July 24, 2001, to the 1999 Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, as amended December 13, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.14 | 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
70
Table of Contents
| 10.15 | Amendment, dated as of December 13, 2000, to the Super-Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.16 | Amendment No. 2, dated as of July 24, 2001, to the 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of November 19, 1999, as amended December 13, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.17 | 1999 Performance Stock Option Plan Stock Option Agreement, dated as of November 20, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.18 | Amendment, dated as of July 24, 2001, to the 1999 Performance Stock Option Plan Stock Option Agreement, dated as of November 20, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.19 | 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of November 20, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.20 | Amendment, dated as of July 24, 2001, to the 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of November 20, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.21 | 1999 Performance Stock Option Plan Stock Option Agreement, dated as of December 13, 2000, between the Registrant and Steven Francis.** | |
| 10.22 | Amendment, dated as of July 24, 2001, to the 1999 Performance Stock Option Plan Stock Option Agreement, dated as of December 13, 2000, between the Registrant and Steven Francis. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.23 | 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of December 13, 2000, between the Registrant and Steven Francis. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.24 | Amendment, dated as of July 24, 2001, to the 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of December 13, 2000, between the Registrant and Steven Francis. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.25 | 1999 Performance Stock Option Plan Stock Option Agreement, dated as of December 13, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.26 | Amendment, dated as of July 24, 2001, to the 1999 Performance Stock Option Plan Stock Option Agreement, dated as of December 13, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.27 | 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of December 13, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.28 | Amendment, dated as of July 24, 2001, to the 1999 Super-Performance Stock Option Plan Stock Option Agreement, dated as of December 13, 2000, between the Registrant and Susan Nowakowski. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.29 | 2001 Stock Option Plan Stock Option Agreement, dated as of May 21, 2001, between the Registrant and Donald Myll.** | |
71
Table of Contents
| 10.30 | AMN Healthcare Services, Inc. 2001 Senior Management Bonus Plan. (Management Contract or Compensatory Plan or Arrangement)** | |
| 10.31 | AMN Healthcare, Inc. Executive Nonqualified Excess Plan (Management Contract or Compensatory Plan or Arrangement).**** | |
| 10.32 | Amendment to AMN Healthcare, Inc. Executive Nonqualified Excess Plan, dated as of January 1, 2002 (Management Contract or Compensatory Plan or Arrangement).**** | |
| 10.33 | 2001 Stock Option Plan Stock Option Agreement, dated as of January 17, 2002, between the Registrant and Steven Francis (Management Contract or Compensatory Plan or Arrangement).**** | |
| 10.34 | 2001 Stock Option Plan Stock Option Agreement, dated as of January 17, 2002, between the Registrant and Susan Nowakowski (Management Contract or Compensatory Plan or Arrangement).**** | |
| 10.35 | 2001 Stock Option Plan Stock Option Agreement, dated as of January 17, 2002, between the Registrant and William Miller (Management Contract or Compensatory Plan or Arrangement).**** | |
| 10.36 | 2001 Stock Option Plan Stock Option Agreement, dated as of January 17, 2002, between the Registrant and Andrew Stern (Management Contract or Compensatory Plan or Arrangement).**** | |
| 10.37 | Executive Severance Agreement between AMN Healthcare, Inc. and David C. Dreyer, dated September 20, 2004 (Management Contract or Compensatory Plan or Arrangement) (incorporated by reference to the exhibit filed with the Registrant’s Current Report on Form 8-K dated September 16, 2004). | |
| 10.38 | Stock Option Plan (incorporated herein by reference to the Registrant’s Proxy Statement, Schedule 14A filed with the Commission on April 14, 2004 (SEC File No. 1-16753)). | |
| 10.39 | Stock Option Plan Stock Option Agreement, dated as of May 18, 2004, between the Registrant and Andrew M. Stern (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.40 | Stock Option Plan Stock Option Agreement, dated as of May 18, 2004, between the Registrant and William F. Miller III (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.41 | Stock Option Plan Stock Option Agreement, dated as of May 18, 2004, between the Registrant and Kenneth F. Yontz (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.42 | Stock Option Plan Stock Option Agreement, dated as of May 18, 2004, between the Registrant and Steven C. Francis (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.43 | Stock Option Plan Stock Option Agreement, dated as of May 18, 2004, between the Registrant and Susan R. Nowakowski (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.44 | Stock Option Plan Stock Option Agreement, dated as of May 18, 2004, between the Registrant and Denise L. Jackson (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.45 | Stock Option Plan Stock Option Agreement, dated as of September 20, 2004, between the Registrant and David C. Dreyer (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.46 | Executive Severance Agreement, dated as of December 20, 2002, between AMN Healthcare, Inc. and Denise L. Jackson (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.47 | Stock Option Plan Stock Option Agreement, dated as of July 24, 2001, between the Registrant and Denise L. Jackson (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.48 | Stock Option Plan Stock Option Agreement, dated as of January 17, 2002, between the Registrant and Denise L. Jackson (Management Contract or Compensatory Plan or Arrangement)***** | |
| 10.49 | Stock Option Plan Stock Option Agreement, dated as of May 8, 2003, between the Registrant and Denise L. Jackson (Management Contract or Compensatory Plan or Arrangement)***** | |
72
Table of Contents
| 10.50 | Employment Agreement, dated as of May 4, 2005, between AMN Healthcare, Inc. and Steven C. Francis. (Management Contract or Compensatory Plan or Arrangement) (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2005). | |
| 10.51 | Employment Agreement, dated as of May 4, 2005, between AMN Healthcare, Inc. and Susan R. Nowakowski. (Management Contract or Compensatory Plan or Arrangement) (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2005). | |
| 10.52 | Executive Severance Agreement, dated as of May 4, 2005, between AMN Healthcare, Inc. and Denise L. Jackson. (Management Contract or Compensatory Plan or Arrangement) (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2005). | |
| 10.53 | Executive Severance Agreement, dated as of May 4, 2005, between AMN Healthcare, Inc. and David C. Dreyer. (Management Contract or Compensatory Plan or Arrangement) (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2005). | |
| 10.54 | Form of Stock Option Plan Stock Option Agreement (Management Contract or Compensatory Plan or Arrangement) (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2005). | |
| 10.55 | Stock Option Plan Stock Option Agreement, dated as of September 28, 2005, between the Registrant and Steven C. Francis (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2005). | |
| 10.56 | Stock Option Plan Stock Option Agreement, dated as of September 28, 2005, between the Registrant and Douglas D. Wheat (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2005). | |
| 10.57 | Stock Option Plan Stock Option Agreement, dated as of September 28, 2005, between the Registrant and R. Jeffrey Harris (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2005). | |
| 10.58 | Form of Indemnification Agreement (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2005). | |
| 10.59 | The 2005 Amended and Restated Executive Nonqualified Excess Plan of AMN Healthcare, Inc. (incorporated by reference to the exhibits filed with the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2005). | |
| 10.60 | Amendment, dated as of March 8, 2006, to the Executive Severance Agreement, dated as of May 4, 2005, between AMN Healthcare, Inc. and Denise L. Jackson (Management Contract or Compensatory Plan or Arrangement).* | |
| 10.61 | Amendment, dated as of March 8, 2006, to the Executive Severance Agreement, dated as of May 4, 2005, between AMN Healthcare, Inc. and David C. Dreyer (Management Contract or Compensatory Plan or Arrangement).* | |
| 21.1 | Subsidiaries of the Registrant.* | |
| 23.1 | Report and Consent of Independent Registered Public Accounting Firm.* | |
| 31.1 | Certification by Susan R. Nowakowski pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934* | |
| 31.2 | Certification by David C. Dreyer pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934* | |
| 32.1 | Certification by Susan R. Nowakowski pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002* | |
| 32.2 | Certification by David C. Dreyer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002* | |
73
Table of Contents
| * | Filed herewith. |
| ** | Incorporated by reference to the exhibits filed with the Registrant’s Registration Statement on Form S-1 (File No. 333-65168). |
| *** | Incorporated by reference to the exhibits filed with the Registrant’s Annual Report on Form 10-K for the fiscal year ended December 31, 2001. |
| **** | Incorporated by reference to the exhibits filed with the Registrant’s Registration Statement on Form S-1 (File No. 333-86952). |
| ***** | Incorporated by reference to the exhibits filed with the Registrant’s Annual Report on Form 10-K for the fiscal year ended December 31, 2004. |
74
Table of Contents
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
| AMN HEALTHCARE SERVICES, INC. | ||
| /s/ SUSAN R. NOWAKOWSKI | ||
| Susan R. Nowakowski President and Chief Executive Officer | ||
Date: March 10, 2006
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed by the following persons in the capacities indicated and on the 10th day of March, 2006.
| /s/ SUSAN R. NOWAKOWSKI Susan R. Nowakowski Director, President and Chief Executive Officer |
| /s/ STEVEN C. FRANCIS Steven C. Francis Director and Executive Chairman of the Board |
| /s/ WILLIAM F. MILLER III William F. Miller III Director |
| /s/ ANDREW M. STERN Andrew M. Stern Director |
| /s/ DOUGLAS D. WHEAT Douglas D. Wheat Director |
| /s/ KENNETH F. YONTZ Kenneth F. Yontz Director |
| /s/ R. JEFFREY HARRIS R. Jeffrey Harris Director |
| /s/ DAVID C. DREYER David C. Dreyer Chief Accounting Officer and Chief Financial Officer |
75
Table of Contents
Schedule II
AMN HEALTHCARE SERVICES, INC.
VALUATION AND QUALIFYING ACCOUNTS
For Years Ended December 31, 2005, 2004 and 2003
| Allowance for Doubtful Accounts |
Balance at the Beginning of Year |
Provision |
Deductions(*) |
Balance at End of Year | ||||||||||
| (in thousands) | ||||||||||||||
| Year ended December 31, 2003 |
$ | 4,310 | $ | (315 | ) | $ | (653 | ) | $ | 3,342 | ||||
| Year ended December 31, 2004 |
$ | 3,342 | $ | 173 | $ | (1,763 | ) | $ | 1,752 | |||||
| Year ended December 31, 2005 |
$ | 1,752 | $ | 1,738 | $ | (1,115 | ) | $ | 2,375 | |||||
| (*) | Accounts written off |
See accompanying report of independent registered public accounting firm.
76